
Abstract
Objective
To evaluate the effect of online follow-up on the quality of life of patients who undergo extraction of impacted mandibular third molars.
Materials and methods
This study enrolled patients with impacted mandibular third molars who were treated at the Department of Oral and Maxillofacial Surgery of the Stomatological Hospital at Southern Medical University and divided them into test and control groups. The test group received an online follow-up on the first, third, and fifth days after tooth extraction, while the control group was not followed up with. Patients in both groups were reexamined on the postoperative seventh day, completing the postoperative symptom severity (PoSSe) scale to comprehensively and quantitatively evaluate their quality of life after tooth extraction. A visual analogue scale (VAS) was used to evaluate the degree of approval for an online follow-up after tooth extraction by 20 senior doctors (≥ 40 years old) and 20 young doctors (<4 0 years old).
Results
The PoSSe scale scores of the remaining options in the test group were significantly lower than those in the control group. The VAS score of senior doctors for online follow-up was significantly lower than that of young doctors.
Conclusions
A postoperative online follow-up effectively improved the quality of life of patients who underwent extraction of impacted mandibular third molars. Compared with senior doctors, young doctors were more likely to approve an online follow-up after tooth extraction.
Clinical relevance
Online medical care can be considered as an auxiliary tool to improve the effect of oral treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
An impacted mandibular third molar is a commonly encountered condition in the Department of Oral and Maxillofacial Surgery, and it is mainly treated by surgical extraction [1,2,3]. Because the operation often necessitates cutting the gum and removing the bone, tooth extraction often affects the patients’ eating, speaking, and feeling, causing pain, swelling, and bleeding, which seriously affects their quality of life [4].
To date, all aspects of the improvement related to impacted mandibular third molar extraction have mainly been focused on the steps during the diagnosis and treatment [5,6,7,8,9,10,11,12,13,14,15,16,17]. However, reports on the postoperative follow-up care of patients after returning home are rare and limited to telephone follow-up [18,19,20]. Traditional postoperative follow-up via telephone has proven to be effective [20], and it has effects such as reducing the cost of consultation compared with conventional on-site follow-up [19]. However, in clinical practice, we have also found that telephone follow-up greatly increases the time consumption of doctors and nurses, as they have to repeat the same instructions or guidelines, and patients often reject the calls, as they think that these unknown incoming calls are harassing calls.
The increase in online medical care facilitates patients’ access to medical services and also enables doctors to manage their cases more efficiently and follow up with their registered patients quickly and accurately to obtain important clinical data [21, 22]. This study used the Good Doctor Online mobile app as an example, through which the doctors followed up with the registered patients after tooth extraction. As a questionnaire with good reliability and validity, the PoSSe scale was used to evaluate the quality of life of patients after operation [23].
The primary aim of the present study was to evaluate the effectiveness of postoperative online follow-up on patients’ quality of life following impacted madibular third molar removal. A further objective was to investigate the application value of online medical care in the field of oral therapy.
Materials and methods
Study design
The study was a prospective, randomized, double-blind clinical trial. No changes to trial design were made during the study. The report of the methodology used in the study conforms with the CONSORT Statement [24].
Participants
Patients with impacted mandibular third molars treated at the Department of Oral and Maxillofacial Surgery of the Stomatological Hospital at Southern Medical University from June 2019 to December 2019 were enrolled in the study. All patients were informed about the procedure and signed a consent form. The basic information of patients was collected, and a cone beam CT (CBCT) was taken before operation. Two observers who were not involved in the follow-up of research subjects evaluated the CBCT independently to make a judgment on the position of the third molar, Pell and Gregory classification, Winter classification, and the alveolar nerve canal [25]. Two training sessions were organized prior to the final observations for calibration of the observers.
Inclusion criteria
The included subjects were healthy patients aged 18–45 years with an indication of extraction of impacted mandibular third molars. All of them received the first extraction operation; they had no history of systematic disease such as high blood pressure, diabetes, or heart disease; and they had good medical compliance and were able to return on time.
Exclusion criteria
The excluded patients had contraindications of tooth extraction, local or systemic infection within 4 weeks before tooth extraction, smoking, poor oral hygiene, severe periodontitis, being pregnant or lactating, or having basic diseases or severely damaged organ function.
Rejection criteria
Patients with poor compliance, patients without follow-up, and patients whose operation time was too long (> 45 min) were excluded from our analysis.
Sample size calculation
A priori power analysis was carried out during the planning stage of the study in order to determine the appropriate sample size that would allow performance of robust statistics on the PoSSe scale and VAS. To detect a difference between the two groups with a two-sided 5% significance level and a power of 80%, a sample size of 60 patients and 40 doctors per group was necessary.
Randomization
A randomization table was created electronically in blocks of 2 patients. The treatment assignment was performed by a person not involved in any part of the clinical treatment using sealed envelopes. Each participant had an equal chance of being assigned to one of the two groups, but they did not know this. The treatment assignment was disclosed to the surgeon immediately after tooth extraction. The PoSSe scale assessments were performed by an assessor not involved in any other part of the trial.
Surgical procedures
Surgery was performed under local anesthesia with articaine 4% and epinephrine 1:100,000 (Bieland, France). All patients were operated on by the same surgeon with more than 10 years of experience. According to the surgical difficulties and by strictly following the standard operating procedure, incision, flapping, bone removal, and tooth splitting were performed as needed. After removal of the tooth, the surgical field was meticulously rinsed with sterile 0.9% saline and sutured. After placing a cotton ball over the wound, all patients were given postoperative instructions by the surgeon (i.e., biting over the cotton ball for half an hour, intermittently applying ice on the affected cheek for 6 h after surgery, not brushing teeth on the day of the operation, and consuming only liquids for a few days). The following medication was prescribed: an antibiotic (amoxicillin 750 mg p.o. three times a day for 3 days; patients with a history of allergy to penicillin were prescribed clindamycin 300 mg p.o. four times a day for 3 days), a NSAID (ibuprofen 600 mg p.o. at least 12 h apart when necessary), and a mouthrinse (0.12% chlorhexidine mouthwash twice a day for 7 days).
Postsurgical management
Patients in the test group were asked to download the Good Doctor Online mobile app on their mobile phones and register their personal information. The surgeon used the Good Doctor Online mobile app to group and actively follow up with the patients on the first, third, and fifth days after surgery to monitor their postoperative response, reemphasize the postoperative instructions, and answer the patients’ questions. Patients in the control group did not receive a postoperative online follow-up. Patients in both groups were followed up with in the hospital for suture removal and completion of the PoSSe scale 7 days after the surgery. The PoSSe scale was used as a measure to effectively evaluate the quality of life of the patients, including their eating, talking, feeling, appearance, pain scale, nausea, and other daily life activities.
We recorded the approval of an online follow-up after tooth extraction by 20 senior doctors (≥ 40 years old) and 20 young doctors (< 40 years old). A VAS was used for the analysis, in which a score of 0 represented lack of approval and a score of 10 represented high approval. None of the 40 doctors participated in the clinical trial, and they did not know the results of the clinical trial.
This study tested the null hypothesis that there were no differences in the clinical outcomes of patients without online follow-up vs. those with online follow-up, against the alternative hypothesis of a difference. All measurements were taken by independent blinded assessors.
Statistical analysis
The SPSS 20.0 software (IBM SPSS, Inc., Chicago, IL) was used for statistical analysis in this study. Normally distributed data were presented in the form of mean ± standard deviation. The test level α was set at 0.05. Two-sided P < 0.05 was considered to indicate a statistically significant difference. Baseline data of the test and control groups were compared using the chi-square (χ2) test and independent sample t test to measure the comparability between the two groups. Kappa values were also calculated for inter- and intra-observer agreement. A κ value of < 0.40 was considered to be poor, 0.40–0.59 fair, 0.60–0.74 good, and 0.75–1.00 excellent agreement. Levene’s test was used to compare the PoSSe scale and VAS scores between the two groups.
Results
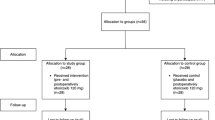
In this study, 145 patients were enrolled, and 12 patients were excluded. The remaining 133 patients were randomly divided into the test group (68 cases) and control group (65 cases). Thirteen patients did not come to the on-site follow-up, and 122 patients were finally analyzed, including 62 in the test group and 60 in the control group (Fig. 1).

CONSORT flow chart of the participants in the trial
There was no significant difference in age, operation time, sex, Pell and Gregory classification, Winter classification, relationship with inferior alveolar nerve canal, osteotomy, crown cutting, or root splitting between the two groups (P > 0.05). Thus, the two groups were comparable (Table 1). Interobserver agreement was excellent for baseline, showing a κ value of 0.93 for the classification of the third molar. Owing to this excellent interobserver agreement, the results obtained from observers were used for further analysis.
All patients successfully underwent tooth extraction. In the test group, in addition to our active follow-ups, 18 patients still actively asked questions through the app. There was 1 case of postoperative hemorrhage and 1 case of postoperative swelling that failed to improve on their own under the online guidance of the doctor and needed to be followed up with in the hospital. The remaining cases were provided nursing advice and did not need to come to the hospital, which minimized the burden of patient visits. In the control group, 9 patients returned to the hospital for follow-up treatment, including 2 cases of postoperative hemorrhage, 3 cases of discomfort due to swelling, and 4 cases of foreign body sensation in the wound. Among these 9 patients, only 1 case of postoperative hemorrhage required postoperative wound re-suturing after examination by the doctor, and the remaining cases were provided explanation and given comforting treatment. Thirty-two patients in the control group said they had questions during the whole healing process, but because they could not get the doctor’s response in time, they could only query the Internet or ask friends who had had their teeth pulled out. In the on-site follow-up 7 days after surgery, the scores of the other PoSSe scale items were significantly lower in the test group than in the control group (Table 2). Higher scores on the PoSSe scale represent more severe symptoms and worse quality of life of patients.
The VAS scores of young doctors and senior doctors for the approval of an online follow-up after tooth extraction were 8.05 ± 1.46 and 4.45 ± 2.21, respectively, indicating that the young doctors’ approval of a postoperative online follow-up was significantly higher than that of senior doctors (F = 36.78, P = 0.000).
Discussion
Extraction of impacted mandibular third molars often causes various complications and discomfort to the patients, affecting their quality of life after surgery [26]. Currently, the research on the improvement of this situation has mainly focused on the improvement of tooth extraction techniques [5, 6], suture methods [7, 8], flapping methods [9, 10], choice of implants in the extraction sockets [11, 12], irrigation of extraction sockets [13, 14], and postoperative care methods [15,16,17]. This study changed the postoperative care mode of the telephone, which was commonly used in the past, to the innovative mode of a mobile app. This method enabled us to easily register and group the patients. The patients were followed up with via the group messaging function, and we provided targeted answers to questions raised by the patients. For common questions, we set up common answers regarding the treatment of mild wound bleeding, dietary precautions, and medication timing so as to quickly reply to the patients. The mobile app can also transmit pictures, such as of patients’ mouth opening, facial swelling, and wound healing, to doctors, which is more effective than simple text communication.
With the development of Internet and the arrival of the 5G era, online medicine has developed solid technical support. In December 2019, a highly contagious pneumonia caused by a novel coronavirus was found in China [27, 28]. Hospitals are high-risk places, so the Chinese government encouraged the public to minimize going out and deal with common diseases through Internet hospitals. Thus, online medical care has a very important value.
This study found that 9 patients in the control group returned to the hospital for reexamination due to discomfort, and only 1 of them had obvious bleeding from the wound that needed to be re-sutured. The remaining 8 patients developed various postoperative reactions, leading to dental fear, which was well resolved through explanation and providing nursing advice, without the need for clinical treatment. Therefore, we believe that if the 9 patients had also received timely postoperative online consultation, some of them may not have needed to specifically return to the hospital.
The prevalence of dental fear is very high among outpatients [29, 30], especially before and after extraction [31]. Serious dental anxiety affects the doctor–patient relationship and the progress of the oral treatment plan [32]. Anxious patients are hypothesized to overestimate the amount of pain involved [33]. Fear of pain was found to be the most significant predictor of dental fear in both males and females [34]. Pain is a kind of subjective feeling. Psychological intervention can reduce the degree of pain and improve the comfort of patients through the extraction of impacted third molars [35]. Although there is a close relationship between pain and injury, the intensity of the two is not exactly the same; some pain is not necessarily caused by injury, and some injuries will not produce pain. The quality and quantity of pain perception are closely related to the cognition of pain [36]. Severe pain usually occurs in patients after extraction of impacted third molars. In order to effectively relieve the postoperative pain, it is necessary to intervene. In this study, the test group was followed up with a mobile app after operation to answer questions in time and give suggestions to relieve dental fear.
Based on the above analysis, it was not difficult to understand why the PoSSe scale scores in the test group were significantly lower than those in the control group. Through the postoperative online follow-up, we improved the quality of life of patients after extraction of impacted mandibular third molars.
Interestingly, we found that young doctors had a higher degree of approval for an online follow-up after tooth extraction using a mobile app, possibly because the young doctors grew up accompanied by the development of mobile Internet, making them more open to adopting an online follow-up than the senior doctors.
Of course, with the development of online medical care, many corresponding problems still need to be overcome, such as the coverage of medical insurance and the management of medical disputes, which require further consideration. Online medical care is still preliminary in the dental field, and there is no relevant evidence yet about the enhancing effects of these tools in the oral surgery field. There are also some limitations to our study, such as the objectivity of the evaluation method. We will make up for these defects in further studies.
Conclusions
Postoperative online follow-up effectively improves the quality of life of patients who undergo extraction of impacted mandibular third molars. Young doctors are more likely to approve the online follow-up after tooth extraction than senior doctors. However, we should seriously address many issues encountered in the development of online medical care.
References
Ibikunle AA, Adeyemo WL, Ladeinde AL (2016) Oral health-related quality of life following third molar surgery with either oral administration or submucosal injection of prednisolone. Oral Maxillofac Surg 20(4):343–352
Coulthard P, Bailey E, Esposito M, Furness S, Renton TF, Worthington HV (2014) Surgical techniques for the removal of mandibular wisdom teeth. Cochrane Database Syst Rev 7:D4345
Freudlsperger C, Deiss T, Bodem J, Engel M, Hoffmann J (2012) Influence of lower third molar anatomic position on postoperative inflammatory complications. J Oral Maxillofac Surg 70(6):1280–1285
McGrath C, Comfort MB, Lo EC, Luo Y (2003) Changes in life quality following third molar surgery--the immediate postoperative period. Br Dent J 194(5):265–268 261
Ma ZG, Xie QY, Yang C, Xu GZ, Cai XY, Li JY (2013) An orthodontic technique for minimally invasive extraction of impacted lower third molar. J Oral Maxillofac Surg 71(8):1309–1317
Ali AS, Benton JA, Yates JM (2018) Risk of inferior alveolar nerve injury with coronectomy vs surgical extraction of mandibular third molars-A comparison of two techniques and review of the literature. J Oral Rehabil 45(3):250–257
Cetinkaya BO, Sumer M, Tutkun F, Sandikci EO, Misir F (2009) Influence of different suturing techniques on periodontal health of the adjacent second molars after extraction of impacted mandibular third molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 108(2):156–161
Osunde OD, Adebola RA, Saheeb BD (2012) A comparative study of the effect of suture-less and multiple suture techniques on inflammatory complications following third molar surgery. Int J Oral Maxillofac Surg 41(10):1275–1279
Roode GJ, Butow K (2010) An alternative surgical flap design for impacted third molars: a comparison of two different surgical techniques. SADJ 65(6):246 248-251
Borgonovo AE, Giussani A, Grossi GB, Maiorana C (2014) Evaluation of postoperative discomfort after impacted mandibular third molar surgery using three different types of flap. Quintessence Int 45(4):319–330
Dos SCJ, Ritto FG, Medeiros P (2017) Efficacy of platelet-rich fibrin after mandibular third molar extraction: a systematic review and meta-analysis. J Oral Maxillofac Surg 75(8):1576–1577
Borie E, Olivi DG, Orsi IA, Garlet K, Weber B, Beltran V, Fuentes R (2015) Platelet-rich fibrin application in dentistry: a literature review. Int J Clin Exp Med 8(5):7922–7929
Ghaeminia H, Hoppenreijs TJ, Xi T, Fennis JP, Maal TJ, Berge SJ, Meijer GJ (2017) Postoperative socket irrigation with drinking tap water reduces the risk of inflammatory complications following surgical removal of third molars: a multicenter randomized trial. Clin Oral Investig 21(1):71–83
Cho H, David MC, Lynham AJ, Hsu E (2018) Effectiveness of irrigation with chlorhexidine after removal of mandibular third molars: a randomised controlled trial. Br J Oral Maxillofac Surg 56(1):54–59
Larsen MK, Kofod T, Starch-Jensen T (2019) Therapeutic efficacy of cryotherapy on facial swelling, pain, trismus and quality of life after surgical removal of mandibular third molars: a systematic review. J Oral Rehabil 46(6):563–573
Ferrante M, Petrini M, Trentini P, Perfetti G, Spoto G (2013) Effect of low-level laser therapy after extraction of impacted lower third molars. Lasers Med Sci 28(3):845–849
Zandi M, Amini P, Keshavarz A (2016) Effectiveness of cold therapy in reducing pain, trismus, and oedema after impacted mandibular third molar surgery: a randomized, self-controlled, observer-blind, split-mouth clinical trial. Int J Oral Maxillofac Surg 45(1):118–123
Sittitavornwong S, Waite PD, Holmes JD, Klapow JC (2005) The necessity of routine clinic follow-up visits after third molar removal. J Oral Maxillofac Surg 63(9):1278–1282
Inverso G, Desrochers HR, Padwa BL (2014) The value of postoperative visits for third molar removal. J Oral Maxillofac Surg 72(1):30–34
Susarla SM, Black R, Dodson TB (2011) After dentoalveolar surgery, most patients are satisfied with telephone follow-up. J Oral Maxillofac Surg 69(8):2099–2105
Tu J, Wang C, Wu S (2015) The internet hospital: an emerging innovation in China. Lancet Glob Health 3(8):e445–e446
Xie X, Zhou W, Lin L, Fan S, Lin F, Wang L, Guo T, Ma C, Zhang J, He Y, Chen Y (2017) Internet hospitals in China: cross-sectional survey. J Med Internet Res 19(7):e239
Ruta DA, Bissias E, Ogston S, Ogden GR (2000) Assessing health outcomes after extraction of third molars: the postoperative symptom severity (PoSSe) scale. Br J Oral Maxillofac Surg 38(5):480–487
Moher D, Schulz KF, Altman DG (2001) The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomised trials. Lancet 357(9263):1191–1194
Mahasantipiya PM, Savage NW, Monsour PA, Wilson RJ (2005) Narrowing of the inferior dental canal in relation to the lower third molars. Dentomaxillofac Radiol 34(3):154–163
Monaco G, De Santis G, Pulpito G, Gatto MR, Vignudelli E, Marchetti C (2015) What are the types and frequencies of complications associated with mandibular third molar coronectomy? A follow-up study. J Oral Maxillofac Surg 73(7):1246–1253
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223):497–506
Wang C, Horby PW, Hayden FG, Gao GF (2020) A novel coronavirus outbreak of global health concern. Lancet 395(10223):470–473
Tellez M, Kinner DG, Heimberg RG, Lim S, Ismail AI (2015) Prevalence and correlates of dental anxiety in patients seeking dental care. Community Dent Oral 43(2):135–142
Aartman IHA, de Jongh A, Makkes PC, Hoogstraten J (2000) Dental anxiety reduction and dental attendance after treatment in a dental fear clinic: a follow-up study. Munksgaard International Publishers, Copenhagen, pp 435–442
López-Jornet P, Camacho-Alonso F, Sanchez-Siles M (2014) Assessment of general pre and postoperative anxiety in patients undergoing tooth extraction: a prospective study. Br J Oral Maxillofac Surg 52(1):18–23
Erten H, Akarslan ZZ, Bodrumlu E (2006) Dental fear and anxiety levels of patients attending a dental clinic. Quintessence Int 37(4):304–310
Kent G (1984) Anxiety, pain and type of dental procedure. Behav Res Ther 22(5):465–469
McNeil DW, Berryman ML (1989) Components of dental fear in adults? Behav Res Ther 27(3):233–236
Gazal G, Tola AW, Fareed WM, Alnazzawi AA, Zafar MS (2016) A randomized control trial comparing the visual and verbal communication methods for reducing fear and anxiety during tooth extraction. Saudi Dent J 28(2):80–85
McNeil DW, Au AR, Zvolensky MJ, McKee DR, Klineberg IJ, Ho CCK (2001) Fear of pain in orofacial pain patients. Pain 89(2-3):245–252
Funding
This study was funded by the National Natural Science Foundation of China (81670950), the Medical Research Foundation of Guangdong Province (B2020142), and the Stomatological Hospital of Southern Medical University Research Incubation Foundation (PY2019025). We would like to thank Beijing Interactive Peak Technology Co., Ltd., for providing free use of the Good Doctor Online mobile app.
Author information
Authors and Affiliations
Contributions
Xianghuai Zheng performed the conception and design of study/review/case series and approved the manuscript and is one of the guarantors of the manuscript. Jianjiang Zhao and Zhiping Wang approved the manuscript and are one of the guarantors of the manuscript. Bo Jia performed the acquisition of data: laboratory or clinical/literature search. Zhaoqiang Zhang performed the acquisition of data: laboratory or clinical/literature search. Jinyuan Guo performed the analysis and interpretation of data collected. Zhaohui Duan performed drafting of article and/or critical revision. Xi Lin approved the manuscript and is one of the guarantors of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was registered in the Chinese Clinical Trial Registration Center (registration number: ChiCTR2000031032) and approved by the ethics committee of the Stomatological Hospital of Southern Medical University (approval number: [2019]40). All procedures performed in studies involving human participants were in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zheng, X., Zhao, J., Wang, Z. et al. Postoperative online follow-up improves the quality of life of patients who undergo extraction of impacted madibular third molars: a randomized controlled trial. Clin Oral Invest 25, 993–999 (2021). https://doi.org/10.1007/s00784-020-03388-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-020-03388-0