
Abstract
Purpose
To explore the relationship between cervical spine and the global spine alignment and to postulate the hypotheses that a lordotic alignment of cervical spine is not the only standard to identify asymptomatic subjects, and the degenerative modification of cervical curves depends primarily on their spinal-pelvic alignment.
Methods
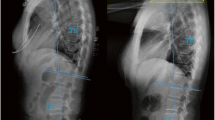
A cohort of 120 cases of Chinese asymptomatic subjects and a cohort of 121 cases of Chinese cervical spondylotic patients were recruited prospectively from 2011 to 2012. Roussouly Classification was utilized to categorize all subjects and patients according to their thoracic spine, lumbar spine and pelvic alignment. The cervical alignments were evaluated as lordosis, straight, sigmoid or kyphosis. Through the lateral X-ray images of neutral cervical and global spine, a number of parameters were measured and analyzed, including pelvic incidence, pelvic tilt, sacral slope, thoracic kyphosis (TK), lumbar lordosis, global cervical angles (angles between two lines parallel with posterior walls of C2 and C7), practical cervical angles (the addition of different cervical end plate angles from C3 to C7, and inter-vertebral angles from C23 to C67), T1 slope, spinal sacral angles (SSA), Hip to C7/Hip to Sacrum and C0–C2 angle.
Results
The percentages of cervical lordosis were 28.3 % and 36.4 % in asymptomatic and spondylotic group, respectively. The cervical spine alignments correlated with Roussouly types of global spine alignment in both asymptomatic and cervical spondylotic group (P < 0.001). And there were significant differences between Roussouly Type 2 and 4, Type 3 and 4, Type 1 and 3 in cervical angles in spondylotic group (P < 0.05). In the comparison of the two cohorts, significant differences were found in both general and practical cervical angles in Roussouly Type 4 (P = 0.00 and 0.01, respectively), and there were significant differences in inter-vertebral angle in Roussouly Type 2 at C4–5 and C5–6 levels (P = 0.04 and 0.04, respectively), and in Roussouly Type 3 at C6–7 level (P = 0.01). The SSA showed significant difference between Roussouly Type 2 and 4 in asymptomatic subjects (P = 0.00), and between Type 1 and 3, 1 and 4, 2 and 3, 2 and 4 in cervical spondylotic patients (P = 0.01, 0.02, 0.00 and 0.01, respectively). The T1 slope was significantly different among Roussouly types (P = 0.04) with its largest value in Type 1 in cervical spondylotic group. There are significant differences in C0–C2 angles in all Roussouly types (P = 0.01, 0.02, 0.00 and 0.01, respectively), as well as in the ratio of Hip to C7/hip to sacrum in Type 2 (P = 0.01), and Type 3 (P = 0.00) in the comparison of the two cohorts. The multiple linear regression of all parameters showed both general and practical cervical angles were significantly related to TK, C0–C2 and T1 slope (P = 0.01, 0.00 and 0.00, respectively).
Conclusion
The cervical alignment correlates with their global spine and pelvic curves. And lordosis is not the only presentation in asymptomatic subjects. The degenerative modification of cervical disc angles was the compensation of global spine degeneration for horizontal gaze. Cervical angles are influenced by their TK angles, occipital-C2 joint and the tilt of T1 vertebral body. The occipital-C2 joint has a compensating mechanism in all Roussouly types in cervical spondylosis.





Similar content being viewed by others


Notes
Consent was obtained from each subject or patient with the approval from Peking University Third Hospital Institutional Review Board.
References
Gore DR, Sepic SB, Gardner GM (1986) Roentgenographic findings of the cervical spine in asymptomatic people. Spine 11:521–524
Kasai T, Ikata T, Katoh S et al (1996) Growth of the cervical spine with special reference to its lordosis and mobility. Spine 21(18):2067–2073
Harrison DD, Troyanovich SJ, Harrison DE et al (1996) A normal sagittal spinal configuration: a desirable clinical outcome. J Manipulative Physiol Ther 19:398–405
Lee CS, Noh H, Lee DH et al (2012) Analysis of sagittal spinal alignment in 181 asymptomatic children. J Spinal Disord Tech 25(8):E259–E263
Hardacker JW, Shuford RF, Capicotto PN et al (1997) Radiographic standing cervical segmental alignment in adult volunteers without neck symptoms. Spine 22:1472–1480
Boyle J, Milne N, Singer K (2002) Influence of age on cervicothoracic spinal curvature: an ex vivo radiographic surgery. Clin Biomech 17:361–371
Mac-Thiong JM, Labelle H, Charlebois M (2003) Sagittal plane analysis of the spine and pelvis in adolescent idiopathic scoliosis according to the coronal curve type. Spine 28(13):1404–1409
Roussouly P, Gollogly S, Berthonnaud E et al (2005) Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine 30(3):346–353
Legaye J, Duval-Beaupere G, Hecquet J et al (1998) Pelvic incidence: a fundamental parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J 7(2):99–103
Roussouly P, Gollogly S, Noseda O et al (2006) The vertical projection of the sum of the ground reactive forces of a standing patient is not the same as the C7 plumb line. A radiographic study of the sagittal alignment of 153 asymptomatic volunteers. Spine 31(11):E320–E325
Barrey C, Jund J, Noseda O et al (2007) Sagittal balance of the pelvis-spine complex and lumbar degenerative disease. A comparative study about 85 cases. Eur Spine J 16(9):1459–1467
Matsunaga S, Onishi T, Sakou T (2001) Significance of occipitoaxial angle in subaxial lesion after occipitocervical fusion. Spine 26(2):161–165
Knott PT, Mardjetko SM, Techy F (2010) The use of the T1 sagittal angle in predicting overall sagittal balance of the spine. Spine J 10:994–998
Ohara A, Miyamoto K, Naganwa T et al (2006) Reliabilities of and correlations among five standard methods of assessing the sagittal alignment of the cervical spine. Spine 31(22):2585–2591
Park MS, Moon SH, Lee HM et al (2013) The effect of age on cervical sagittal alignment normative data on 100 asymptomatic subjects. Spine 38(8):E458–E463
Mac-Thiong J.M., Roussouly P, Berthonnaud E et al (2010) Sagittal parameters of global spinal balance normative values from a prospective cohort of seven hundred nine Caucasian asymptomatic adult. Spine 35(22):E1193–1198
Gore DR (2001) Roentgenographic findings in the cervical spine in asymptomatic persons: a ten-year follow-up. Spine 26(22):2463–2466
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yu, M., Zhao, WK., Li, M. et al. Analysis of cervical and global spine alignment under Roussouly sagittal classification in Chinese cervical spondylotic patients and asymptomatic subjects. Eur Spine J 24, 1265–1273 (2015). https://doi.org/10.1007/s00586-015-3832-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-015-3832-2