
Abstract
Background
This study aimed to assess predictors for grade 3–5 vesicoureteral reflux (VUR) in infants ≤ 2 months of age admitted for first urinary tract infection (UTI).
Methods
Retrospective cohort study of 195 infants ≤ 2 months admitted to a pediatric ward for first UTI between 2006 and 2017. Clinical, laboratory, and imaging data were collected from electronic medical charts. We examined associations between grade 3–5 VUR and different patient characteristics.
Results
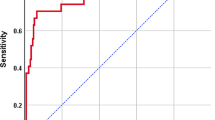
Twenty infants (10%) were diagnosed with grade 3–5 VUR; all had fever. Infants with grade 3–5 VUR had higher blood neutrophil percentage (BNP) (65% vs. 46%, P < 0.001), higher neutrophil-to-lymphocyte ratio (NLR) (2.6 vs. 1.3, P < 0.001), more renal ultrasound abnormalities (prenatal 26% vs. 5%, P = 0.007; postnatal 84% vs. 55%, P = 0.015), and Pseudomonas UTI (15% vs. 1%, respectively, P < 0.001). NLR > 1.65 showed sensitivity 100% and specificity 61% for detecting grade 3–5 VUR. BNP > 53% showed sensitivity 100% and specificity 60% for detecting grade 3–5 VUR. BNP was the best single marker for grade 3–5 VUR with area under the curve (AUC) of 0.82 (95% CI 0.75–0.89). In a multivariate model, AUC for combination of BNP and hydronephrosis was 0.86 (95% CI 0.79–0.93, P = 0.007).
Conclusions
Infants ≤ 2 months of age admitted for a first UTI are at risk for grade 3–5 VUR and thus should undergo a voiding cystourethrography (VCUG) if their renal ultrasound is abnormal or if they have Pseudomonas UTI. Avoiding VCUG can be considered in afebrile infants and in infants with BNP < 53% or NLR < 1.65.



Similar content being viewed by others


References
Morley EJ, Lapoint JM, Roy LW, Cantor R, Grant WD, Paolo WF, Wojcik S (2012) Rates of positive blood, urine, and cerebrospinal fluid cultures in children younger than 60 days during the vaccination era. Pediatr Emerg Care 28:125–130. https://doi.org/10.1097/PEC.0b013e318243fa50
Swerkersson S, Jodal U, Sixt R, Stokland E, Hansson S (2017) Urinary tract infection in small children: the evolution of renal damage over time. Pediatr Nephrol 32:1907–1913. https://doi.org/10.1007/s00467-017-3705-5
Ylinen E, Ala-Houhala M, Wikström S (2003) Risk of renal scarring in vesicoureteral reflux detected either antenatally or during the neonatal period. Urology 61:1238–1242. https://doi.org/10.1016/S0090-4295(03)00229-2
Tekgül S, Riedmiller H, Hoebeke P, Kočvara R, Nijman RJ, Radmayr C, Stein R, Dogan HS, European Association of Urology (2012) EAU guidelines on vesicoureteral reflux in children. Eur Urol 62:534–542. https://doi.org/10.1016/j.eururo.2012.05.059
RIVUR Trial Investigators, Hoberman A, Greenfield SP, Mattoo TK, Keren R, Mathews R, Pohl HG, Kropp BP, Skoog SJ, Nelson CP, Moxey-Mims M, Chesney RW, Carpenter MA (2014) Antimicrobial prophylaxis for children with vesicoureteral reflux. N Engl J Med 370:2367–2376. https://doi.org/10.1056/NEJMoa1401811
Subcommittee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management, Roberts KB (2011) Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics 43:595–610. https://doi.org/10.1083/jcb.43.3.564
Mori R, Lakhanpaul M, Verrier-Jones K (2007) Diagnosis and management of urinary tract infection in children: summary of NICE guidance. BMJ 335:395–397. https://doi.org/10.1136/bmj.39286.700891.AD
Lebowitz RL, Olbing H, Parkkulainen KV, Smellie JM, Tamminen-Möbius TE (1985) International system of radiographic grading of vesicoureteric reflux. International Reflux Study in Children. Pediatr Radiol 15:105–109
Weiss R, Duckett J, Spitzer A (1992) Results of a randomized clinical trial of medical versus surgical management of infants and children with grades III and IV primary vesicoureteral reflux (United States). The International Reflux Study in Children. J Urol 148:1667–1673
Cleper R, Krause I, Eisenstein B, Davidovits M (2004) Prevalence of vesicoureteral reflux in neonatal urinary tract infection. Clin Pediatr (Phila) 43:619–625. https://doi.org/10.1177/000992280404300706
Ismaili K, Lolin K, Damry N, Alexander M, Lepage P, Hall M (2011) Febrile urinary tract infections in 0- to 3-month-old infants: a prospective follow-up study. J Pediatr 158:69–72. https://doi.org/10.1016/j.jpeds.2010.06.053
Kanellopoulos TA, Salakos C, Spiliopoulou I, Ellina A, Nikolakopoulou NM, Papanastasiou DA (2006) First urinary tract infection in neonates, infants and young children: a comparative study. Pediatr Nephrol 21:1131–1137. https://doi.org/10.1007/s00467-006-0158-7
Wallace SS, Zhang W, Mahmood NF, Williams JL, Cruz AT, Macias CG, Quinonez RA, Orth RC (2015) Renal ultrasound for infants younger than 2 months with a febrile urinary tract infection. AJR Am J Roentgenol 205:894–898. https://doi.org/10.2214/AJR.15.14424
Fernbach SK, Maizels M, Conway JJ (1993) Ultrasound grading of hydronephrosis: introduction to the system used by the Society for Fetal Urology. Pediatr Radiol 23:478–480
Lee MD, Lin CC, Huang FY, Tsai TC, Huang CT, Tsai JD (2009) Screening young children with a first febrile urinary tract infection for high-grade vesicoureteral reflux with renal ultrasound scanning and technetium-99m-labeled dimercaptosuccinic acid scanning. J Pediatr 154:797–802. https://doi.org/10.1016/j.jpeds.2008.12.045
Dayan PS, Hanson E, Bennett JE, Langsam D, Miller SZ (2004) Clinical course of urinary tract infections in infants younger than 60 days of age. Pediatr Emerg Care 20:85–88. https://doi.org/10.1097/01.pec.0000113876.10140.9b
Littlewood JM (1972) 66 infants with urinary tract infection in first month of life. Arch Dis Child 47:218–226. https://doi.org/10.1136/adc.47.252.218
Chang PW, Abidari JM, Shen MW, Greenhow TL, Bendel-Stenzel M, Roman HK, Biondi EA, Schroeder AR, PRIS Bacteremic UTI Investigators (2016) Urinary imaging findings in young infants with bacteremic urinary tract infection. Hosp Pediatr 6:647–652. https://doi.org/10.1542/hpeds.2015-0229
Leroy S, Romanello C, Smolkin V, Galetto-Lacour A, Korczowski B, Tuerlinckx D, Rodrigo C, Gajdos V, Moulin F, Pecile P, Halevy R, Gervaix A, Duhl B, Vander Borght T, Prat C, Foix-L'Hélias L, Altman DG, Gendrel D, Bréart G, Chalumeau M (2012) Prediction of moderate and high grade vesicoureteral reflux after a first febrile urinary tract infection in children: construction and internal validation of a clinical decision rule. J Urol 187:265–271. https://doi.org/10.1016/j.juro.2011.09.034
Halimi-Asl A, Hosseini AH, Nabavizadeh P (2014) Can procalcitonin reduce unnecessary voiding cystoureterography in children with first febrile urinary tract infection? Iran J Pediatr 24:418–422
Han SY, Lee IR, Park SJ, Kim JH, Shin JI (2016) Usefulness of neutrophil-lymphocyte ratio in young children with febrile urinary tract infection. Korean J Pediatr 59:139–144. https://doi.org/10.3345/kjp.2016.59.3.139
Oostenbrink R, van der Heijden AJ, Moons KGM, Moll HA (2000) Prediction of vesico-ureteric reflux in childhood urinary tract infection: a multivariate approach. Acta Paediatr Int J Paediatr 89:806–810. https://doi.org/10.1111/j.1651-2227.2000.tb00380.x
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the institutional Research Ethics Board, waiving the need for informed consent.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bahat, H., Ben-Ari, M., Ziv-Baran, T. et al. Predictors of grade 3–5 vesicoureteral reflux in infants ≤ 2 months of age with pyelonephritis. Pediatr Nephrol 34, 907–915 (2019). https://doi.org/10.1007/s00467-018-4167-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-018-4167-0