
Abstract
Objective
The purpose of this study was to investigate the effects of diagnostic and surgical developments in the complete resection of the mediastinal masses.
Methods
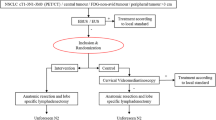
Of 313 patients, 236 underwent therapeutic or diagnostic complete resections. We analyzed age, gender, diagnostic interventions, neoadjuvant treatment, type of surgical intervention (sternotomy, video-assisted thoracic surgery [VATS], thoracotomy), pathology, duration of hospital stay, complications, mortality, and associated diseases. Patients were divided into two groups according to the period of operation: group A included patients who were operated on between January 2002 and January 2007; group B included patients who were operated on between January 2007 and January 2012.
Results
Resection with VATS increased significantly after 2007, from 17.7 to 35 % (p = 0.03). The rate of complications increased after 2007 (p = 0.03), which was apparent in non-VATS patients (p = 0.03). The use of magnetic resonance imaging (MRI) decreased from 29 to 15.5 % (p = 0.02) and positron emission tomography (PET)–computed tomography (CT) use increased from 1.6 to 25.2 % (p < 0.001).
Conclusions
We identified a paradigm shift in mediastinal mass surgery. PET–CT became a more preferred diagnostic method and MRI became less preferred. The rate of VATS resection doubled and sternotomy decreased. Complication rates increased in non-VATS due to an increase in extended resections.
Similar content being viewed by others


References
Davis RD, Oldham HN, Sabiston DC (1987) Primary cysts and neoplasms of the mediastinum: recent changes in the clinical presentation, methods of diagnosis, management, and results. Ann Thorac Surg 44:229–237
Yim AP, Kay RL, Ho JK (1995) Video-assisted thoracoscopic thymectomy for myasthenia gravis. Chest 108:1440–1443
Landrenau RJ, Dowling RD, Castillo WM, Ferson PF (1992) Thoracoscopic resection of anterior mediastinal tumor. Ann Thorac Surg 54:142–144
Palanivelu C, Prakash A, Senthilkumar R (2006) Minimally invasive esophagectomy: thoracoscopic mobilization of the esophagus and mediastinal lymphadenectomy in prone position-experience of 130 patients. J Am Coll Surg 203(1):7–16
Marulli G, Rea F, Melfi F et al (2012) Robot-aided thoracoscopic thymectomy for early-stage thymoma: a multicenter European study. J Thorac Cardiovasc Surg 144:1125–1132
Heimburger IL, Battersby JS, Velios F (1963) Primary mediastinal tumors of the childhood. J Thorac Cardiovasc Surg 86:978–984
Rubush JL, Gardner IR, Boyd WC, Ehrenhaft JL (1973) Mediastinal tumors: review of 186 cases. J Thorac Cardiovasc Surg 65:216–222
Ovrum E, Birkeland S (1979) Mediastinal tumors and cysts: a review of 91 cases. Scand J Thorac Cardiovasc Surg 13:161–168
Nandi P, Wong KC, Mok CK (1980) Primary mediastinal tumors. J R Coll Surg Edinb 25:460–466
Grosfeld JL, Skinner MA, Rescorla FJ et al (1994) Mediastinal tumors in children: experience with 196 cases. Ann Surg Oncol 1:121–127
Toker A, Erus S, Ozkan B, Ziyade S, Tanju S (2011) Does a relationship exist between the number of thoracoscopic thymectomies performed and the learning curve for thoracoscopic resection of thymoma in patients with myasthenia gravis? Interact Cardiovasc Thorac Surg 12(2):152–155
Yim APC (1995) Video-assisted thoracoscopic management of anterior mediastinal masses. Surg Endosc 9:1184–1188
Cheng YJ, Wu HH, Chou SH, Kao EL (2001) Video-assisted thoracoscopic management of mediastinal tumours. JSLS 5:241–244
Chetty GK, Khan OA, Onyeaka CVP, Ahmad F, Rajesh PB, Waller DA (2004) Experience with videoassisted surgery for suspected mediastinal tumors. Eur J Surg Oncol 30(7):776–780
El-Bawab H, Al-Sugair AA, Rafay M, Hajjar W, Mahdy M, Al-Kattan K (2007) Role of flourine-18 fluorodeoxyglucose positron emission tomography in thymic pathology. Eur J Cardiothorac Surg 31(4):731–736
Otsuka H (2012) The utility of FDG-PET in the diagnosis of thymic epithelial tumors. J Med Invest 59(3–4):225–234
Hida Y, Muto J, Kaga K et al (2012) Indication of video-assisted thoracic surgery for mediastinal mass lesions. Kyobu Geka 65(11):934–938
Brown LR, Aughenbaugh GL (1991) Masses of the anterior mediastinum: CT and MR imaging. AJR 157:1171–1180
Patel PM, Alibazoglu H, Ali A, Fordham E, La Monica G (1996) Normal thymic uptake of FDG on PET imaging. Clin Nucl Med 21(10):772–775
Brink I, Reinhardt MJ, Hoegerle S, Altehoefer C, Moser E, Nitzche EU (2001) Increased metabolic activity in the thymus gland studied with 18 FDG PET: age dependency and frequency after chemotherapy. J Nucl Med 42(4):591–595
Disclosure
Alper Toker, Suat Erus, Erkan Kaba, Serhan Tanju, and Berker Özkan have no conflicts of interest relevant to the content of this paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Toker, A., Erus, S., Kaba, E. et al. Has there been a paradigm shift in mediastinal surgery from open to minimally invasive, and from magnetic resonance imaging (MRI) to positron emission tomography–computerized tomography (PET–CT) in the last decade?. Surg Endosc 28, 861–865 (2014). https://doi.org/10.1007/s00464-013-3233-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-3233-8