
Abstract
Purpose
Endoscopic sphenopalatine artery ligation (ESPAL) is known as an effective treatment for posterior epistaxis. Anatomical variations of the intranasal branching may result in long operative time and possible inadequate cauterization. A modification of ESPAL by cauterization at the sphenopalatine foramen (SPF), has been performed by our group. Our study assessed the clinical benefit of endoscopic sphenopalatine foramen cauterization (ESFC) and compared it to ESPAL.
Method
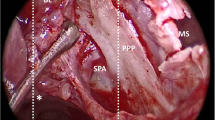
A retrospective study was conducted. Patients who received ESFC for posterior epistaxis from 2016 to 2018 at a tertiary hospital were recruited. Middle meatal antrostomy was done. After ethmoidal crest was identified and nipped, pterygopalatine fossa was entered through the SPF. Sphenopalatine artery (SPA) and its branches within the SPF were cauterized without identification of any SPA distal branches in the nasal cavity. Patients receiving conventional ESPAL by the same surgeon were recruited and compared as control. Patients were followed-up for 3 months. Success rate, operative time, and complication were assessed.
Results
Thirty-four patients were identified. Recurrent epistaxis was absent in 90.0% and 100% of patients receiving ESPAL (9/10 patients) and ESFC (24/24 patients) respectively, p = 0.294. Median operative time was 115 and 60 min, respectively, p < 0.001. Ipsilateral hard palatal or anterior palatal numbness were found in one and three patients, respectively. All resolved spontaneously within 2 weeks.
Conclusion
ESFC is effective in treating posterior epistaxis. It requires significantly less amount of time while the success rate was comparable to conventional ESPAL.

Similar content being viewed by others


References
Abdelkader M, Leong SC, White PS (2007) Endoscopic control of the sphenopalatine artery for epistaxis: long-term results. J Laryngol Otol 121:759–762
Sharp HR, Rowe-Jones JM, Biring GS, Mackay IS (1997) Endoscopic ligation or diathermy of the sphenopalatine artery in persistent epistaxis. J Laryngol Otol 111:1047–1050
O’Flynn PE, Shadaba A (2000) Management of posterior epistaxis by endoscopic clipping of the sphenopalatine artery. Clin Otolaryngol Allied Sci 25:374–377
Snyderman CH, Goldman SA, Carrau RL, Ferguson BJ, Grandis JR (1999) Endoscopic sphenopalatine artery ligation is an effective method of treatment for posterior epistaxis. Am J Rhinol 13:137–140
Kumar S, Shetty A, Rockey J, Nilssen E (2003) Contemporary surgical treatment of epistaxis. What is the evidence for sphenopalatine artery ligation? Clin Otolaryngol Allied Sci 28:360–363
Traboulsi H, Alam E, Hadi U (2015) Changing trends in the management of epistaxis. Int J Otolaryngol 2015:263987
Simmen DB, Raghavan U, Briner HR, Manestar M, Groscurth P, Jones NS (2006) The anatomy of the sphenopalatine artery for the endoscopic sinus surgeon. Am J Rhinol 20:502–505
Budrovich R, Saetti E (1992) Microscopic and endoscopic ligature of the sphenopalatine artery. Laryngoscope 102:1390–1394
Prades JM, Asanau A, Timoshenko AP, Faye MB, Martin C (2008) Surgical anatomy of the sphenopalatine foramen and its arterial content. Surg Radiol Anat 30:583–587
Bolger WE, Borgie RC, Melder P (1999) The role of the crista ethmoidalis in endoscopic sphenopalatine artery ligation. Am J Rhinol 13:81–86
Midilli R, Orhan M, Saylam CY, Akyildiz S, Gode S, Karci B (2009) Anatomic variations of sphenopalatine artery and minimally invasive surgical cauterization procedure. Am J Rhinol Allergy 23:e38–41
Harvinder S, Rosalind S, Gurdeep S (2008) Endoscopic cauterization of the sphenopalatine artery in persistent epistaxis. Med J Malaysia 63:377–378
Saraceni Neto P, Nunes LMA, Caparroz FAd, Gregorio LL, de Souza RPESF, Simões JC, Kosugi EM (2017) Resection of the ethmoidal crest in sphenopalatine artery surgery. Int Forum Allergy Rhinol 7:87–90
Chandra RK, Rohman GT, Walsh WE (2008) Anterior palate sensory impairment after septal surgery. Am J Rhinol 22:86–88
Langford RJ (1989) The contribution of the nasopalatine nerve to sensation of the hard palate. Br J Oral Maxillofac Surg 27:379–386
Midilli R, Gode S, Ozturk K (2015) The “two-point” technique for endoscopic sphenopalatine artery cauterization: is it effective and safe? Hippokratia 19:284
Piastro K, Scagnelli R, Gildener-Leapman N, Pinheiro-Neto CD (2018) Outcomes of sphenopalatine and internal maxillary artery ligation inside the pterygopalatine fossa for posterior epistaxis. Rhinology 56:144–148
Acknowledgements
We would like to thank Naret Taengyai, Head of Otolaryngology Division, Sawan Pracharak Hospital, for his technical advice and continued support.
Funding
Unfunded project. Wirach Chitsuthipakorn, Kachorn Seresirikachorn, and Dichapong Kanjanawasee have no financial disclosure. Kornkiat Snidvongs is a speaker at the Bureau for Merck Sharp Dolme, Menarini, and Meda.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by WC, KS, and KS. The first draft of the manuscript was written by WC and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors, hereby, declare no conflict of interest.
Ethical approval
Sawanpracharak Hospital Ethics Committee, Approval No. 5/2561, 6th February, 2018.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
VDO 1_ESPAL. The video of the conventional technique of Endoscopic Sphenopalatine Artery ligation (ESPAL). (MP4 70024 kb)
VDO 2_ESFC. The video of the Endoscopic Sphenopalatine Foramen Cauterization (ESFC). (MP4 75653 kb)
Rights and permissions
About this article

Cite this article
Chitsuthipakorn, W., Seresirikachorn, K., Kanjanawasee, D. et al. Endoscopic sphenopalatine foramen cauterization is an effective treatment modification of endoscopic sphenopalatine artery ligation for intractable posterior epistaxis. Eur Arch Otorhinolaryngol 277, 2463–2467 (2020). https://doi.org/10.1007/s00405-020-06005-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-020-06005-8