
Abstract
Purpose
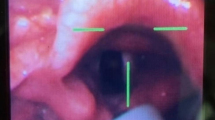
Present study compares two routes in nasal passage for transnasal flexible fiberoptic laryngoscopy (TNFFL).
Methods
Included in the study were 60 patients who were split equally into Group 1 and Group 2 and all underwent TNFFL. The tip of endoscope was introduced between the septum and inferior turbinate along the nasal floor in Group 1 and between the inferior turbinate and middle turbinate in Group 2. O2 saturation, heart rate, systolic blood pressure, diastolic blood pressure of patients were taken 30 min before and immediately after procedure. Patients were asked to rate the pain-irritation, gag reflex, dyspnea they experienced during procedure using visual analogue scale. Two routes were compared in terms of physiological effects and patient comfort.
Results
No statistically significant difference was found between two groups in terms of physiological effects or patient comfort. When values recorded immediately after procedure were compared with baseline values, a significant decrease was observed in O2 saturation and heart rate in Group 1 and Group 2, respectively. No clinically detectable symptoms were observed in the patients.
Conclusion
Decreases in O2 saturation and heart rate may be regarded as physiological effects of TNFFL. No significant difference between two routes was noted in the present study in terms of physiological effects and patient comfort during TNFFL. Introducing the endoscope between the inferior and middle turbinates may be a comfortable and safe option, particularly if the endoscope cannot be advanced along the nasal floor due to septum deviation, septal crest, inferior turbinate hypertrophy.
Similar content being viewed by others


References
Sawashima M, Hirose H (1968) New laryngoscopic technique by use of fiber optics. J Acoust Soc Am 43(1):168–169
Guo Y, Feng Y, Liang H, Zhang R, Cai X, Pan X (2018) Role of flexible fiberoptic laryngoscopy in predicting difficult intubation. Minerva Anestesiol 84(3):337–345
Lehoczki CLB, Carvalho D, Ng RTY, Gusmão RJ (2006) Nasolaryngoscopy or laryngotracheoscopy: which is the best exam for assessing the airways of children? Braz J Otorhinolaryngol 72(4):487–490
Ongkasuwan J, Yung KC, Courey MS (2012) The physiologic impact of transnasal flexible endoscopy. The Laryngoscope 122(6):1331–1334
Silberman HD, Wilf H, Tucker JA (1976) Flexible fiberoptic nasopharyngolaryngoscope. Ann Otol Rhinol Laryngol 85(5):640–645
Javed F, Parmar A, Hussain A, Hajioff D, Pinder D (2017) A randomised controlled trial assessing the efficacy of co-phenylcaine nasal spray in flexible transnasal pharyngolaryngoscopy. Ann R Coll Surg Engl 99(4):313–318
Hwang SH, Park CS, Kim BG, Cho JH, Kang JM (2015) Topical anesthetic preparations for rigid and flexible endoscopy: a meta-analysis. Eur Arch Otorhinolaryngol 272(2):263–270
Saif AM, Farboud A, Delfosse E, Pope L, Adke M (2016) Assessing the safety and efficacy of drugs used in preparing the nose for diagnostic and therapeutic procedures: a systematic review. Clin Otolaryngol 41(5):546–563
Conlin AE, McLean L (2008) Systematic review and meta-analysis assessing the effectiveness of local anesthetic, vasoconstrictive, and lubricating agents in flexible fibre-optic nasolaryngoscopy. J Otolaryngol Head Neck Surg 37(2):240–249
-Sunkaraneni VS, Jones SE (2011) Topical anaesthetic or vasoconstrictor preparations for flexible fibre-optic nasal pharyngoscopy and laryngoscopy. Cochrane Database Syst Rev 3
Sadek SAA, De R, Scott A, White AP, Wilson PS, Carlin WV (2001) The efficacy of topical anaesthesia in flexible nasendoscopy: a double-blind randomised controlled trial. Clin Otolaryngol Allied Sci 26(1):25–28
Mahrous AK, Tysome JR, Davis JP (2012) A prospective randomised controlled trial in one hundred and eleven patients to determine whether flexible nasendoscopic laryngoscopy is more comfortable for patients when performed above or below the inferior turbinate. Clin Otolaryngol 37(3):238
Pownell PH, Minoli JJ, Rohrich RJ (1997) Diagnostic nasal endoscopy. Plast Reconstr Surg 99(5):1451–1458
Smith DH, Brook CD, Virani S, Platt MP (2018) The inferior turbinate: an autonomic organ. Am J Otolaryngol 39(6):771–775
Clerico DM (2014) An experimental study of pain upon stimulation of the nasal and sinus cavities. Am J Otolaryngol 35(3):300–304
Abu-Bakra M, Jones NS (2001) Does stimulation of nasal mucosa cause referred pain to the face? Clin Otolaryngol Allied Sci 26(5):430–432
Ovassapian A, Yelich SJ, Dykes MH, Brunner EE (1983) Blood pressure and heart rate changes during awake fiberoptic nasotracheal intubation. Anesth Analg 62(10):951–954
Yung KC, Courey MS (2010) The effect of office-based flexible endoscopic surgery on hemodynamic stability. The Laryngoscope 120(11):2231–2236
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (Yozgat Bozok University Clinical Researches Ethic Committee Ref No.: 2017-KAEK-189ˍ2019.09.25ˍ06) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Cengiz, C., Şahin, E., Dağıstan, H. et al. Comparison of two routes in nasal passage for transnasale flexible fiberoptic laryngoscopy. Eur Arch Otorhinolaryngol 277, 785–789 (2020). https://doi.org/10.1007/s00405-019-05753-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-019-05753-6