
Abstract
Drug-induced sedation endoscopy (DISE) classification systems play a significant role in clinical analysis based on DISE findings, treatment decision process, treatment planning process and fundamentally in treatment outcomes. However, there is a major problem: there is no universally agreed DISE classification system. Hence, for the same DISE examination different DISE classification systems can be used to: assess anatomic findings, decide and plan different treatments. Hence, this leads to different treatment outcomes. The key objective of this study is to propose uDISE model: universal drug-induced sedation endoscopy (DISE) classification system. Set theory and relational mapping was used to develop a DISE classification system based on anatomical structures/level; degree of severity; and configuration of obstruction and its relationship with existing DISE classification systems. uDISE model consists of seven anatomical sites (nose, velum, tonsils, lateral pharyngeal wall/oropharynx, tongue base, epiglottis and larynx), three degrees of obstructive severity (none, partial and complete), three configurations of obstruction (anteroposterior, lateral and circumferential) and a severity index. uDISE model was mapped to four existing DISE classification systems: Pringle and Croft grading system, VOTE, NOHL and P-T-L-Tb-E. uDISE model provides a methodology for mapping different DISE findings based on different classification systems into one common DISE assessments format. This provides a framework for comparing different DISE assessments, treatment plan and treatment outcome irrespective of DISE classification system used. Further research is required to establish a complete relational mapping between uDISE model and other existing DISE classification systems.
Similar content being viewed by others

Introduction
When surgery is the considered treatment intervention for obstructive sleep apnea, identification, analysis and reporting of upper airway obstruction during sleep is important for optimal surgical intervention outcomes [1]. Croft and Pringle proposed drug-induced sleep endoscopy (DISE) as an endoscopic evaluation of the dynamic changes of the upper airway during sedated sleep [2].
DISE has been shown to:
-
1.
Provide 3D dynamic visualisation of multi-segmental upper airway obstruction [3].
-
2.
Provide quality assessment of dynamic airway events [4];
-
3.
Provide useful information on patient management [5].
-
4.
Improve treatment planning as compared to using awake upper airway assessments technique [6].
-
5.
Have reliable intraobserver agreement [7].
-
6.
Have moderate to substantial interrater reliability [8].
-
7.
Have good test–rest reliability [9].
-
8.
Have good agreement with polysomnography [10].
Some criticisms of DISE includes:
-
1.
Changes in snoring patterns in sedated sleep as compared to natural sleep [11].
-
2.
Merely a snapshot of snoring; not representative of how snoring changes throughout the sleep [12].
-
3.
Subjective evaluation assessment [13].
-
4.
A growing number for multiple classification systems [14].
However, DISE is growing to become the gold standard for observing dynamic upper airway obstruction during sleep.
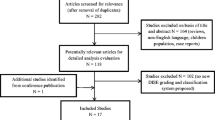
This study focuses on the problem of multiple DISE classification systems. At the first European Position Meeting on DISE, the problem was stated “It is disappointing that so far no consensus has been reached on a scoring and classification system… The goal remains to come to one universally accepted classification system” [14]. Furthermore, seven different DISE classification systems were highlighted in the European position paper on DISE [14] (for more details on different DISE classification system, readers should read Table 3 in [14] and references [2, 7, 15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30]). Furthermore, it has been suggested that there are potentially over 16 DISE classification system proposed in the literature [31].
The objectives of this study are to:
-
1.
Develop a universal DISE classification system, uDISE model.
-
2.
Provide a framework for relating uDISE model with other existing DISE classification systems.
DISE classification system
Methods
uDISE model
uDISE model classification system was developed by analysing 18 existing DISE classification systems based on anatomical structures, anatomical levels, severity of obstruction and configuration of obstruction [2, 7, 15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30].
Classification referential mapping
uDISE model was mapped to four existing DISE classification systems using set theory and relational mapping based on anatomical structures, anatomical levels, severity of obstruction and configuration of obstruction.
Discussion
uDISE model
The uDISE model (Table 1) encompasses the most commonly involved structures, encompassing the degree and configuration of obstruction.
Severity of obstruction
The severity of obstruction for assessing the degree of airway narrowing is [32]:
-
1.
0: no obstruction (no vibration, <50%).
-
2.
1: partial obstruction (vibration 50–75%).
-
3.
2: complete obstruction (collapse, >75%).
Configuration of obstruction
The configuration of obstruction can be described as anteroposterior (anterior structures moving posteriorly against the posterior pharyngeal wall), lateral (structures move laterally towards the centre of the airway) or concentric (combination of the former) [14].
Anatomical structures
The seven most common obstruction sites are evaluated in uDISE model: nose, velum, tonsil, oropharynx (lateral walls), tongue base, epiglottis and larynx.
Nasal obstruction was considered to be obstruction in the nasal cavity and nasopharynx [22]. Obstruction at the velum was related to obstruction to the soft palate, uvula or lateral pharyngeal wall tissue at the level of the velopharynx [21]. Due to the indistinguishability of the three structures both anatomically and during DISE examination, they were grouped as velum obstruction [21]. Velum obstruction was considered to occur in the anteroposterior, lateral and concentric configuration. Obstruction at the oropharynx walls was solely based on obstruction involving only lateral pharyngeal wall tissue [21]. Tonsils obstruction was considered as a distinct structure separate from the lateral pharyngeal wall tissue [14, 21, 29]. Both tonsils and lateral pharyngeal wall tissue all collapsed in a lateral configuration [21]. Tongue base obstruction was the narrowing of the airway at the tongue based in the anteroposterior, lateral and circumferential configuration based on the space between the anterior commissure and the posterior pharyngeal wall [7, 21, 29]. Epiglottis obstruction occurred when the epiglottis collapse was either as a result of the anteroposterior prolapse of the folding of the epiglottis with decreased structural rigidity or posterior displacement of the entire epiglottis towards the pharyngeal wall with normal structural integrity or a lateral folding of the epiglottis. Laryngeal obstructions were considered to be obstruction at the supraglottic and glottis [22].
Obstruction scoring
An example of a completely normal result would be N0V0Ts0O0Tb0E0L0. A tonsillar enlargement causing obstruction will be scored as N0V0Ts1LO0Tb0E0L0. A simple palate snoring will be scored as N0V1APTs0O0Tb0E0L0. A multilevel obstruction with severe tonsillar obstruction and severe tongue based obstruction will score N0V0Ts2LO0Tb2APE0L0.
Treatment planning
Ongoing research is examining how uDISE model score relates with surgical treatment [1]. Example of uDISE model score—treatment relationship will be
-
N0V1APTs0O0Tb0E0L0—uvulopalatopharyngoplasty.
-
N0V0Ts2LO0Tb2APE0L0—tonsillectomy and tongue base reduction.
Severity index
The severity index is calculated by adding the digits representing the severity of obstruction at each anatomic structure/level [23]. For a patent airway with a score of N0V0Ts0O0Tb0E0L0 is 0. A single-level epiglottic obstruction N0V0Ts0O0Tb0E2APL0 is 2. A multilevel obstruction at the tonsil and tongue base, N0V0Ts2LO0Tb2APE0L0, has a severity index of 4.
Relational mapping
Pringle et al. [15]
Grade 1 (G1P), simple palatal snoring consisted of the following properties: no obstruction (velum, AP, C, L, 0), noise production, vibration of soft palate (velum, AP, 1), vibration of the walls of the velopharyngeal sphincter (velum, AP, 1) and upper oropharynx (velum, L, 1), flapping of soft palate during inspiration (velum, AP, 1), prolapse of the uvula into the nasopharynx during expiration (velum, AP, 1), narrowing of the velopharyngeal area in the anteroposterior (velum, AP, 1) and circumferential direction (velum, C, 1) and tonsils bulging into the narrowing of the airway (tonsils, L, 0, 1). Grade 1 obstruction was mapped to uDISE model as:
-
G1P → {V0–1, AP, L, C} U {Ts0–1, L}.
Grade 2 (G2P), single-level palatal obstruction consisted of the following properties: obstructive episodes (velum, 2), mild-to-severe obstruction (velum, 2), obstruction only at velopharyngeal level (velum), anteroposterior (velum, AP), lateral (velum, AP), circumferential obstruction (velum, C). Grade 1 obstruction was mapped to uDISE model as:
-
G2P → {V2, AP, L, C} U {Ts2, L,}.
Grade 3 (G3+P), multi-segmental involvement—intermittent oro-hypopharyngeal collapse consisted of the following properties: obstruction at the velopharyngeal level and oro-hypopharyngeal level during inspiration (velum, oropharynx, AP, L, C 2). Due to the constraint of a required obstruction at the oropharynx, velum was excluded. Grade 3 (G3+P) was mapped to oropharynx obstruction with anteroposterior, lateral and concentric configuration as shown below:
-
G3+P → {O2, AP, L, C}.
Grade 4 (G4+P), sustained multi-segmental obstruction consisted of the following properties: obstruction at the velopharyngeal level and oro-hypopharyngeal level during inspiration and expiration (velum, oropharynx, AP, L, C 2). Due to the oro-hypopharyngeal constraint, velum was excluded. A+ sign was used to indicate multisegment obstruction. Grade 4 obstruction (G4+P) was mapped to oropharynx obstruction with anteroposterior, lateral and concentric configuration as shown below:
-
G4+P → {O2, AP, L, C}.
Grade 5 (G5P), tongue base-level obstruction consisted of the following properties: obstruction occurs at the level of tongue base with either the tongue base appearing to fall back onto the posterior pharyngeal wall (tongue base, 0–2, AP) or the posterior pharyngeal walls appearing to close down onto the tongue base (tongue base, 0–2, AP); epiglottis obscures the laryngeal inlet and obstructs the airway (epiglottis, 0–2, AP). Grade 5 (G5p) obstruction was mapped to tongue base and epiglottis obstruction in uDISE model as shown below:
-
G5p → {T0–2, AP, L, C: E0–2, AP, L}.
Pringle and Croft grading system accounts for inspiration and expiration for grade 3 and grade 4 which is not accounted for in uDISE model as it is not widely regarded as an important factor. Also, it is not clear how the Pringle and Croft grading system classifies single-level obstruction at the oropharynx level, nose and larynx.
Kezirian et al. [21]
VOTE classification system consists of four levels (velum, oropharynx, tongue base and epiglottis); three degrees of obstruction (0—none, 1—partial, and 2—complete), and three configurations of obstruction (anteroposterior, lateral, and concentric).
Obstruction at the velum level (Vk) with three degrees of obstruction (0–2) and three obstruction configurations [anteroposterior (AP), lateral (L) and concentric (C)] in VOTE classification was directly mapped to obstruction at the velum level (V) with three degrees of obstruction (0–2) and three obstruction configurations [anteroposterior (AP), lateral (L) and concentric (C)] in uDISE model:
-
Vk 0–2, AP, L, C → {V0–2, AP, L, C}.
Obstruction at the oropharynx level (Ok) with three degrees of obstruction (0–2) and one obstruction configuration (L) in the VOTE classification system was mapped directly to the oropharynx (O) and tonsils with three degrees of obstruction (0–2) and one obstruction configuration (L) in the uDISE model:
-
Ok 0–2, L → {O0–2, L} U {Ts0–2, L}.
Obstruction at the tongue base level (Tk) with three degrees of obstruction (0–2) and obstruction configuration in AP direction in the VOTE classification system was mapped directly to tongue base level (Tb) with three degrees of obstruction (0–2) and obstruction configuration in AP direction in uDISE model:
-
Tk 0–2, AP → {T0–2, AP}.
Obstruction at the epiglottis level (Ek) with three degrees of obstruction (0–2) and two obstruction configurations in anteroposterior and lateral direction in the VOTE classification system was mapped directly with obstruction at the epiglottis level (E) with three degrees of obstruction (0–2) and two obstruction configurations in anteroposterior and lateral direction in uDISE model:
-
Ek 0–2, AP, L → {E0–2, AP, L}.
VOTE classification does not consider obstruction at the nose and larynx [22]. In addition, VOTE does not account for concentric obstruction at the oropharynx level [33] and lateral and concentric obstruction at the tongue base [7].
Vicini et al. [22]
NOHL classification system consists of four levels [nose (Nv), oropharynx (Ov), hypopharynx (Hv), and larynx (Lv)]; three degrees of obstruction (0–25%: 1, 25–50%: 2, 50–75%: 3, 75–100%: 4) and three configurations of obstruction [anteroposterior, transversal (t), and concentric].
Obstruction at the nose was mapped as:
-
NV 1–4 → {N0–2}.
Due to the static nature of obstruction at the nasal level, the configuration of the obstruction is not important. Furthermore, the effect of nasal obstruction on OSA is still debatable.
Obstruction in the transverse direction of the oropharynx was mapped as:
-
OV t, 1–2 → {O0, L}; OV t, 3 → {O1, L}; OV t, 4 → {O2, L}.
Obstruction in the concentric direction of the oropharynx was mapped as:
-
OV C, 1–2 → {O0, C}; OV c, 3 → {O1, C}; OV c, 4 → {O2, C}.
Palatine tonsillar hypertrophy grade (grade 3 or 4) was mapped as:
-
TsV 3, 4 → {Ts 2, L}.
Obstruction in the AP direction of the tongue base was mapped as:
-
HV AP, 1–2 → {T0, AP}; HV AP, 3 → {T1, AP}; HV AP, 4 → {T2, AP}.
Obstruction in the lateral direction of the tongue base was mapped as:
-
HV L, 1–2 → {T0, l}; HV L, 3 → {T1, L}; HV L, 4 → {T2, L}.
Obstruction in the concentric direction of the tongue base was mapped as:
-
HV C, 1–2 → {T0, l}; HV C, 3 → {T1, L}; HV C, 4 → {T2, L}.
Obstruction in the AP direction of the epiglottis was mapped as:
-
LN → {E0, AP}; LP → {E1–2, AP}.
Obstruction in the lateral direction of the epiglottis was mapped as:
-
LN → {E0, L}; LP → {E1–2, L}.
Anteroposterior, lateral and concentric obstruction at the velum in uDISE model was mapped as follows:
-
V0, AP → {OV AP, 1–2}; V1, AP → {OV AP, 3}; V2, AP → {OV AP, 4},
-
V0, L → {OV t, 1–2}; V1, L → {OV t, 3}; V2, L → {OV t, 4},
-
V0, C → {OV C, 1–2}; V1, C → {OV C, 3}; V2, L → {OV C, 4}.
Veer [29]
P-T-L-Tb-E classification system evaluated obstruction at five key anatomical sites: palate (PV), tonsils (TV), lateral wall (LV), tongue base (TbV) and epiglottis (EV), three degrees of obstruction (0—none, <50%—partial, and >50%—complete) and three configurations of obstruction (anteroposterior, lateral, and concentric).
Obstruction at the palate level (PV) with anteroposterior and concentric obstruction was mapped to the obstruction at the velum (V) with anteroposterior and concentric obstruction:
-
PV 1 → {V0, AP, C}; PV 2 → {V1–2, AP}; PV 3 → {V1–2, C}.
Obstruction at the tonsils was mapped as obstruction at the tonsil level with lateral obstruction configuration:
-
TV 1 → {Ts0, L}; TV 2 → {Ts1, L}; TV 3 → {Ts2, L}.
Obstruction at the lateral pharyngeal wall was mapped to obstruction at the oropharynx with lateral obstruction configuration:
-
LV 1 → {O0, L}; LV 2 → {O1, L}; LV 3 → {O2, L}.
Obstruction at the tongue base was mapped to obstruction at the tongue base with anteroposterior obstruction configuration:
-
TbV 1 → {T0, AP}; TbV 2 → {T1, AP}; TbV 3 → {T2, AP}.
Obstruction at the epiglottis was mapped to obstruction at the epiglottis with anteroposterior obstruction configuration:
-
EV 1 → {E0, AP}; EV 2 → {E1–2, AP}.
It is worth mentioning that obstruction at the nose and larynx are not considered in P-T-L-Tb-E classification system. Furthermore, obstruction in the lateral direction at the velum level, obstruction at the oropharynx in the anteroposterior and concentric direction, obstruction at the tongue base in the lateral and concentric direction and obstruction at the epiglottis in the lateral direction is not considered in P-T-L-Tb-E classification system.
Limitations
This study has its three key limitations. First, uDISE model is a model based on an amalgamation of the strength of existing DISE classification system which inherently limits the scope of adding new anatomical structures and configurations of obstructions. Second, uDISE model was related to four existing DISE classification systems. More research is needed to relate uDISE model with other existing DISE classification systems. Third, a randomised clinical study is required to validate the accuracy and reliability of uDISE model.
Conclusion
First, uDISE model is a new DISE classification system for analysing visual findings based on DISE in an easy, accurate, objective and systematic way. Second, uDISE model provides a framework for mapping different DISE findings across different classification systems into one common DISE assessment format. Hence, this provides a methodology for comparing different DISE assessment, treatment plan and treatment outcome irrespective of initial DISE classification system used. Third, uDISE model provides a frame work to relate assessment score with treatment plan and potentially predicts treatment outcome. Fourth, uDISE model provides both a human and computational framework for systematically classifying DISE findings. Further research is needed to clinically validate uDISE model.
References
De Vito A, Agnoletti V, Zani G, Corso RM, D’Agostino G, Firinu E, Marchi C, Hsu Y-S, Maitan S, Vicini C (2017) The importance of drug-induced sedation endoscopy (D.I.S.E.) techniques in surgical decision making: conventional versus target controlled infusion techniques—a prospective randomized controlled study and a retrospective surgical outcomes analysis. Eur Arch Otorhinolaryngol 274(5):2307–2317
Croft CB, Pringle M (1991) Sleep nasendoscopy: a technique of assessment in snoring and obstructive sleep apnoea. Clin Otolaryngol Allied Sci 16(5):504–509
Berry S, Roblin G, Williams A, Watkins A, Whittet HB (2005) Validity of sleep nasendoscopy in the investigation of sleep related breathing disorders. Laryngoscope 115(3):538–540
Kotecha BT, Hannan SA, Khalil HMB, Georgalas C, Bailey P (2007) Sleep nasendoscopy: a 10-year retrospective audit study. Eur Arch Otorhinolaryngol 264(11):1361–1367
Georgalas C, Garas G, Hadjihannas E, Oostra A (2010) Assessment of obstruction level and selection of patients for obstructive sleep apnoea surgery: an evidence-based approach. J Laryngol Otol 124(1):1–9
Eichler C, Sommer JU, Stuck BA, Hörmann K, Maurer JT (2013) Does drug-induced sleep endoscopy change the treatment concept of patients with snoring and obstructive sleep apnea? Sleep Breath 17(1):63–68
Carrasco-Llatas M, Zerpa-Zerpa V, Dalmau-Galofre J (2017) Reliability of drug-induced sedation endoscopy: interobserver agreement. Sleep Breath 21(1):173–179
Kezirian EJ, White DP, Malhotra A, Ma W, McCulloch CE, Goldberg AN (2010) Interrater reliability of drug-induced sleep endoscopy. Arch Otolaryngol Head Neck Surg 136(4):393–397
Rodriguez-Bruno K, Goldberg AN, McCulloch CE, Kezirian EJ (2009) Test–retest reliability of drug-induced sleep endoscopy. Otolaryngol Head Neck Surg 140(5):646–651
Llatas MC, Porras GA, Gonzalez MTC, Sanbartolome AR, Bayarri PG, Gomez-Pajares F, Galofre JD (2014) Drug-induced sleep endoscopy: a two drug comparison and simultaneous polysomnography. Eur Arch Otorhinolaryngol 271(1):181–187
Marais J (1998) The value of sedation nasendoscopy: a comparison between snoring and non-snoring patients. Clin Otolaryngol Allied Sci 23(1):74–76
Hill PD, Osman EZ, Osborne JE, Lee BWV (2000) Changes in snoring during natural sleep identified by acoustic crest factor analysis at different times of night. Clin Otolaryngol Allied Sci 25(6):507–510
Vroegop AV, Vanderveken OM, Wouters K, Hamans E, Hohenhorst W, Kezirian EJ, Kotecha B, De Vries N, Braem MJ, Van De Heyning PH (2012) Variation in observer agreement in drug-induced sleep endoscopy. Sleep 35:A143
De Vito A, Carrasco Llatas M, Vanni A, Bosi M, Braghiroli A, Campanini A, de Vries N, Hamans E, Hohenhorst W, Kotecha BT, Maurer J, Montevecchi F, Piccin O, Sorrenti G, Vanderveken OM, Vicini C (2014) European position paper on drug-induced sedation endoscopy (DISE). Sleep Breath 18(3):453–465
Pringle MB, Croft CB (1993) A grading system for patients with obstructive sleep apnoea-based on sleep nasendoscopy. Clin Otolaryngol Allied Sci 18(6):480–484
Camilleri AE, Ramamurthy L, Jones PH (1995) Sleep nasendoscopy: what benefit to the management of snorers? J Laryngol Otol 109(12):1163–1165
Quinn SJ, Daly N, Ellis PDM (1995) Observation of the mechanism of snoring using sleep nasendoscopy. Clin Otolaryngol 20(4):360–364
Sadaoka T, Kakitsuba N, Fujiwara Y, Kanai R, Takahashi H (1996) The value of sleep nasendoscopy in the evaluation of patients with suspected sleep-related breathing disorders. Clin Otolaryngol Allied Sci 21(6):485–489
Higami S, Inoue Y, Higami Y, Takeuchi H, Ikoma H (2002) Endoscopic classification of pharyngeal stenosis pattern in obstructive sleep apnea hypopnea syndrome. Psychiatry Clin Neurosci 56(3):317–318
Iwanaga K, Hasegawa K, Shibata N, Kawakatsu K, Akita YY, Suzuki K, Yagisawa M, Nishimura T (2003) Endoscopic examination of obstructive sleep apnea syndrome patients during drug-induced sleep. Acta Otolaryngol Suppl 550(550):36–40
Kezirian EJ, Hohenhorst W, De Vries N (2011) Drug-induced sleep endoscopy: the VOTE classification. Eur Arch Otorhinolaryngol 268(8):1233–1236
Vicini C, De Vito A, Benazzo M, Frassineti S, Campanini A, Frasconi P, Mira E (2012) The nose oropharynx hypopharynx and larynx (NOHL) classification: a new system of diagnostic standardized examination for OSAHS patients. Eur Arch Otorhinolaryngol 269(4):1297–1300
Bachar G, Nageris B, Feinmesser R, Hadar T, Yaniv E, Shpitzer T, Eidelman L (2012) Novel grading system for quantifying upper-airway obstruction on sleep endoscopy. Lung 190(3):313–318
Victores AJ, Takashima M (2012) Effects of nasal surgery on the upper airway: a drug-induced sleep endoscopy study. Laryngoscope 122(11):2606–2610
Gillespie MB, Reddy RP, White DR, Discolo CM, Overdyk FJ, Nguyen SA (2013) A trial of drug-induced sleep endoscopy in the surgical management of sleep-disordered breathing. Laryngoscope 123:277–282. doi:10.1002/lary.23506
Koo SK, Choi JW, Myung NS, Lee HJ, Kim YJ, Kim YJ (2013) Analysis of obstruction site in obstructive sleep apnea syndrome patients by drug induced sleep endoscopy. Am J Otolaryngol Head Neck Med Surg 34(6):626–630
Lee CH, Kim DK, Kim SY, Rhee C-S, Won T-B (2015) Changes in site of obstruction in obstructive sleep apnea patients according to sleep position: a DISE study. Laryngoscope 125(1):248–254
Herzog M, Kellner P, Plößl S, Glien A, Rohrmeier C, Kühnel T, Plontke S, Herzog B (2015) Drug-induced sleep endoscopy and simulated snoring in patients with sleep-disordered breathing: agreement of anatomic changes in the upper airway. Eur Arch Otorhinolaryngol 272(9):2541–2550
Veer V (2016) Comprehensive documentation for sleep surgery. In: European sleep surgery conference
Soares D, Folbe AJ, Yoo G, Badr MS, Rowley JA, Lin H-S (2013) Drug-induced sleep endoscopy vs awake Müller’s maneuver in the diagnosis of severe upper airway obstruction. Otolaryngol Neck Surg 148(1):151–156
De Vito A (2017) Response to letter to the editor: “is drug induced sedation endoscopy surgical decision making process objective and systematic?” Eur Arch Otorhinolaryngol. doi:10.1007/s00405-017-4564-1
Hohenhorst W, Ravesloot MJL, Kezirian EJ, De Vries N (2012) Drug-induced sleep endoscopy in adults with sleep-disordered breathing: technique and the VOTE classification system. Oper Tech Otolaryngol Neck Surg 23(1):11–18
Ravesloot MJL, de Vries N (2011) One hundred consecutive patients undergoing drug-induced sleep endoscopy: results and evaluation. Laryngoscope 121(12):2710–2716
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding was received for this research.
Conflict of interest
Esuabom Dijemeni declares that he has no conflict of interest. Gabriele D’Amone declares that he has no conflict of interest. Israel Gbati declares that he has no conflict of interest.
Ethical approval
This article does not contain any studies with human and animals participants performed by any of the authors.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Dijemeni, E., D’Amone, G. & Gbati, I. uDISE model: a universal drug-induced sedation endoscopy classification system—part 1. Eur Arch Otorhinolaryngol 274, 3795–3801 (2017). https://doi.org/10.1007/s00405-017-4597-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-017-4597-5