
Abstract
Nonanaplastic follicular cell-derived thyroid carcinoma (NAFCTC) includes differentiated- (DTC) and poorly differentiated thyroid carcinoma (PDTC). DTC has an excellent prognosis, while PDTC is situated between DTC and anaplastic carcinomas. Short-term studies suggest that PDTC patients diagnosed only on tumor necrosis and/or mitosis have a prognosis similar to those diagnosed according to the TURIN proposal. The purpose of this study was to evaluate prognosis for NAFCTC based on long-term follow-up illuminating the significance of tumor necrosis and mitosis. A cohort of 225 patients with NAFCTC was followed more than 20 years. Age, sex, distant metastasis, histology, tumor size, extrathyroidal invasion, lymph node metastasis, tumor necrosis and mitosis were examined as possible prognostic factors. Median follow-up time for patients alive was 28 years (range 20–43 years). Age, distant metastasis, extrathyroidal invasion, tumor size, tumor necrosis and mitosis were independent prognostic factors in multivariate analysis for overall survival (OS). In disease specific survival (DSS) age was not significant. Using only necrosis and/or mitosis as criteria for PDTC the 5-, 10- and 20-year OS for DTC was 87, 79 and 69%, respectively. In DSS it was 95, 92 and 90%. For PDTC the 5-, 10- and 20-year OS was 57, 40 and 25%, respectively. In DSS it was 71, 55 and 48%. Tumor necrosis and mitosis are highly significant prognostic indicators in analysis of long time survival of nonanaplastic follicular cell-derived thyroid carcinoma indicating that a simplification of the actually used criteria for poorly differentiated carcinomas may be justified.
Similar content being viewed by others


Introduction
Thyroid carcinoma is a relatively uncommon cancer accounting for approximately 1% of malignant disease; still it is the most frequent endocrine malignancy [1, 2]. Over the last decades a rise in incidence has been detected in several countries including Denmark and it seems that especially the incidentally found papillary micro-carcinomas are responsible for the increase [3, 4].
Nonanaplastic follicular cell-derived thyroid carcinoma (NAFCTC) includes differentiated- (DTC) and poorly differentiated thyroid carcinoma (PDTC). DTC has an excellent prognosis with a 10-year survival above 90% [5], while PDTC is situated between DTC and anaplastic carcinomas. In 2004, WHO recognized PDTC as a separate histological entity and defined it as “a follicular-cell neoplasm that shows limited evidence of structural follicular cell differentiation and occupy both morphologically and behaviorally an intermediate position between differentiated (follicular and papillary carcinomas) and undifferentiated (anaplastic) carcinoma” [6]. In 2006, Hiltzik et al. found that PDTC defined on the basis of only mitosis and necrosis constitutes a group of tumors that is more aggressive and homogeneous than PDTC defined by the WHO criteria [7]. In 2007, the TURIN proposal was published including necrosis and mitosis, as proposed by Hiltzik et al. but also, it was extended with variables concerning growth pattern (solid, trabecular or insular) and nuclear morphology [8] making interpretation more complicated. Controversy still exists regarding the diagnostic criteria [7, 9, 10]. In 2014, Gnemmi et al. published a comparison of the TURIN proposal with Hiltzik’s histological grade not including growth pattern. They found similar performances in predicting prognosis [11], indicating that the less complicated model from Hiltzik et al. could be a sufficient tool for identification of PDTC. However, the median follow-up time for the Hiltzik and the Gnemmi studies were only 3.5 and 5.7 years, respectively.
The purpose of this study was to evaluate prognosis for NAFCTC based on long-term follow-up with focus on the significance of tumor necrosis and mitosis.
Materials and methods
From 1970 to 1992, 297 patients with histologically verified primary thyroid carcinoma were treated and/or followed at Odense University Hospital, Denmark—a tertiary head and neck cancer center. Due to the unique Danish personal identity number it was possible to establish a retrospective cohort study of NAFCTC patients with a long-term follow-up. All patients came from a well-defined geographic area, the Region of Southern Denmark. At the end of the inclusion period the same pathologist (PA) did a complete histological revision. Autopsy findings were not included.
Two hundred thirty-one patients had histologically verified NAFCTC. In six cases treatment with curative intent was not possible and they were excluded from further analysis. Two hundred twenty-five patients were eligible for analysis. Three patients were lost to follow-up because of emigration. They were censored according to last available information.
Follow-up procedure for thyroid cancer was performed with a 3-month interval 2 years after treatment and a 6-month interval the following 3 years. In the case of recurrence follow-up procedure would start over. Standard ENT examination was performed. Ultrasound was not yet standard procedure and was not done routinely.
Initial data concerning diagnostic procedures, treatment, and histology has been shown in an earlier publication [12], while new data concerning recurrence, last contact to hospital and cause of death were retrieved as part of the present study. The information was obtained from review of patient charts, contact to general practitioners and death certificates. In survival analysis primary endpoints were death and recurrence. Survival analysis was investigated as overall survival (OS) and disease specific survival (DSS). In OS death from all causes was considered an event. In DSS death from disease or death with disease were considered events. Recurrence was defined as persistent disease or occurrence of disease after the end of primary treatment confirmed by histology, cytology and/or imaging. Patients with a residual tumor after primary treatment were registered with the date of recurrence set to be the date of diagnosis. In a few cases only the month of recurrence was available, thus the date of recurrence was listed as the first of that month. Closing date for the follow-up was March 1, 2013.
TNM staging was performed according to the fourth edition of UICC TNM classification [13]. An update to the seventh edition [14] was not possible due to insufficient information concerning lymph node metastasis and extrathyroidal invasion. Indications for radioactive iodine treatment (RAI) were presence of distant metastasis, lymph node metastasis, extrathyroidal extension and/or non-radical surgery.
Age at the time of diagnosis, sex, distant metastasis, histological type (papillary versus follicular), tumor size, extrathyroidal invasion (pT4), regional lymph node metastasis, tumor necrosis and mitosis and were evaluated as possible prognostic factors. All variables were dichotomized. Age had 45 years as cut-point. For tumor size the median was used as cut-point. Distant metastasis, extrathyroidal invasion, tumor necrosis and regional lymph node metastasis were registered as “present” or “not present”. The presence of mitosis was registered as positive if more than one mitosis per high power field was observed.
Survival curves were generated using the Kaplan–Meier method. In univariate analysis the Mantel-Haenzel log-rank test was used to evaluate differences between groups. P values < 0.05 were considered significant. Variables identified as significant for survival in univariate analysis were included in a multivariate Weibull regression model, model fit was checked using Cox-Schnell residuals. Backward selection procedures were performed.
Medlog® (Information Analysis Corporation, Crystal Bay, Nevada 89402 USA) for Windows® version 2012-8 was used for clinical data management and data registration, and SPSS® for MAC version 21 (IBM Corporation, Armonk, New York 10504-1722 USA) and STATA/IC 11 (StataCorp LP, College Station, Texas 77845 USA) were used for statistical analysis.
Results
Follow-up
Two hundred twenty-five patients were included in the analysis and the female:male ratio was 2.8:1. The median age at the time of diagnosis was 51 years (range 8–91 years).
The median follow-up time for patients alive was 28 years (range 20–43 years), when the three patients lost to follow-up were not included. They were censored after 3, 4 and 19 years, respectively. One hundred seventeen patients died during the period of follow-up (0.2–34 years after diagnosis). The median age at the time of death was 75 years (range 31–99 years). During follow-up, 117 patients died (thyroid carcinoma 45%; other disease than cancer 37%; other cancer 13%; accidents 2%; complications to treatment 1%; unknown 3%). Sixty-seven patients had recurrence. Stage and treatment of the study group are shown in Table 1.
Prognostic factors
Univariate analysis of patient and tumor related prognostic factors are shown in Table 2. In six patients no primary tumor was found leaving 219 patients for analysis of histological features.
A total of 218 patients had sufficient tissue for examination of all parameters and were included in a multivariate analysis using death as primary endpoint. The results are shown in Table 3.
Surgical treatment was dichotomized with total and subtotal thyroidectomies in one group and less extensive procedures in another group. In univariate analysis surgical treatment was not significant. Patients who received RAI had a significantly worse prognosis compared to non-receivers, but this difference disappeared when adjustment for stage was performed.
Survival
Figures 1 and 2 show Kaplan–Meier survival curves for NAFCTC. In OS the 5-, 10- and 20-year survival was 75, 65 and 54%, respectively. In DSS 53 the 5-, 10- and 20-year survival was 84, 78 and 75%, respectively.

Kaplan–Meier curve for overall survival in 225 patients displayed with 95% confidence interval

Kaplan–Meier curve for disease specific survival in 225 patients displayed with 95% confidence interval
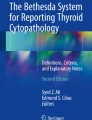
Figure 3 shows Kaplan–Meier survival curves for DTC and Hiltzik criteria group for OS. In the DTC group the 5-, 10- and 20-year survival was 87, 79 and 69%, respectively. In the Hiltzik criteria group the 5-, 10- and 20-year survival was 57, 40 and 25%, respectively. Log rank test showed significantly difference between the groups (P < 0.0001).

Kaplan–Meier curve for overall survival in differentiated thyroid carcinoma and Hiltzik criteria group
Figure 4 shows Kaplan–Meier survival curves for DTC and Hiltzik criteria group for DSS. In the DTC group the 5-, 10- and 20-year survival was 95, 92 and 90%, respectively. In the Hiltzik criteria group the 5-, 10- and 20-year survival was 71, 55 and 48%, respectively. Log rank test showed significantly difference between the groups (P < 0.0001).

Kaplan–Meier curve for disease specific survival in differentiated thyroid carcinoma and Hiltzik criteria group
Discussion
This study is the first to evaluate the prognostic significance of the Hiltzik criteria (tumor necrosis and mitosis) on NAFCTC long time survival. In general DTC displays an excellent prognosis and since recurrence and death from disease can occur after decades, a long follow-up time is important. In the present study, all patients were followed for at least 20 years. This provides an accurate 20-year survival analysis with no censoring due to a short follow-up time, which strengthens the study. Limitations are the treatment at a single institution, a relatively small number of patients and variation in treatment strategy since at the time no national or regional treatment guidelines were available for standardization.
An initial analysis of the study group was performed in 1998 [12]. It was based on a relatively short follow-up time with a median of 10.2 years. Age above 45 years, distant metastasis, tumor necrosis, extrathyroidal invasion and p53-expression were found to be significant prognostic indicators. At that time PDTC was not yet recognized as a separate histological entity, and consequently some of the specimens would be re-classified as PDTC today explaining the relatively poor survival results initially presented.
The aim of the present study was to evaluate long-term prognostic factors with focus on tumor necrosis and mitosis. This would allow differentiation in survival analysis between DTC and PDTC according to the Hiltzik criteria [7], which Gnemmi el al. [11] found to be similar to TURIN criteria in predicting prognosis. Our study based on very long observation time confirms the results by Gnemmi et al.
Age is generally known to be one of the most influential prognostic factors in DTC, but there is still disagreement on where to set the cut-point. In numerous studies different cut-points are suggested such as 40, 45, 50 and 60 years [5, 15–20]. In our study 45 years was the cut-point, which is in accordance to the UICC/TNM staging system for DTC [14]. In the multivariate analysis of our series age is significant in OS but not in DSS.
Distant metastasis is also a very strong prognostic factor in DTC. This has been shown in several others studies [16, 18, 21] and is yet reconfirmed. Because of standardization of radioiodine therapy prognosis may have slightly improved for patients with distant metastasis, especially in younger patients with lung metastases and 131I-uptake [22].
Godballe et al. [12] identified both tumor size and extrathyroidal invasion as significant prognostic factors in univariate analysis, but the significance of size disappeared in the multivariate analysis. In the present long-term study tumor size remained significant in multivariate analysis of NAFCTC, suggesting that both tumor size and extrathyroidal invasion contain prognostic information.
In univariate analysis histological type (papillary versus follicular) was significant in OS and DSS. Patients with follicular carcinoma had a considerable less favorable prognosis than patients with papillary carcinoma. However, this significance was not found in multivariate analysis. The result is confirmed in some studies [5, 16, 17], while other studies find a prognostic difference [19–21].
Tumor necrosis and tumor mitosis were significant independent prognostic factors in OS and DSS in multivariate analysis. As mentioned above these factors are used in histology grading for PDTC, which is a relatively new diagnostic entity [9]. According to the TURIN proposal information regarding convoluted nuclei and growth pattern (trabecular/insular/solid) is also required to classify PDTC. In our study information about growth pattern was not evaluated. Thus application of the TURIN proposal was not possible. However, the Hiltzik criteria only required the high-grade features tumor necrosis and/or mitosis. When the NAFCTC patients were divided according to the Hiltzik criteria (Fig. 2), 153 patients were classified as DTC and 66 patients as PDTC. Compared to several other studies this model displayed similar 10-year survival exceeding 90% [5, 19, 23] for DTC. In PDTC 5-year OS has been reported from 60 to 73% [7, 11, 24], which is comparable to the 5-year OS at 57% in this study. Our findings support that tumor necrosis and/or mitosis according to Hiltzik criteria identify a group of patients with an intermediate prognosis equivalent to PDTC.
Due to the long follow-up time this study showed some interesting recurrences. Four patients in our study had their first recurrence more than 10 years after initial treatment. In one case the patient had the first recurrence 27 years after initial treatment and died 5 years later from thyroid carcinoma with distant metastases in multiple organs. This has also been observed in other long-term follow-up studies [25]. The findings emphasize the importance of a long follow-up time.
Conclusion
Tumor necrosis and mitosis are highly significant prognostic indicators in analysis of long time survival of nonanaplastic follicular cell-derived thyroid carcinoma indicating that a simplification of the actually used criteria for poorly differentiated carcinomas may be justified.
References
Blomberg M, Feldt-Rasmussen U, Andersen KK, Kjaer SK (2012) Thyroid cancer in Denmark 1943–2008, before and after iodine supplementation. Int J Cancer 131(10):2360–2366. doi:10.1002/ijc.27497
Sherman SI (2003) Thyroid carcinoma. The Lancet 361(9356):501–511
Londero SC, Krogdahl A, Bastholt L, Overgaard J, Pedersen HB, Frisch T, Bentzen J, Pedersen PU, Christiansen P, Godballe C (2013) Papillary thyroid carcinoma in Denmark 1996–2008: an investigation of changes in incidence. Cancer Epidemiol 37(1):e1–e6. doi:10.1016/j.canep.2012.10.011
Londero SC, Krogdahl A, Bastholt L, Overgaard J, Trolle W, Pedersen HB, Bentzen J, Schytte S, Christiansen P, Godballe C, Danish Thyroid Cancer G (2013) Papillary thyroid microcarcinoma in Denmark 1996–2008: a national study of epidemiology and clinical significance. Thyroid 23(9):1159–1164. doi:10.1089/thy.2012.0595
Mazzaferri EL, Jhiang SM (1994) Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med 97(5):418–428
DeLellis RA et al (2004) Pathology and genetics of tumours of endocrine organs. International Agency for Research in Cancer, Lyon
Hiltzik D, Carlson DL, Tuttle RM, Chuai S, Ishill N, Shaha A, Shah JP, Singh B, Ghossein RA (2006) Poorly differentiated thyroid carcinomas defined on the basis of mitosis and necrosis: a clinicopathologic study of 58 patients. Cancer 106(6):1286–1295. doi:10.1002/cncr.21739
Volante M, Collini P, Nikiforov YE, Sakamoto A, Kakudo K, Katoh R, Lloyd RV, LiVolsi VA, Papotti M, Sobrinho-Simoes M, Bussolati G, Rosai J (2007) Poorly differentiated thyroid carcinoma: the Turin proposal for the use of uniform diagnostic criteria and an algorithmic diagnostic approach. Am J Surg Pathol 31(8):1256–1264. doi:10.1097/PAS.0b013e3180309e6a
Volante M, Papotti M (2010) Poorly differentiated thyroid carcinoma: 5 years after the 2004 WHO classification of endocrine tumours. Endocr Pathol 21(1):1–6. doi:10.1007/s12022-009-9100-4
Tallini G (2011) Poorly differentiated thyroid carcinoma. Are we there yet? Endocr Pathol 22(4):190–194. doi:10.1007/s12022-011-9176-5
Gnemmi V, Renaud F, Do Cao C, Salleron J, Lion G, Wemeau JL, Copin MC, Carnaille B, Leteurtre E, Pattou F, Aubert S (2014) Poorly differentiated thyroid carcinomas: application of the Turin proposal provides prognostic results similar to those from the assessment of high-grade features. Histopathology 64(2):263–273. doi:10.1111/his.12246
Godballe C, Asschenfeldt P, Jorgensen KE, Bastholt L, Clausen PP, Hansen TP, Hansen O, Bentzen SM (1998) Prognostic factors in papillary and follicular thyroid carcinomas: p53 expression is a significant indicator of prognosis. Laryngoscope 108(2):243–249
Hermanek P, Sobin LH (1987) TNM classification of malignant tumours, vol 4., fully rev. ed. Springer, Berlin
Sobin LH, Gospodarowicz MK, Wittekind C (2010) TNM classification of malignant tumours, vol 7. ed. Wiley-Blackwell, Chichester
Bellantone R, Lombardi CP, Boscherini M, Ferrante A, Raffaelli M, Rubino F, Bossola M, Crucitti F (1998) Prognostic factors in differentiated thyroid carcinoma: a multivariate analysis of 234 consecutive patients. J Surg Oncol 68(4):237–241
Eustatia-Rutten CF, Corssmit EP, Biermasz NR, Pereira AM, Romijn JA, Smit JW (2006) Survival and death causes in differentiated thyroid carcinoma. J Clin Endocrinol Metab 91(1):313–319. doi:10.1210/jc.2005-1322
Konturek A, Barczynski M, Nowak W, Richter P (2012) Prognostic factors in differentiated thyroid cancer—a 20-year surgical outcome study. Langenbeck’s. Arch Surg 397(5):809–815. doi:10.1007/s00423-011-0899-z
Pelizzo MR, Boschin IM, Toniato A, Piotto A, Pagetta C, Gross MD, Al-Nahhas A, Rubello D (2007) Papillary thyroid carcinoma: 35-year outcome and prognostic factors in 1858 patients. Clin Nucl Med 32(6):440–444. doi:10.1097/RLU.0b013e31805375ca
Sciuto R, Romano L, Rea S, Marandino F, Sperduti I, Maini CL (2009) Natural history and clinical outcome of differentiated thyroid carcinoma: a retrospective analysis of 1503 patients treated at a single institution. Ann Oncol 20(10):1728–1735. doi:10.1093/annonc/mdp050
Vorburger SA, Ubersax L, Schmid SW, Balli M, Candinas D, Seiler CA (2009) Long-term follow-up after complete resection of well-differentiated cancer confined to the thyroid gland. Ann Surg Oncol 16(10):2862–2874. doi:10.1245/s10434-009-0592-4
Lundgren CI, Hall P, Dickman PW, Zedenius J (2006) Clinically significant prognostic factors for differentiated thyroid carcinoma: a population-based, nested case-control study. Cancer 106(3):524–531. doi:10.1002/cncr.21653
Durante C, Haddy N, Baudin E, Leboulleux S, Hartl D, Travagli JP, Caillou B, Ricard M, Lumbroso JD, De Vathaire F, Schlumberger M (2006) Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. J Clin Endocrinol Metab 91(8):2892–2899. doi:10.1210/jc.2005-2838
Gilliland FD, Hunt WC, Morris DM, Key CR (1997) Prognostic factors for thyroid carcinoma. A population-based study of 15,698 cases from the surveillance, epidemiology and end results (SEER) program 1973–1991. Cancer 79(3):564–573
Ibrahimpasic T, Ghossein R, Carlson DL, Nixon I, Palmer FL, Shaha AR, Patel SG, Tuttle RM, Shah JP, Ganly I (2014) Outcomes in patients with poorly differentiated thyroid carcinoma. J Clin Endocrinol Metab 99(4):1245–1252. doi:10.1210/jc.2013-3842
Grogan RH, Kaplan SP, Cao H, Weiss RE, Degroot LJ, Simon CA, Embia OM, Angelos P, Kaplan EL, Schechter RB (2013) A study of recurrence and death from papillary thyroid cancer with 27 years of median follow-up. Surgery 154 (6):1436–1446. doi:10.1016/j.surg.2013.07.008. discussion 1446–1437
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No financial support or funding.
Conflict of interest
No conflict of interest.
Ethics
This article does not contain any studies with animals performed by any of the authors. This study has been approved by the Danish Data Protection Agency and The Regional Scientific Ethical Committees for Southern Denmark.
Informed consent
For this type of study formal consent is not required.
Disclosure statement
No competing financial interests exist. No writing assistance used.
Additional information
The study is from the Department of ORL Head & Neck Surgery, Odense University Hospital, Odense, Denmark.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Skansing, D.B., Londero, S.C., Asschenfeldt, P. et al. Nonanaplastic follicular cell-derived thyroid carcinoma: mitosis and necrosis in long-term follow-up. Eur Arch Otorhinolaryngol 274, 2541–2548 (2017). https://doi.org/10.1007/s00405-017-4527-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-017-4527-6