
Abstract
Background
Device therapy in addition to medical treatment improves prognosis in a subset of patients with heart failure and reduced ejection fraction. However, some patients remain symptomatic or their heart failure even progresses despite cardiac resynchronization therapy (CRT). The aim of the study was to evaluate the proportion of patients who could benefit from optimization of medical therapy using sacubitril/valsartan, ivabradine, or both following CRT implantation.
Methods
We conducted a post hoc analysis of a single-centre, patient and outcome-assessor blinded, randomized-controlled trial, in which patients scheduled for CRT were randomized to empiric (n = 93) or imaging-guided left-ventricular lead placement (n = 89). All patients underwent clinical evaluation and blood sampling at baseline and 6 months following CRT implantation. The proportion of patients meeting the indication for sacubitril/valsartan (irrespective of angiotensin-converting enzyme inhibitor or angiotensin 2 receptor blocker dosage) and/or ivabradine according to current guidelines was evaluated at baseline and after 6 months.
Results
Of 182 patients with an indication for CRT, 146 (80%) also had an indication for optimization of medical therapy at baseline by adding sacubitril/valsartan, ivabradine, or both. Of the 179 survivors at 6 months, 136 (76%) were still symptomatic after device implantation; of these, 51 (38%) patients had an indication for optimization of medical therapy: sacubitril/valsartan in 37 (27%), ivabradine in 7 (5%), and both drugs in 7 (5%) patients. Seven (18%) patients without indication at baseline developed an indication for medical optimization 6 months after CRT implantation.
Conclusion
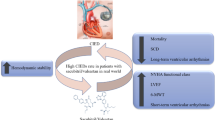
In the present study, 38% of those who remained symptomatic 6 months after CRT implantation were eligible for optimization of medical therapy with sacubitril/valsartan, ivabradine, or both. Patients with CRT may benefit from systematic follow-up including evaluation of medical treatment.
Graphic abstract

Similar content being viewed by others


Abbreviations
- ACE-I:
-
Angiotensin-converting enzyme inhibitors
- ARB:
-
Aldosterone receptor blocker
- ARNI:
-
Angiotensin receptor neprilysin inhibitor
- BNP:
-
Brain natriuretic peptide
- CRT:
-
Cardiac resynchronization therapy
- ICD:
-
Implantable cardioverter-defibrillator
- LVEF:
-
Left-ventricular ejection fraction
- MRA:
-
Mineralocorticoid antagonist
- NT-proBNP:
-
N-terminal pro-brain natriuretic peptide
- NYHA:
-
New York Heart Association
References
The SOLVD Investigators (1991) Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med 325(5):293–302
MERIT-HF Study Group (1999) Effect of metoprolol CR/XL in chronic heart failure: metoprolol CR/XL randomised intervention trial in congestive heart failure (MERIT-HF). Lancet 353(9169):2001–2007
Pitt B, Zannad F, Remme WJ et al (1999) The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med 341(10):709–717
Cleland JG, Daubert JC, Erdmann E et al (2005) The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med 352(15):1539–1549
Moss AJ, Hall WJ, Cannom DS et al (2009) Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med 361(14):1329–1338
Moss AJ, Zareba W, Hall WJ et al (2002) Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med 346(12):877–883
Okumura N, Jhund PS, Gong J et al (2016) Importance of clinical worsening of heart failure treated in the outpatient setting: evidence from the prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure trial (PARADIGM-HF). Circulation 133(23):2254–2262
Packer M, McMurray JJ, Desai AS et al (2015) Angiotensin receptor neprilysin inhibition compared with enalapril on the risk of clinical progression in surviving patients with heart failure. Circulation 131(1):54–61
Ponikowski P, Voors AA, Anker SD et al (2016) ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 18(8):891–975
McMurray JJ, Packer M, Desai AS et al (2014) Angiotensin–neprilysin inhibition versus enalapril in heart failure. N Engl J Med 371(11):993–1004
Swedberg K, Komajda M, Bohm M et al (2010) Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet 376(9744):875–885
Martens P, Nuyens D, Rivero-Ayerza M et al (2019) Sacubitril/valsartan reduces ventricular arrhythmias in parallel with left ventricular reverse remodeling in heart failure with reduced ejection fraction. Clin Res Cardiol 108(10):1074–1082
McMurray JJ, Adamopoulos S, Anker SD et al (2012) ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the task force for the diagnosis and treatment of acute and chronic heart failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J 33(14):1787–1847
Sommer A, Kronborg MB, Poulsen SH et al (2013) Empiric versus imaging guided left ventricular lead placement in cardiac resynchronization therapy (ImagingCRT): study protocol for a randomized controlled trial. Trials 14:113
McMurray JJ, Packer M, Desai AS et al (2013) Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-converting enzyme inhibition in patients with chronic systolic heart failure: rationale for and design of the prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure trial (PARADIGM-HF). Eur J Heart Fail 15(9):1062–1073
Sommer A, Kronborg MB, Norgaard BL et al (2016) Multimodality imaging-guided left ventricular lead placement in cardiac resynchronization therapy: a randomized controlled trial. Eur J Heart Fail 18(11):1365–1374
Ponikowski P, Voors AA, Anker SD et al (2016) 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 37(27):2129–2200
Juenger J, Schellberg D, Kraemer S et al (2002) Health related quality of life in patients with congestive heart failure: comparison with other chronic diseases and relation to functional variables. Heart 87(3):235–241
Soto GE, Jones P, Weintraub WS, Krumholz HM, Spertus JA (2004) Prognostic value of health status in patients with heart failure after acute myocardial infarction. Circulation 110(5):546–551
Ekman I, Chassany O, Komajda M et al (2011) Heart rate reduction with ivabradine and health related quality of life in patients with chronic heart failure: results from the SHIFT study. Eur Heart J 32(19):2395–2404
Lewis EF, Claggett BL, McMurray JJV et al (2017) Health-related quality of life outcomes in PARADIGM-HF. Circ Heart Fail 10(8):e003430
Bristow MR, Saxon LA, Boehmer J et al (2004) Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med 350(21):2140–2150
Veazie PJ, Noyes K, Li Q et al (2012) Cardiac resynchronization and quality of life in patients with minimally symptomatic heart failure. J Am Coll Cardiol 60(19):1940–1944
Martens P, Verbrugge FH, Nijst P et al (2017) Feasibility and association of neurohumoral blocker up-titration after cardiac resynchronization therapy. J Card Fail 23(8):597–605
Schmidt S, Hurlimann D, Starck CT et al (2014) Treatment with higher dosages of heart failure medication is associated with improved outcome following cardiac resynchronization therapy. Eur Heart J 35(16):1051–1060
Witt CT, Kronborg MB, Nohr EA, Mortensen PT, Gerdes C, Nielsen JC (2015) Optimization of heart failure medication after cardiac resynchronization therapy and the impact on long-term survival. Eur Heart J Cardiovasc Pharmacother 1(3):182–188
Leyva F, Zegard A, Okafor O et al (2018) Survival after cardiac resynchronization therapy: results from 50 084 implantations. Europace 21(5):754–762
Hamed S, Schmack B, Mueller F et al (2019) Implementation of an intensified outpatient follow-up protocol improves outcomes in patients with ventricular assist devices. Clin Res Cardiol. https://doi.org/10.1007/s00392-019-01451-9
Funding
The ImagingCRT study was funded by Aarhus University, the Danish Heart Foundation (11-04-R84-A3234-22641), the Danish Council for Independent Research (11-107461), Central Denmark Region (1-45-72-4-09), Eva and Henry Frænkels Foundation, and Fabrikant Karl G. Andersens Foundation. Sponsors were not involved in the design of the study, recruitment or patient investigations, nor in analysis, interpretation of data, and writing of the report.
Author information
Authors and Affiliations
Contributions
AJ, KP, and RRN were responsible for the conception and design of the study, analysis and interpretation of data, and drafting of the manuscript. AS and JCN were responsible for data acquisition. All authors have critically revised the manuscript for important intellectual content and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
Professor John J. V. McMurray’s employer, Glasgow University, has been paid by Novartis for his time spent as Principal Investigator/Executive/Steering Committee member for a number of clinical trials using sacubitril/valsartan and meetings and lectures related to sacubitril/valsartan. The Novo Nordisk Foundation (NNF16OC0018658) financially supports Professor Jens Cosedis Nielsen. The other authors report no conflicts of interest.
Data sharing statement
Raw data and statistical coding are available from the corresponding author at kpryds@clin.au.dk
Rights and permissions
About this article

Cite this article
Jorsal, A., Pryds, K., McMurray, J.J.V. et al. Optimizing heart failure treatment following cardiac resynchronization therapy. Clin Res Cardiol 109, 638–645 (2020). https://doi.org/10.1007/s00392-019-01553-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-019-01553-4