
Abstract
Purpose
Secondary non-response to infliximab (IFX) in patients with Crohn’s disease (CD) is so common that prediction of non-response is required to adopt the optimal therapy for an individual patient.
Methods
The clinical model was constructed in a training cohort. Clinical features, serological parameters, and genetic biomarkers at week 14 IFX therapy were obtained as predictors. Secondary non-response was defined at week 54. Univariate analysis was first performed to eliminate irrelevant predictors with non-response. Then, a logistic regression model was developed by using predictors with P < 0.1 in a univariate analysis. Finally, the model was validated with reference to its discrimination, calibration, and decision curve analysis (DCA).
Results
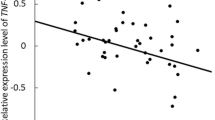
In a univariate analysis, erythrocyte sedimentation rate (ESR), the previous surgery, disease location, C-reactive protein (CRP), and TNFRSF1B (676 T>G) were found associated with secondary non-response to IFX. Logistic regression analysis with stepwise backward selection P < 0.05 then identified that ESR, the previous surgery, CRP, and TNFRSF1B (676 T>G) could serve as independent predictors, and a clinical model was developed based on the above predictors. Model 2 with TNFRSF1B (676 T>G) incorporated demonstrated more satisfactory discrimination (P = 0.029), better calibration (U P2 > 0.05), and higher clinical value in the validation cohort.
Conclusions
The study presents a model to predict non-response to IFX in CD, which incorporates previous surgery, ESR, CRP, and TNFRSF1B (676 T>G). This model can be used to help clinicians adjust the therapeutic strategy and CD patients avoid unnecessary exposure to IFX.




Similar content being viewed by others


References
Veauthier B, Hornecker JR (2018) Crohn’s disease: diagnosis and management. Am Fam Physician 98(11):661–669
D’Haens G, Vermeire S, Lambrecht G, Baert F, Bossuyt P, Pariente B, Buisson A, Bouhnik Y, Filippi J, van der Woude J, Van Hootegem P, Moreau J, Louis E, Franchimont D, De Vos M, Mana F, Peyrin-Biroulet L, Brixi H, Allez M, Caenepeel P, Aubourg A, Oldenburg B, Pierik M, Gils A, Chevret S, Laharie D, Détré P, Bertin M-J, Williams S (2018) Increasing infliximab dose based on symptoms, biomarkers, and serum drug concentrations does not increase clinical, endoscopic, and corticosteroid-free remission in patients with active luminal Crohn’s disease. Gastroenterology 154(5):1343–1351.e1341. https://doi.org/10.1053/j.gastro.2018.01.004
Singh S, George J, Boland BS, Vande Casteele N, Sandborn WJ (2018) Primary non-response to tumor necrosis factor antagonists is associated with inferior response to second-line biologics in patients with inflammatory bowel diseases: a systematic review and meta-analysis. J Crohns Colitis 12(6):635–643. https://doi.org/10.1093/ecco-jcc/jjy004
Danese S, Sandborn WJ, Colombel JF, Vermeire S, Glover SC, Rimola J, Siegelman J, Jones S, Bornstein JD, Feagan BG (2019) Endoscopic, radiologic, and histologic healing with vedolizumab in patients with active Crohn’s disease. Gastroenterology 157(4):1007–1018.e1007. https://doi.org/10.1053/j.gastro.2019.06.038
Feagan BG, Sandborn WJ, Gasink C, Jacobstein D, Lang Y, Friedman JR, Blank MA, Johanns J, Gao LL, Miao Y, Adedokun OJ, Sands BE, Hanauer SB, Vermeire S, Targan S, Ghosh S, de Villiers WJ, Colombel JF, Tulassay Z, Seidler U, Salzberg BA, Desreumaux P, Lee SD, Loftus EV Jr, Dieleman LA, Katz S, Rutgeerts P (2016) Ustekinumab as induction and maintenance therapy for Crohn’s disease. N Engl J Med 375(20):1946–1960. https://doi.org/10.1056/NEJMoa1602773
Dulai PS, Boland BS, Singh S, Chaudrey K, Koliani-Pace JL, Kochhar G, Parikh MP, Shmidt E, Hartke J, Chilukuri P, Meserve J, Whitehead D, Hirten R, Winters AC, Katta LG, Peerani F, Narula N, Sultan K, Swaminath A, Bohm M, Lukin D, Hudesman D, Chang JT, Rivera-Nieves J, Jairath V, Zou GY, Feagan BG, Shen B, Siegel CA, Loftus EV Jr, Kane S, Sands BE, Colombel JF, Sandborn WJ, Lasch K, Cao C (2018) Development and validation of a scoring system to predict outcomes of vedolizumab treatment in patients with Crohn’s disease. Gastroenterology 155(3):687–695.e610. https://doi.org/10.1053/j.gastro.2018.05.039
Billiet T, Papamichael K, de Bruyn M, Verstockt B, Cleynen I, Princen F, Singh S, Ferrante M, Van Assche G, Vermeire S (2015) A matrix-based model predicts primary response to infliximab in Crohn’s disease. J Crohns Colitis 9(12):1120–1126. https://doi.org/10.1093/ecco-jcc/jjv156
Gisbert JP, Chaparro M (2019) Predictors of primary response to biologic treatment [anti-TNF, vedolizumab, and ustekinumab] in patients with inflammatory bowel disease: from basic science to clinical practice. J Crohn's Colitis. https://doi.org/10.1093/ecco-jcc/jjz195
Kennedy NA, Heap GA, Green HD, Hamilton B, Bewshea C, Walker GJ, Thomas A, Nice R, Perry MH, Bouri S, Chanchlani N, Heerasing NM, Hendy P, Lin S, Gaya DR, Cummings JRF, Selinger CP, Lees CW, Hart AL, Parkes M, Sebastian S, Mansfield JC, Irving PM, Lindsay J, Russell RK, McDonald TJ, McGovern D, Goodhand JR, Ahmad T (2019) Predictors of anti-TNF treatment failure in anti-TNF-naive patients with active luminal Crohn’s disease: a prospective, multicentre, cohort study. Lancet Gastroenterol Hepatol 4(5):341–353. https://doi.org/10.1016/s2468-1253(19)30012-3
Magro F, Rodrigues-Pinto E, Santos-Antunes J, Vilas-Boas F, Lopes S, Nunes A, Camila-Dias C, Macedo G (2014) High C-reactive protein in Crohn’s disease patients predicts nonresponse to infliximab treatment. J Crohns Colitis 8(2):129–136. https://doi.org/10.1016/j.crohns.2013.07.005
Medrano LM, Taxonera C, Márquez A, Barreiro-de Acosta M, Gómez-García M, González-Artacho C, Pérez-Calle JL, Bermejo F, Lopez-Sanromán A, Martín Arranz MD, Gisbert JP, Mendoza JL, Martín J, Urcelay E, Núñez C (2014) Role of TNFRSF1B polymorphisms in the response of Crohn’s disease patients to infliximab. Hum Immunol 75(1):71–75. https://doi.org/10.1016/j.humimm.2013.09.017
Collins GS, Reitsma JB, Altman DG, Moons KG (2015) Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ 350:g7594. https://doi.org/10.1136/bmj.g7594
Vrieze SI (2012) Model selection and psychological theory: a discussion of the differences between the Akaike information criterion (AIC) and the Bayesian information criterion (BIC). Psychol Methods 17(2):228–243. https://doi.org/10.1037/a0027127
Kramer AA, Zimmerman JE (2007) Assessing the calibration of mortality benchmarks in critical care: the Hosmer-Lemeshow test revisited. Crit Care Med 35(9):2052–2056. https://doi.org/10.1097/01.Ccm.0000275267.64078.B0
Van Calster B, Wynants L, Verbeek JFM, Verbakel JY, Christodoulou E, Vickers AJ, Roobol MJ, Steyerberg EW (2018) Reporting and interpreting decision curve analysis: a guide for investigators. Eur Urol 74(6):796–804. https://doi.org/10.1016/j.eururo.2018.08.038
Rogler G (2019) JAK efficacy in Crohn’s disease. J Crohns Colitis. https://doi.org/10.1093/ecco-jcc/jjz186
Qasem A, Ramesh S, Naser SA (2019) Genetic polymorphisms in tumour necrosis factor receptors (TNFRSF1A/1B) illustrate differential treatment response to TNFα inhibitors in patients with Crohn’s disease. BMJ Open Gastroenterol 6(1):e000246. https://doi.org/10.1136/bmjgast-2018-000246
Chen W, Xu H, Wang X, Gu J, Xiong H, Shi Y (2015) The tumor necrosis factor receptor superfamily member 1B polymorphisms predict response to anti-TNF therapy in patients with autoimmune disease: a meta-analysis. Int Immunopharmacol 28(1):146–153. https://doi.org/10.1016/j.intimp.2015.05.049
Reinisch W, Wang Y, Oddens BJ, Link R (2012) C-reactive protein, an indicator for maintained response or remission to infliximab in patients with Crohn’s disease: a post-hoc analysis from ACCENT I. Aliment Pharmacol Ther 35(5):568–576. https://doi.org/10.1111/j.1365-2036.2011.04987.x
Jurgens M, Mahachie John JM, Cleynen I, Schnitzler F, Fidder H, van Moerkercke W, Ballet V, Noman M, Hoffman I, van Assche G, Rutgeerts PJ, van Steen K, Vermeire S (2011) Levels of C-reactive protein are associated with response to infliximab therapy in patients with Crohn’s disease. Clin Gastroenterol Hepatol 9(5):421–427.e421. https://doi.org/10.1016/j.cgh.2011.02.008
Miyoshi J, Hisamatsu T, Matsuoka K, Naganuma M, Maruyama Y, Yoneno K, Mori K, Kiyohara H, Nanki K, Okamoto S, Yajima T, Iwao Y, Ogata H, Hibi T, Kanai T (2014) Early intervention with adalimumab may contribute to favorable clinical efficacy in patients with Crohn’s disease. Digestion 90(2):130–136. https://doi.org/10.1159/000365783
Wong U, Cross RK (2017) Primary and secondary nonresponse to infliximab: mechanisms and countermeasures. Expert Opin Drug Metab Toxicol 13(10):1039–1046. https://doi.org/10.1080/17425255.2017.1377180
Matsuoka K, Hamada S, Shimizu M, Nanki K, Mizuno S, Kiyohara H, Arai M, Sugimoto S, Iwao Y, Ogata H, Hisamatsu T, Naganuma M, Kanai T, Mochizuki M, Hashiguchi M (2018) Factors predicting the therapeutic response to infliximab during maintenance therapy in Japanese patients with Crohn’s disease. PLoS One 13(10):e0204632. https://doi.org/10.1371/journal.pone.0204632
Juillerat P, Sokol H, Froehlich F, Yajnik V, Beaugerie L, Lucci M, Burnand B, Macpherson AJ, Cosnes J, Korzenik JR (2015) Factors associated with durable response to infliximab in Crohn’s disease 5 years and beyond: a multicenter international cohort. Inflamm Bowel Dis 21(1):60–70. https://doi.org/10.1097/mib.0000000000000225
Huang YQ, Liang CH, He L, Tian J, Liang CS, Chen X, Ma ZL, Liu ZY (2016) Development and validation of a radiomics nomogram for preoperative prediction of lymph node metastasis in colorectal cancer. J Clin Oncol 34(18):2157–2164. https://doi.org/10.1200/jco.2015.65.9128
Gonczi L, Bessissow T, Lakatos PL (2019) Ver(s)ifying the efficacy of vedolizumab therapy on mucosal healing in patients with Crohn’s disease. Gastroenterology 157(4):925–927. https://doi.org/10.1053/j.gastro.2019.07.032
Oshima S, Watanabe M (2018) Genetic and environmental factors drive personalized medicine for Crohn’s disease. J Clin Invest 128(11):4758–4760. https://doi.org/10.1172/jci124303
Author information
Authors and Affiliations
Contributions
LX performed the statistical procedure and draft the article. JS designed this study, and QZ helped edit the manuscript. The final version of the manuscript was approved by all authors.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
This study was approved by the ethics review board in Renji Hospital, School of Medicine, Shanghai Jiao Tong University.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Xu, L., Shen, J. & Zheng, Q. Development of a clinical model to predict secondary non-response of infliximab treatment in Crohn’s disease. Int J Colorectal Dis 35, 2019–2026 (2020). https://doi.org/10.1007/s00384-020-03679-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-020-03679-8