
Abstract
Purpose
Intraoperative chest tubes (IOCTs) can be placed during esophageal atresia/tracheoesophageal fistula (EA/TEF) repair to control pneumothoraces and detect esophageal leaks, potentially preventing the need for postoperative chest tubes (POCTs). However, data are lacking regarding IOCTs’ effect. We hypothesized that IOCT placement would not reduce the risk of POCT placement and would increase hospital length of stay (LOS).
Methods
This was a single-center case-control study of type C EA/TEF patients repaired at a tertiary referral center between 2006 and 2017. Postoperative complications of patients who received IOCTs (n = 83) were compared to that of patients who did not receive IOCTs (n = 26). Patients were compared via propensity score matching. Additionally, sensitivity analyses excluding low birth weight (LBW) patients and patients undergoing delayed esophageal anastomosis were also performed.
Results
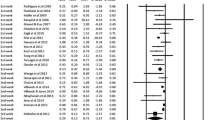
There was no significant difference in rates of pneumothoraces or esophageal leaks between the IOCT and no-IOCT groups, nor were either of these complications detected earlier in the IOCT group. Rates of POCT placement and mortality also did not differ between groups. IOCT patients were associated with increased hospital LOS (28 vs 15.5 days, p < 0.001) and esophageal strictures (30% vs 8%, p = 0.04) requiring a return to the operating room (RTOR).
Conclusion
IOCTs did not improve outcomes in EA/TEF repair. IOCTs seem associated with increased LOS and ROTR for esophageal stricture, suggesting that IOCTs may not be beneficial after EA/TEF repair.

Similar content being viewed by others


References
Wang B, Tashiro J, Allan BJ, Sola JE, Pariph PP, Hogan AR, Neville HL, Perez EA (2014) A nationwide analysis of clinical outcomes among newborns with esophageal atresia and tracheoesophageal fistulas in the United States. J Surg Res 190(2):604–612. https://doi.org/10.1016/j.jss.2014.04.033
Lal D, Miyano G, Juang D, Sharp NE, St Peter SD (2013) Current patterns of practice and technique in the repair of esophageal atresia and tracheoesophageal fistula: an IPEG survey. J Laproendosc Adv Surg Tech A 23(7):635–638. https://doi.org/10.1089/lap.2013.0210
Shawyer AC, Pemberton J, Flageole HH (2014) Post-operative management of esophageal atresia-tracheoesophageal fistula and gastroesophageal reflux: a Canadian Association of Pediatric Surgeons annual meeting survey. J Pediatr Surg 49(5):716–719. https://doi.org/10.1016/j.jpedsurg.2014.02.052
McCallion WA, Hannon RJ, Boston VE (1992) Prophylactic extrapleural chest drainage following repair of esophageal atresia: is it necessary? J Pediatr Surg 27(5):561
Fowler CL (1995) Subclavian artery compression from a chest tube after thoracotomy in a premature infant. Pediatr Radiol 25(6):458–459
Johnson JF, Wright DR (1990) Chest tube perforation of esophagus following repair of esophageal atresia. J Pediatr Surg 25(12):1227–1230
Aslanabadi S, Jamshidi M, Tubbs RS, Shoja MM (2009) The role of prophylactic chest drainage in the operative management of esophageal atresia with tracheoesophageal fistula. Pediatr Surg Int 25(4):365–368. https://doi.org/10.1007/s00383-009-2345-7
Gawad N, Wayne C, Bass J, Nasr A (2018) A chest tube may not be needed after surgical repair of esophageal atresia and tracheoesophageal fistula. Pediatr Surg Int 34(9):967–970. https://doi.org/10.1007/s00383-018-4307-4
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde NG (2009) Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 42(2):377–381. https://doi.org/10.1016/j.jbi.2008.08.010
Gu X, Rosenbaum PR (1993) Comparison of multivariate matching methods: structures, distances and algorithms. J Comput Graph Stat 2:405–420
R Core Team (2018). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/.
Kay SM, Shaw K (1999) Revisiting the role of routine retropleural drainage after repair of esophageal atresia with distal tracheoesophageal fistula. J Pediatr Surg 34(7):1082–1085. https://doi.org/10.1016/S0022-3468(99)90571-7
Paramalingam S, Burge DM, Stanton MP (2013) Operative intercostal chest drain is not required following extrapleural or transpleural esophageal atresia repair. Eur J Pediatr Surg 23(4):273–275. https://doi.org/10.1055/s-0032-1330845
Author information
Authors and Affiliations
Contributions
Conceptualization and methodology: Christopher P. Gayer; Methodology: Joanna C. Lim, Jamie M. Golden, Patrick T. Delaplain, Michelle V.L. Nguyen; Formal analysis and investigation: Patrick T. Delaplain, Michelle V.L. Nguyen; Writing-original draft preparation: Michelle V.L. Nguyen; Writing-review and editing: Michelle V.L. Nguyen, Christopher P. Gayer, Patrick T. Delaplain; Supervision: Christopher P. Gayer.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no disclosures or conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (include the name of committee + reference number) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Nguyen, M.V.L., Delaplain, P.T., Lim, J.C. et al. The value of prophylactic chest tubes in tracheoesophageal fistula repair. Pediatr Surg Int 36, 687–696 (2020). https://doi.org/10.1007/s00383-020-04664-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-020-04664-6