
Abstract
Background
Retroperitoneal laparoscopic adrenalectomy is gaining traction as a minimally invasive technique. One of the purported relative contraindications is BMI given the smaller working space. We hypothesize that other anthropometric measurements may be better predictors of operative time.
Methods
An IRB-approved, single-institution, retrospective study of 83 patients who underwent laparoscopic retroperitoneal adrenalectomy evaluated the association of anthropometric measurements taken from cross-sectional imaging and the primary outcome of operative time. Descriptive statistics were performed with Wilcoxon rank-sum test for continuous variables (median; IQR) and Chi-square (n; %) for categorical variables. A linear random effects model was used to model operative time.
Results
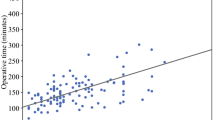
The majority of the patients were white (40; 48.2%) women (46; 55.4%) with a median age of 54 with interquartile range (IQR) of 43–63 and a median BMI of 27.8 (IQR 21.2–38.6). On univariable analysis, factors that led to longer operative time included right-sided operation (p = 0.04), male gender (p < 0.01), clinical diagnosis (p < 0.01), waist area (p < 0.01), waist/hip ratio (p < 0.01), periadrenal volume (p < 0.01), posterior adiposity index (PAI) (p < 0.01) and BMI (p < 0.01). Only side, order of operation, and periadrenal fat volume (p < 0.01, p = 0.02 and p < 0.01, respectively) remained independent predictors of increased operative time on multivariable analysis.
Conclusion
This study demonstrates that anthropometric measurements, specifically periadrenal fat volume, and side of operation, are better predictors for increased operative time in laparoscopic retroperitoneal adrenalectomies than BMI. This information can help facilitate appropriate patient selection for this operative approach.



Similar content being viewed by others


References
Carr AA, Wang TS (2016) Minimally invasive adrenalectomy. Surg Oncol Clin N Am 25(1):139–152
Kebebew E, Siperstein AE, Duh QY (2001) Laparoscopic adrenalectomy: the optimal surgical approach. J Laparoendosc Adv Surg Tech A 11(6):409–413
Lee J, El-Tamer M, Schifftner T et al (2008) Open and laparoscopic adrenalectomy: analysis of the national surgical quality improvement program. J Am Coll Surg 206(5):953–959 (discussion 959–961)
Marek-Safiejko M, Safiejko K, Lukaszewicz J et al (2016) A comparison of two approaches to laparoscopic adrenalectomy: lateral transperitoneal versus posterior retroperitoneal approach. Adv Clin Exp Med 25(5):829–835
Chen W, Li F, Chen D et al (2013) Retroperitoneal versus transperitoneal laparoscopic adrenalectomy in adrenal tumor: a meta-analysis. Surg Laparosc Endosc Percutan Tech 23(2):121–127
Epelboym I, Digesu CS, Johnston MG et al (2014) Expanding the indications for laparoscopic retroperitoneal adrenalectomy: experience with 81 resections. J Surg Res 187(2):496–501
Arezzo A, Bullano A, Cochetti G et al (2018) Transperitoneal versus retroperitoneal laparoscopic adrenalectomy for adrenal tumours in adults. Cochrane Database Syst Rev 12:CD011668
Lairmore TC, Folek J, Govednik CM, Snyder SK (2016) Improving minimally invasive adrenalectomy: selection of optimal approach and comparison of outcomes. World J Surg 40(7):1625–1631. https://doi.org/10.1007/s00268-016-3471-8
Mohammadi-Fallah MR, Mehdizadeh A, Badalzadeh A et al (2013) Comparison of transperitoneal versus retroperitoneal laparoscopic adrenalectomy in a prospective randomized study. J Laparoendosc Adv Surg Tech A 23(4):362–366
Vrielink OM, Engelsman AF, Hemmer PHJ et al (2018) Multicentre study evaluating the surgical learning curve for posterior retroperitoneoscopic adrenalectomy. Br J Surg 105(5):544–551
Guerrieri M, Campagnacci R, De Sanctis A, Baldarelli M, Coletta M, Perretta S (2008) The learning curve in laparoscopic adrenalectomy. J Endocrinol Invest 31(6):531–536
Lan BY, Taskin HE, Aksoy E et al (2015) Factors affecting the surgical approach and timing of bilateral adrenalectomy. Surg Endosc 29(7):1741–1745
Staren ED, Prinz RA (1996) Adrenalectomy in the era of laparoscopy. Surgery 120(4):706–709 (discussion 710–711)
Hu Q, Hang Z, Ho Y et al (2015) Impact of obesity on perioperative outcomes of retroperitoneal laparoscopic adrenalectomy. Urol Int 95(3):361–366
Inaishi T, Kikumori T, Takeuchi D et al (2018) Obesity does not affect peri- and postoperative outcomes of transabdominal laparoscopic adrenalectomy. Nagoya J Med Sci 80(1):21–28
Zonca P, Buzga M, Ihnat P, Martinek L (2015) Retroperitoneoscopic adrenalectomy in obese patients: is it suitable? Obes Surg 25(7):1203–1208
Agcaoglu O, Sahin DA, Siperstein A, Berber E (2012) Selection algorithm for posterior versus lateral approach in laparoscopic adrenalectomy. Surgery 151(5):731–735
Lindeman B, Gawande AA, Moore FD Jr, Cho NL, Doherty GM, Nehs MA (2019) The posterior adiposity index: a quantitative selection tool for adrenalectomy approach. J Surg Res 233:26–31
Walz MK, Alesina PF, Wenger FA et al (2006) Posterior retroperitoneoscopic adrenalectomy—results of 560 procedures in 520 patients. Surgery 140(6):943–948 (discussion 948–950)
Laird NM, Ware JH (1982) Random-effects models for longitudinal data. Biometrics 38(4):963–974
Mickey RM, Greenland S (1989) The impact of confounder selection criteria on effect estimation. Am J Epidemiol 129(1):125–137
Breslow NE, Clayton DG (1993) Approximate inference in generalized linear mixed models. J Am Stat Assoc 88(421):9–25
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Pearlstein, S.S., Kuo, J.H., Chabot, J.A. et al. Periadrenal Volume is a Better Predictor of Prolonged Operative Time in Laparoscopic Retroperitoneal Adrenalectomy than BMI. World J Surg 44, 578–584 (2020). https://doi.org/10.1007/s00268-019-05324-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-019-05324-0