
Abstract
Background
Dorsal nasal augmentation is an essential part of injection rhinoplasty on the Asian nose. Aesthetic physicians require detailed knowledge of the nasal anatomy to accurately and safely inject filler.
Methods
One hundred and thirty-five histological cross sections were examined from 45 longitudinal strips of soft tissue harvested from the midline of the nose, beginning from the glabella to the nasal tip. Muscles and nasal cartilage were used as landmarks for vascular identification.
Results
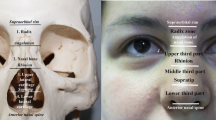
At the nasal tip, a midline longitudinal columellar artery with a diameter of 0.21 ± 0.09 mm was noted in 14 cadavers (31.1 %). At the infratip, subcutaneous tissue contained cavernous tissue similar to that of the nasal mucosa. The feeding arteries of these dilated veins formed arteriovenous shunts, into which retrograde injection of filler may be possible. All of the nasal arteries present were identified as subcutaneous arteries. They coursed mainly in the superficial layer of the subcutaneous tissues, with smaller branches forming subdermal plexuses. A substantial arterial anastomosis occurred at the supratip region, in which the artery lay in the middle of the subcutaneous tissue at the level of the major alar cartilages. These arteries had a diameter ranging between 0.4 and 0.9 mm and were found in 29 of 45 specimens (64.4 %). This was at the level midway between the rhinion above the supratip and the infratip. This anastomotic artery also crossed the midline at the rhinion superficial to the origin of the procerus on the lower end of the nasal bone. Here the arterial diameter ranged between 0.1 and 0.3 mm, which was not large enough to cause arterial emboli. Fascicular cross sections of the nasalis muscle directly covered the entire upper lateral cartilage. The subdermal tissue contained few layers of fat cells along with the occasional small artery. The procerus arose from the nasal bone and was continuous with the nasalis in 16 cadavers (35.6 %). There was fatty areolar tissue between the procerus and the periosteal layer and no significant arteries present. The procerus ascended beyond the brow to insert into the frontalis muscle with very few cutaneous insertions. The supratrochlear vessels and accompanying nerve were occasionally found on the surface of the frontalis muscle.
Conclusion
Most nasal arteries found in the midline are subcutaneous arteries. Filler should be injected deeply to avoid vascular injury leading to compromised perfusion at the dorsum or filler emboli at the nasal tip.
Level of Evidence V
This journal requires that the authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.









Similar content being viewed by others


References
Harrison DH (2013) Reflections on the open and closed rhinoplasty. J Plast Reconstr Aesthet Surg 66:1356–1359
Schuster B (2015) Injection rhinoplasty with hyaluronic acid and calcium hydroxyapatite: A retrospective survey investigating outcome and complication rates. Facial Plast Surg 31:301–307
Cassuto D (2009) The use of Dermicol-P35 dermal filler for nonsurgical rhinoplasty. Aesthet Surg J 29:S22–S24
Han X, Han X, Hu J, Cheng L, Li F (2015) Multiplane hyaluronic acid (EME) in female Chinese rhinoplasty using blunt and sharp needle technique. J Plast Reconstr Aesthet Surg. 68:1504–1509
Baptista C, Nguyen PSA, Desouches C, Magalon G, Bardot J, Casanova D (2013) Correction of sequelae of rhinoplasty by lipofilling. J Plast Reconstr Aesthet Surg 66:805–811
Humphrey CD, Arkins JP, Dayan SH (2009) Soft tissue fillers in the nose. Aesthet Surg J 29:477–484
Kurkjian TJ, Ahmad J, Rohrich RJ (2014) Soft-tissue fillers in rhinoplasty. Plast Reconstr Surg 133:21e–126e
Piggott JR, Yazdani A (2011) Hyaluronic acid used for the correction of nasal deviation in an 18-year-old Middle Eastern man. Can J Plast Surg 19:156–158
Pavicic T, Funt D (2013) Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol 13:295
Kim SN, Byun DS, Park JH, Han SW, Baik JS, Kim JY (2014) Panophthalmoplegia and vision loss after cosmetic nasal dorsum injection. J Clin Neurosci 21:678–680
DeLorenzi C (2013) Complications of injectable fillers, part I. Aesthetic Surg J 33:561–575
Beleznay K, Carruthers JD, Humphrey S, Jones D (2015) Avoiding and treating blindness from fillers: a review of the world literature. Dermatol Surg 41:1097–1117
Li X, Du L, Lu JJ (2015) A novel hypothesis of visual loss secondary to cosmetic facial filler injection. Ann Plast Surg 75(3):258–260
Saban Y, Andretto AC, Bouaziz D, Polselli R (2012) Nasal arterial vasculature: medical and surgical applications. Arch Facial Plast Surg 14:429–436
Mashiko T, Takanobu M, Harushi K, Harunosuke D, Kentaro K, Shinichiro K, Kahori K, Akira O, Kuni Y, Yoshimura K (2013) Semipermanent volumization by an absorbable filler. Plast Reconstr Surg Glob Open 1:1–11
Acknowledgments
Miss Yasmina M E Sahraoui from the University of Liverpool kindly revised this manuscript. Dr. Depicha Jindatip and Mrs. Vanida Buasorn kindly supported all histology cross sections and vascular endothelial staining.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest to disclose.
Rights and permissions
About this article

Cite this article
Tansatit, T., Moon, HJ., Rungsawang, C. et al. Safe Planes for Injection Rhinoplasty: A Histological Analysis of Midline Longitudinal Sections of the Asian Nose. Aesth Plast Surg 40, 236–244 (2016). https://doi.org/10.1007/s00266-016-0621-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-016-0621-1