
Abstract
Introduction
To introduce a drug to the market, it’s not mandatory for it to be more effective and safer than the current treatment for the same condition. Consequently, head-to-head studies between the two best treatments for the same condition are not required, and this could result in a lack of information for patients, clinicians, and decision-makers. This study aims to evaluate the presence of head-to-head studies among the drugs used for the treatment of non-small cell lung cancer (NSCLC).
Methods
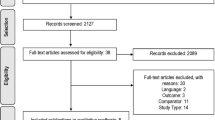
Taking into account the National Comprehensive Cancer Network (NCCN) guidelines updated to 2022, which list all available treatments for each NSCLC subtype, the search engine Pubmed and the platform clinicaltrials.gov were consulted to find all completed and ongoing head-to-head studies among various treatments for NSCLC.
Results
Among the anti-EGFR (epidermal growth factor receptor) drugs, 7 studies were found, with 6 completed and 5 registrational for drug commercialisation. No completed study to date has compared osimertinib and afatinib. For anti-ALK (anaplastic lymphoma kinase) drugs, 7 studies were found, with 5 completed. Alectinib, brigatinib, and lorlatinib have no completed comparison studies, but all were compared with crizotinib. Among various immunotherapy-based regimens, 5 studies were found, with only 1 completed. Therapeutic regimens based on pembrolizumab, atezolizumab, or the combination of nivolumab/ipilimumab have not been compared in studies published to date.
Conclusion
There are few head-to-head studies comparing treatments for NSCLC; there are no such studies between the latest generation of drugs. Consequently, ambiguous areas exist due to the lack of comparative studies among the available evidence, preventing the clinician’s choice of the most effective treatment and risking the patient receiving suboptimal therapy. Simultaneously, the price of the drug cannot be determined correctly, relying only on indirect evaluations from different trials. To dispel this uncertainty, it would be desirable to initiate a process that brings together the demands derived from clinical practice and clinical research to provide clinicians and patients with the best possible evidence.




Similar content being viewed by others


References
Sung H, Ferlay J, Siegel RL et al (2021) Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71(3):209–249
Falzone L, Salomone S, Libra M (2018) Evolution of cancer pharmacological treatments at the turn of the third millennium. Front Pharmacol 9:1300
Imyanitov EN, Iyevleva AG, Levchenko EV (2021) Molecular testing and targeted therapy for non-small cell lung cancer: current status and perspectives. Crit Rev Oncol Hematol 157:103194
Zhang Y, Zhang Z (2020) The history and advances in cancer immunotherapy: understanding the characteristics of tumor-infiltrating immune cells and their therapeutic implications. Cell Mol Immunol 17(8):807–821
Ettinger DS, Wood DE, Aisner DL et al (2022) Non-small cell lung cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 20(5):497–530
Reck M, Carbone DP, Garassino M, Barlesi F (2021) Targeting KRAS in non-small-cell lung cancer: recent progress and new approaches. Annals Oncol 32(9):1101–1110
Remon J, Hendriks LEL, Cardona AF, Besse B (2020) EGFR exon 20 insertions in advanced non-small cell lung cancer: a new history begins. Cancer Treat Rev 90:102105
Shaw AT, Engelman JA (2013) ALK in lung cancer: past, present, and future. J Clin Oncol 31(8):1105–1111
Leonetti A, Facchinetti F, Rossi G et al (2018) BRAF in non-small cell lung cancer (NSCLC): pickaxing another brick in the wall. Cancer Treat Rev 66:82–94
Bergethon K, Shaw AT, Ou SH et al (2012) ROS1 rearrangements define a unique molecular class of lung cancers. J Clin Oncol 30(8):863–870
Recondo G, Che J, Janne PA, Awad MM (2020) Targeting MET dysregulation in cancer. Cancer Discov 10(7):922–934
Harada G, Santini FC, Wilhelm C, Drilon A (2021) NTRK fusions in lung cancer: from biology to therapy. Lung Cancer 161:108–113
Belli C, Anand S, Gainor JF et al (2020) Progresses toward precision medicine in RET-altered solid tumors. Clin Cancer Res 26(23):6102–6111
Mazieres J, Drilon A, Lusque A et al (2019) Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Annal Oncol 30(8):1321–1328
Lisberg A, Cummings A, Goldman JW et al (2018) A phase II study of pembrolizumab in EGFR-mutant, PD-L1+, tyrosine kinase inhibitor naive patients with advanced NSCLC. J Thorac Oncol 13(8):1138–1145
Gainor JF, Shaw AT, Sequist LV et al (2016) EGFR mutations and ALK rearrangements are associated with low response rates to PD-1 pathway blockade in non-small cell lung cancer: a retrospective analysis. Clin Cancer Res 22(18):4585–4593
Felip E, Altorki N, Zhou C et al (2021) Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet 398(10308):1344–1357
Akinboro O, Vallejo JJ, Nakajima EC et al (2022) Outcomes of anti–PD-(L)1 therapy with or without chemotherapy (chemo) for first-line (1L) treatment of advanced non–small cell lung cancer (NSCLC) with PD-L1 score ≥ 50%: FDA pooled analysis. J Clin Oncol 40(16_suppl):9000–9000
Lasala R, Logreco A, Romagnoli A, Santoleri F, Musicco F, Costantini A (2020) Cancer drugs for solid tumors approved by the EMA since 2014: an overview of pivotal clinical trials. Eur J Clin Pharmacol 76(6):843–850
Hatswell AJ, Baio G, Berlin JA, Irs A, Freemantle N (2016) Regulatory approval of pharmaceuticals without a randomised controlled study: analysis of EMA and FDA approvals 1999–2014. BMJ Open 6(6):e011666
Ladanie A, Speich B, Briel M et al (2019) Single pivotal trials with few corroborating characteristics were used for FDA approval of cancer therapies. J Clin Epidemiol 114:49–59
Hilal T, Sonbol MB, Prasad V (2019) Analysis of control arm quality in randomized clinical trials leading to anticancer drug approval by the US Food and Drug Administration. JAMA Oncol 5(6):887–892
Rossi A, Aimar G, Audisio M et al (2023) Analysis of the adequacy of control arms in oncology randomised clinical trials published between 2017 and 2021: a meta-research study. Eur J Cancer
Del Fiol G, Workman TE, Gorman PN (2014) Clinical questions raised by clinicians at the point of care: a systematic review. JAMA Intern Med 174(5):710–718
Caldwell DM, Ades AE, Higgins JP (2005) Simultaneous comparison of multiple treatments: combining direct and indirect evidence. BMJ 331(7521):897–900
Kim H, Gurrin L, Ademi Z, Liew D (2014) Overview of methods for comparing the efficacies of drugs in the absence of head-to-head clinical trial data. Br J Clin Pharmacol 77(1):116–121
Mills EJ, Thorlund K, Ioannidis JP (2013) Demystifying trial networks and network meta-analysis. BMJ 346:f2914
Ramalingam SS, Vansteenkiste J, Planchard D et al (2020) Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med 382(1):41–50
Park K, Tan EH, O’Byrne K et al (2016) Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): a phase 2B, open-label, randomised controlled trial. Lancet Oncol 17(5):577–589
Wu YL, Cheng Y, Zhou X et al (2017) Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): a randomised, open-label, phase 3 trial. Lancet Oncol 18(11):1454–1466
Nakagawa K, Garon EB, Seto T et al (2019) Ramucirumab plus erlotinib in patients with untreated, EGFR-mutated, advanced non-small-cell lung cancer (RELAY): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol 20(12):1655–1669
Seto T, Kato T, Nishio M et al (2014) Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous non-small-cell lung cancer harbouring EGFR mutations (JO25567): an open-label, randomised, multicentre, phase 2 study. Lancet Oncol 15(11):1236–1244
Piccirillo MC, Bonanno L, Garassino MC et al (2022) Addition of Bevacizumab to Erlotinib as first-line treatment of patients with EGFR-mutated advanced nonsquamous NSCLC: the BEVERLY multicenter randomized phase 3 trial. J Thorac Oncol 17(9):1086–1097
Haratake N, Hayashi H, Shimokawa M et al (2022) Phase III clinical trial for the combination of Erlotinib plus Ramucirumab compared with Osimertinib in previously untreated advanced or recurrent non-small cell lung cancer positive for the L858R mutation of EGFR: REVOL858R (WJOG14420L). Clin Lung Cancer 23(3):e257–e263
Camidge DR, Kim HR, Ahn MJ et al (2018) Brigatinib versus Crizotinib in ALK-positive non-small-cell lung cancer. N Engl J Med 379(21):2027–2039
Shaw AT, Bauer TM, de Marinis F et al (2020) First-line Lorlatinib or Crizotinib in advanced ALK-positive lung cancer. N Engl J Med 383(21):2018–2029
Peters S, Camidge DR, Shaw AT et al (2017) Alectinib versus Crizotinib in untreated ALK-positive non-small-cell lung cancer. N Engl J Med 377(9):829–838
Hida T, Nokihara H, Kondo M et al (2017) Alectinib versus crizotinib in patients with ALK-positive non-small-cell lung cancer (J-ALEX): an open-label, randomised phase 3 trial. Lancet 390(10089):29–39
Zhou C, Kim SW, Reungwetwattana T et al (2019) Alectinib versus crizotinib in untreated Asian patients with anaplastic lymphoma kinase-positive non-small-cell lung cancer (ALESIA): a randomised phase 3 study. Lancet Respir Med 7(5):437–446
Popat S, Liu G, Lu S, Song G, Ma X, Yang JC (2021) Brigatinib vs alectinib in crizotinib-resistant advanced anaplastic lymphoma kinase-positive non-small-cell lung cancer (ALTA-3). Future Oncol 17(32):4237–4247
Targeted treatment for ALK positive patients who have previously been treated for non-squamous non-small cell lung cancer. https://classic.clinicaltrials.gov/ct2/show/NCT03737994. Published 2023. Updated 14 Apr 2023. Accessed 7 Aug 2023
Socinski MA, Jotte RM, Cappuzzo F et al (2018) Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med 378(24):2288–2301
Frost N, Bleckmann A, Griesinger F et al (2023) Rationale and design of the phase II ANTELOPE study of Atezolizumab, Carboplatin and nab-Paclitaxel vs. Pembrolizumab, platinum and pemetrexed in TTF-1 negative, metastatic lung adenocarcinoma (AIO-TRK-0122). Clin Lung Cancer
Immune profile selection by fraction of ctDNA in patients with advanced NSCLC treated with immunotherapy (G360-IIT). https://classic.clinicaltrials.gov/ct2/show/NCT05715229. Published 2023. Updated 6 Jul 2023. Accessed 2023
Testing the effects of MK-3475 (Pembrolizumab) with or without the usual chemotherapy treatment for patients 70 years of age and older with advanced non-small cell lung cancer. https://classic.clinicaltrials.gov/ct2/show/NCT04533451. Published 2023. Updated 18 Apr 2023. Accessed Aug 2023
Shiraishi Y, Hakozaki T, Nomura S et al (2022) A multicenter, randomized phase III study comparing platinum combination chemotherapy plus pembrolizumab with platinum combination chemotherapy plus Nivolumab and Ipilimumab for treatment-naive advanced non-small cell lung cancer without driver gene alterations: JCOG2007 (NIPPON Study). Clin Lung Cancer 23(4):e285–e288
Pemetrexed-free vs. Pemetrexed-based immunochemotherapy in metastatic TTF-1 negative lung adenocarcinoma (ANTELOPE). https://classic.clinicaltrials.gov/ct2/show/NCT05689671. Published 2023. Updated 19 Jan 2023. Accessed Aug 2023
Vokinger KN, Glaus CEG, Kesselheim AS, Serra-Burriel M, Ross JS, Hwang TJ (2023) Therapeutic value of first versus supplemental indications of drugs in US and Europe (2011–20): retrospective cohort study. BMJ 382:e074166
Garattini S, Bertele V (2007) How can we regulate medicines better? BMJ 335(7624):803–805
Wieseler B (2023) Patients need better treatments, not just more of the same. BMJ 382:1466
Naci H, Salcher-Konrad M, Kesselheim AS et al (2020) Generating comparative evidence on new drugs and devices before approval. Lancet 395(10228):986–997
Flacco ME, Manzoli L, Boccia S et al (2015) Head-to-head randomized trials are mostly industry sponsored and almost always favor the industry sponsor. J Clin Epidemiol 68(7):811–820
West HJ (2023) Clinical decision making in the real world-the perfect as the enemy of the good. JAMA Oncol
(EMA) EMA. Data analysis and real world interrogation network (DARWIN EU). https://www.ema.europa.eu/en/about-us/how-we-work/big-data/data-analysis-real-world-interrogation-network-darwin-eu. Published 2023. Accessed 7 Aug 2023
(FDA) USFDA. Real-world evidence. https://www.fda.gov/science-research/science-and-research-special-topics/real-world-evidence. Published 2023. Updated 2 May 2023. Accessed 7 Aug 2023
IQVIA (2023) Global oncology trends. https://www.iqvia.com/insights/the-iqvia-institute/reports/global-oncology-trends-2023. Published 2023. Updated 24 May 2023. Accessed 7 Aug 2023
Del Paggio JC, Sullivan R, Schrag D et al (2017) Delivery of meaningful cancer care: a retrospective cohort study assessing cost and benefit with the ASCO and ESMO frameworks. Lancet Oncol 18(7):887–894
Cohen D (2017) Cancer drugs: high price, uncertain value. BMJ 359:j4543
Angelis A, Polyakov R, Wouters OJ, Torreele E, McKee M (2023) High drug prices are not justified by industry’s spending on research and development. BMJ 380:e071710
Author information
Authors and Affiliations
Contributions
Ruggero Lasala and Felice Musicco contributed to the conception and design of the study; Ruggero Lasala, Alessia Romagnoli, Felice Musicco wrote the main manuscript; Ruggero Lasala, Alessia Romagnoli, Fiorenzo Santoleri, Valentina Isgrò, Corrado Confalonieri, Alberto Costantini, Fiorenza Enrico, Gianluca Russo, Felice Musicco contributed to the acquisition, analysis of the data; Ruggero Lasala, Alessia Romagnoli, Fiorenzo Santoleri, Valentina Isgrò, Corrado Confalonieri, Alberto Costantini, Fiorenza Enrico, Gianluca Russo, Piera Polidori, Alessandra Di Paolo, Francesco Malorgio, Giordano Beretta and Felice Musicco contributed to interpretation of data, reviewed and gave the final approval to the manuscript.
Corresponding author
Ethics declarations
Ethical approval
Considering that our study relies upon data relating to previously published clinical trials and did Fnot require patient involvement, we did not solicit an opinion from the Hospital Ethics Committee nor did we require the collection of informed consent from patients.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Lasala, R., Romagnoli, A., Santoleri, F. et al. The lack of head-to-head randomised trials and the consequences for patients and national health service: The case of non-small cell lung cancer. Eur J Clin Pharmacol 80, 519–527 (2024). https://doi.org/10.1007/s00228-024-03628-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-024-03628-2