
Abstract
Introduction and hypothesis
Obstetric anal sphincter injuries (OASIS) are associated with an increased risk of faecal incontinence after vaginal delivery. The aim of this retrospective population-based cohort study was to assess whether mediolateral episiotomy is associated with a reduction in the rate of OASIS during operative vaginal delivery.
Methods
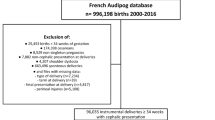
We used data from the Dutch Perinatal Registry (Perined) that includes records of almost all births between 2000 and 2010 in The Netherlands. In a cohort of 170,969 primiparous and multiparous women whose delivery was recorded, we estimated the association between mediolateral episiotomy and OASIS following both vacuum and forceps deliveries using univariate and multivariate logistic regression analysis.
Results
The incidences of OASIS following vacuum delivery in 130,157 primiparous women were 2.5% and 14% in those with and without a mediolateral episiotomy, respectively (adjusted OR 0.14, 95% CI 0.13–0.15), and in 29,183 multiparous women were 2.0% and 7.5%, respectively (adjusted OR 0.23, 95% CI 0.21–0.27). The incidences of OASIS following forceps delivery in 9,855 primiparous women were 3.4% and 26.7% in those with and without a mediolateral episiotomy, respectively (adjusted OR 0.09, 95% CI 0.07–0.11), and in 1,774 multiparous women were 2.6% and 14.2%, respectively (adjusted OR 0.13, 95% CI 0.08–0.22).
Conclusions
The use of a mediolateral episiotomy during both vacuum delivery and forceps delivery is associated with a fivefold to tenfold reduction in the rate of OASIS in primiparous and multiparous women.
Similar content being viewed by others


References
Mous M, Muller SA, De Leeuw JW. Long term effects of anal sphincter rupture during vaginal delivery: faecal incontinence and sexual complaints. BJOG. 2008;115:234–8.
Stedenfeldt M, Oian P, Gissler M, Blix E, Prhonen J. Risk factors for obstetric anal sphincter injury after a successful multicentre interventional programme. BJOG. 2014;121:83–91.
Ekeus C, Nilsson E, Gottvall K. Increasing incidence of anal sphincter tears among primiparas in Sweden: a population-based register study. Acta Obstet Gynecol Scand. 2008;87:564–73.
Baghestan E, Irgens LM, Børdahl PE, Rasmussen S. Trends in risk factors for obstetric anal sphincter injuries in Norway. Obstet Gynecol. 2010;116:25–34.
De Leeuw JW, Struijk PC, Vierhout ME, Wallenburg HC. Risk factors for third degree perineal ruptures during delivery. BJOG. 2001;108(4):383–7.
Murphy DJ, Macleod M, Bahl R, Goyder K, Howarth L, Strachan B. A randomised controlled trial of routine versus restrictive use of episiotomy at operative vaginal delivery: a multicentre pilot study. BJOG. 2008;115(13):1695–702.
Royal College of Obstetricians and Gynaecologists. Third and fourth degree perineal tears, management (Green Top guideline No. 29). London: Royal College of Obstetricians and Gynaecologists; 2015.
De Leeuw JW, de Wit C, Kuijken JP, Bruinse HW. Mediolateral episiotomy reduces the risk for anal sphincter injury during operative vaginal delivery. BJOG. 2008;115:104–8.
De Vogel J, Van der Leeuw-Van Beek A, Gietelink D, Vujkovic M, de Leeuw JW, Van Bavel J, et al. The effect of a mediolateral episiotomy during operative vaginal delivery on the risk of developing obstetrical anal sphincter injuries. Am J Obstet Gynecol. 2012;206:404.e1–e5.
Jangö H, Langhoff-Roos J, Rosthøj S, Sakse A. Modifiable risk factors of obstetric anal sphincter injury in primiparous women: a population-based cohort study. Am J Obstet Gynecol. 2014;210(1):59.e1–e6.
Räisänen S, Vehviläinen-Julkunen K, Cartwright R, Gissler M, Heinonen S. Vacuum-assisted deliveries and the risk of obstetric anal sphincter injuries – a retrospective register-based study in Finland. BJOG. 2012;119:1370–8.
Gurol-Urganci I, Cromwell DA, Edozien LC, Mahmood TA, Adams EJ, Richmond DH, et al. Third- and fourth-degree perineal tears among primiparous women in England between 2000 and 2012: time trends and risk factors. BJOG. 2013;120:1516–25.
Sagi-Dain L, Sagi S. Morbidity associated with episiotomy in vacuum delivery: a systematic review and meta-analysis. BJOG. 2015;122(8):1073–81.
The Netherlands Perinatal Registry. Perinatal care in the Netherlands 2010. Utrecht: The Netherlands Perinatal Registry; 2013.
Anthony S, van der Pal-de Bruin KM, Graafmans WC, Dorrepaal CA, Borkent-Polet M, Van Hemel OJ, et al. The reliability of perinatal and neonatal mortality rates: differential under-reporting in linked professional registers vs. Dutch civil registers. Paediatr Perinat Epidemiol. 2001;15(3):306–14.
Räisänen SH, Vehviläinen-Julkunen K, Gissler M, Heinonen S. Lateral episiotomy protects primiparous but not multiparous women from obstetric anal sphincter rupture. Acta Obstet Gynecol Scand. 2009;88:1365–72.
Altman D, Ragnar I, Ekström A, Tydén T. Anal sphincter lacerations and upright delivery postures – a risk analysis from a randomized controlled trial. Int Urogynecol J. 2007;18:141–6.
Baumann P, Hammoud AO, McNeeley SG, DeRose E, Kudish B, Hendrix S. Factors associated with anal sphincter laceration in 40,923 primiparous women. Int Urogynecol J. 2007;18:985–90.
Bodner-Adler B, Bodner K, Kaider A, Wagenbichler P, Leodolter S, Husslein P, et al. Risk factors for third-degree perineal tears in vaginal delivery, with an analysis of episiotomy types. Reprod Med. 2001;46(8):752–6.
Bender R, Blettner M. Calculating the ‘number needed to be exposed’ with adjustment for confounding variables in epidemiological studies. J Clin Epidemiol. 2002;55:525–30.
Eogan M, Daly L, O’Connell P, O’Herlihy C. Does the angle of episiotomy affect the incidence of anal sphincter injury? BJOG. 2006;113:190–4.
Pirhonen JP, Grenman SE, Haadem K, Gudmundsson S, Lindqvist P, Siihola S, et al. Frequency of anal sphincter rupture at delivery in Sweden and Finland – result of difference in manual help to the baby's head. Acta Obstet Gynecol Scand. 1998;77:974–7.
Jansova M, Kalis V, Rusavy Z, Zemcik R, Lobovsky L, Laine K. Modeling manual protection during delivery. Int Urogynecol J. 2014;25:65–71.
Räisänen S, Vehviläinen-Julkunen K, Cartwright R, Gissler M, Heinonen S. A prior cesarean section and incidence of obstetric anal sphincter injury. Int Urogynecol J. 2013;24(8):1331–9. doi:10.1007/s00192-012-2006-6.
Macleod M, Goyder K, Howarth L, Bahl R, Strachan B, Murphy D. Morbidity experienced by women before and after operative vaginal delivery: prospective cohort study nested within a two-centre randomised controlled trial of restrictive versus routine use of episiotomy. BJOG. 2013;120:1020–7.
Fodstad K, Staff AC, Laine K. Sexual activity and dyspareunia the first year postpartum in relation to degree of perineal trauma. Int Urogynecol J. 2016;27(10):1513–23.
Acknowledgments
We thank all Dutch midwives, obstetricians, neonatologists, and other perinatal health-care providers for the registration of perinatal information and Perined (www.perined.nl) for permission to use the registry data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
None.
Conflicts of interest
None.
Ethical approval
No ethical approval was needed as the analyses were based on anonymous registry data.
Rights and permissions
About this article

Cite this article
van Bavel, J., Hukkelhoven, C.W.P.M., de Vries, C. et al. The effectiveness of mediolateral episiotomy in preventing obstetric anal sphincter injuries during operative vaginal delivery: a ten-year analysis of a national registry. Int Urogynecol J 29, 407–413 (2018). https://doi.org/10.1007/s00192-017-3422-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-017-3422-4