
Abstract
Purpose
To describe injury incidence, time trends in injury incidence, and injury characteristics among Swedish Olympic athletes over 22 years based on insurance data, as a first step to inform injury preventive measures among Olympic athletes.
Methods
The cohort comprised 762 elite athletes (54% males; age 26.5 ± 5.9 years) in 38 sports in the Swedish Olympic Committee support program ‘Top and Talent’ between 1999 and 2020, with total 3427 athlete-years included. Acute and gradual onset injuries were reported to the insurance registry by the athletes’ medical staff.
Results
A total of 1635 injuries in 468 athletes were registered. The overall injury incidence was 47.7 injuries/100 athlete-years (one injury per athlete every second year). An increasing trend in injury incidence was observed in the first decade 2001 to 2010 (annual change 6.0%, 95% CI 3.3–8.8%), while in the second decade 2011 to 2020 no change was evident (0.4%, 95% CI − 1.9 to 2.7%). Gymnastics, tennis, and athletics had the highest incidence (100.0, 99.3, and 93.4 injuries/100 athlete-years, respectively). Among sport categories, mixed and power sports had the highest incidence (72.8 and 69.5 injuries/100 athlete-years, respectively). Higher incidences were seen in the younger age groups (≤ 25 years) in mixed and skill sports. The injury incidence was comparable between male and female athletes, and summer and winter sports. Most injuries occurred in the lower limb, and specifically the knee (24%), foot/ankle (15%) and spine/pelvis (13%).
Conclusion
The results on injury patterns in different sports and age groups may guide preventive focus for health and performance teams working with Olympic athletes.
Level of evidence
II.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Injuries entail major challenges for sports teams and athletes, as they have a negative impact on athletes’ health, sports performance, and success [5, 6, 12, 26]. Structured long-term injury surveillance is fundamental to better understand the injury burden and pattern, to generate ideas for injury prevention, and to evaluate the effects of interventions [24]. Long-term surveillance programmes have been established among elite athletes in sports such as football, rugby, and athletics and have provided increased knowledge of the injury burden in these sports [7, 8, 11, 14, 27]. For instance, based on FIFA injury surveillance there is evidence of reduced incidence of head injuries in professional football after introduction of a rule change penalizing direct and deliberate elbows to head with a red card [2].
For the 2008 Olympic Games, the International Olympic Committee implemented a health surveillance programme which has been conducted ever since [9, 10, 15, 19,20,21,22]. During the summer Olympic Games of 2016 and 2020 and the winter Olympic Games of 2014 and 2018, 8–12% of athletes suffered an injury [19,20,21,22]. This surveillance programme, however, only captures injuries occurring during the Olympic Games, while the injury rate and pattern outside this period is largely unknown. Injuries occurring outside the Olympic Games period could have an impact on athletes’ preparations for the Olympic Games, and more knowledge about injuries may help support athletes in their preparations, potentially reducing the injury burden and allowing better performance. Additionally, surveillance programmes may act as a first step to inform injury preventive measures. Many National Olympic Committees have support programmes for their Olympic candidates. In Norway, for example, a health monitoring programme was implemented in 2011 for the national Olympic and Paralympic candidates, which has provided further insights about injuries outside the Olympic Games period [4].
Insurance registries have been used to collect injury surveillance data [13, 16, 29, 30]. Most athletes in Sweden are insured by the same insurance company, where acute sport injuries have been registered consistently for over 20 years [30]. Previously this registry has been used to study sports injuries at a national level [29], but it has not been used to study injuries specifically occurring among elite Olympic athletes. The aims of this study were to: (1) describe the injury incidence and analyse time trends in injury incidence; and (2) describe injury types and locations, in different age groups, sexes, and sports among Swedish Olympic athletes based on insurance data.
Materials and methods
Study design
This was a cohort study based on insurance registry data from the Swedish insurance company Folksam Insurance Group (Folksam). All data were handled confidentially in line with the Declaration of Helsinki. The study was approved by the Swedish Ethical Review Authority (reg. no 2022-00438-01). The study was reported according to the Strengthening the Reporting of Observational Studies in Epidemiology and the Sport Injury and Illness Surveillance extension [1, 25].
Population
The study population includes Swedish elite male and female athletes, covering a wide range of sports, within the Swedish Olympic Committee (SOC) support programme Top and Talent (Table 1). Inclusion criteria were all athletes that had participated in Top and Talent between January 1999 and December 2020. No exclusion criteria were applied. Top and Talent was initiated in 1998 and is an individually customised support programme for athletes with potential medal capacity in the Olympic Games, with a plan for the athlete to reach top international positions within 3–6 years of entering the programme. Athletes are accepted to the programme based on either top performance in international competitions or a talent selection [23]. Approximately 30% of the athletes in Top and Talent reach medal capacity in the Olympic Games or world championship after 4–6 years of entering the programme. Athletes in Top and Talent are provided with, among other things, medical, coaching, training, and nutritional support, and all athletes have health insurance from Folksam [23]. A total of 762 athletes (412 males, 350 females) in 38 sports participated in Top and Talent between 1999 and 2020 (Table 2). Mean ± SD age of the included athletes was 26.5 ± 5.9 years. On average, 172 ± 23 athletes (range 121–217) participated in the programme each year during the observation period. Duration of participation was median 4 years (IQR 2–6), with total of 3427 athlete-years included.
Data collection
Injury insurance claims were reported to the registry prospectively between 1999 and 2020 by a physician or physiotherapist from SOC via the athletes’ health insurance, after a median of 5 days (IQR 0–22) from date of injury. Only injuries occurring while the athletes participated in Top and Talent were registered. An administrator from Folksam was responsible for recording the injury in the registry. Injuries were diagnosed according to an insurance-specific coding system. The registry contained data about the insured athletes and about each injury. Details on the collected data are presented in Table 1. Injury data were extracted from the insurance registry in September 2022. Initial data processing and database construction was done by Folksam, and the data received for research and analysis were pseudonymised. The database was checked for errors by the first author, and any mismatching information (e.g. mismatched injury location and injury type) were checked against the original insurance claim record by Folksam, and corrected where possible.
Definition of injury
The health insurance covers both injuries and illnesses, but only injuries were included in this study. An eligible injury, as per the insurance policy, was defined as any physical damage with a sudden or gradual onset occurring while the athlete participated in Top and Talent. Pre-existing injuries present prior to start of the insurance were not included. Multiple injuries sustained by an athlete in a single event were recorded as one injury with multiple injury types or locations. Injury type was classified into eight different categories. Due to irregular reporting in the insurance registry, injuries reported as joint/ligament sprains, dislocations, and muscle/tendon strains and ruptures were combined by the authors to the same injury type category for descriptive statistics, named ‘soft tissue/joint injury’. The other injury type categories were contusion, fracture/bone injury, inflammation, concussion, laceration/abrasion, multiple injury types, and ‘unspecified’. Injuries were classified to a body region and location based on the reports made to the insurance registry.
Statistical analysis
Data were summarised using descriptive statistics, with mean, median, frequencies, standard deviations (SD), interquartile ranges (IQR) and/or 95% confidence intervals (CI), as appropriate. Incidence and characteristics (i.e. type and location) of injuries were presented for the total population and stratified for subgroups based on sex (male, female), competitive season (summer and winter sports), sport category (skill, power, mixed, endurance) [17], and age group (≤ 20, 21–25, 26–30, 31–35, 36–40, ≥ 41 years). Injury incidence and characteristics were presented only for individual sports with more than five athletes due to confidentiality reasons. Injury incidence was calculated as an incidence rate: number of injuries divided by number of athlete-years multiplied by 100 and expressed as number of injuries per 100 athlete-years. ‘Athlete-years’ was defined as the number of years an athlete participated in Top and Talent. If an athlete only participated half a year (spring or autumn) they were given a value of 0.5 years. All injuries (new and recurrent) and athlete-years were aggregated per athlete within each subgroup. This means that for age group specific injury numbers the same athlete can be included in multiple age groups depending on the athletes’ age at the exposure (athlete-year) and time of injury. Time trend analyses were performed for the 2001 to 2020 period with Poisson regression using generalized linear models with number of injuries as the dependent variable, year as covariate, and with natural log of the exposure variable (athlete-years) as offset variable. The model-based estimator was used for the covariance matrix and Wald statistics was used to calculate the p-value and 95% CI. The first 2 years (1999–2000) were excluded in the time trend analysis due to suspected low awareness about the health insurance when it first was released. Time trend analyses were performed for the full 20-years period for the total population and split by sex, as decided a priori. In addition, statistical time trend analyses were conducted post hoc for the first and second 10-years periods separately since ocular analysis indicated varying trends in the two decades. Time trends in injury incidence are expressed as the annual percent change between years with a 95% CI. The significance level was set at p < 0.05. All statistical analyses were performed using IBM SPSS Statistics (version 29.0, Armonk, New York, USA).
Results
Injury incidence
In total, 1635 injuries sustained by 468 athletes (61.4% of all athletes) were registered (median 2 injuries per athlete (IQR 1–5; range 1–21)). The overall incidence was 47.7 injuries/100 athlete-years, with 46.4 and 49.3 injuries/100 athlete-years among male and female athletes, respectively. The highest incidence per individual sport was seen in gymnastics, tennis, and athletics (100.0, 99.3, and 93.4 injuries/100 athlete-years, respectively). Injury incidence in the total population and for subgroups is presented in Tables 3 and 4, and Online Resource 1, and incidence by injury type and location is presented in Table 5.
Time trends in injury incidence
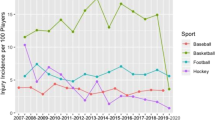
The time trend analysis showed that the overall injury incidence increased by 3.0% annually over the full 20-years period between 2001 and 2020 (95% CI 2.1–3.9%, p < 0.001). Males had an 2.5% annual increased incidence (95% CI 1.4–3.7%, p < 0.001) and females an 3.7% increase (95% CI 2.3–5.1%, p < 0.001). Noteworthy was that the injury incidence increase was evident only in the first 10-years period of 2001–2010 (annual change 6.0%, 95% CI 3.3–8.8%, p < 0.001), while the second 10-year period of 2011–2020 showed no such trend (annual change 0.4%, 95% CI − 1.9 to 2.7%, (n.s.)) Year-by-year injury incidences for subgroups (sex, competitive season, sport category, and age group) are presented in Fig. 1.

Time trend in injury incidence by sex (a), competitive season (b), sport category (c) and age group (d). Symbol next to the year illustrates whether the summer (sun symbol) or winter (snowflake symbol) Olympic Games was held in the current year. Due to small sample size in the age groups 31–35, 36–40 and ≥ 41 years, these age groups were combined to one group ≥ 31 years for visual presentation in graph. Data on age is missing for 14 athletes
Injury characteristics
The lower limb region, and specifically the knee, had the highest injury frequency, and soft tissue/joint injury was the most common injury type category among the specified injury types. Injury characteristics are presented in Tables 4 and 5, and Online Resource 2 and 3.
Discussion
The principal findings of the study were that the overall injury incidence among Swedish Olympic athletes increased by six percent annually between 2001 and 2010, after which the curve flattened with no change between 2011 and 2020. Athletes report approximately one injury to the insurance registry every second year, where most injuries affect the knee, foot/ankle, and spine/pelvis. There is a paucity of research on the year-round injury incidence and characteristics among Olympic athletes and the present study is, to the best of our knowledge, the first to describe injuries over a two-decade long period using insurance data.
Injury incidence and characteristics in the total population
The injury incidence was 47.7 injuries/100 athlete-years. Compared to previous studies in Olympic athletes, this incidence rate is low. During the Olympic Games of 2014 to 2020, the injury incidence was between 5.4 and 7.8 injuries/1000 athlete-days (equal to 197.1–284.7 injuries/100 athlete-years) [19,20,21,22], and among UK Olympic summer sport athletes, an injury incidence of 1.32 injuries/athlete-year (equal to 132.0 injuries/100 athlete-years) has been reported [18]. This discrepancy may be explained by differences in data collection methods (e.g. prospective study with athlete self-report versus medical record or insurance-based registry) and injury definitions (e.g. all injuries irrespective of time-loss or medical attention versus medical attention or insurance claims), and the fact that the insurance registry used in the present study likely captures primarily more severe injuries (i.e. ‘tip of the iceberg’). The true injury incidence in this study population is probably higher, and a direct comparison to previous studies is difficult. Overall, the lower limb was the most injured body region, and the knee, followed by foot/ankle, and spine/pelvis the most injured locations, which is in line with previous studies in Olympic athletes [18,19,20].
Injury incidence and characteristics in subgroups
Injury incidence was highest among power and mixed sports, possibly due to the nature and demands of these sports, which often involve high forces and athlete-to-athlete contacts. It should be noted, however, that there was a variation in injury incidence among single sports within the four sport categories. For instance, in mixed sports, the injury incidence ranged between 16.3 and 99.3 injuries/100 athlete-years, and among power sports between 45.0 and 100.0 injuries/100 athlete-years. All sports that had a higher injury incidence than the total population average belonged to the mixed or power sport categories. Previously, Ranson et al. reported that the injury incidence was highest in combat sports [18], and combat sports were included in the mixed or power sport category in the present study. Injuries to the knee and foot/ankle were prevalent among athletes in the power and mixed sport categories, indicating that these locations should be specifically targeted with injury prevention measures. In many skill and endurance sports, in addition to the knee, injuries were also frequent in the spine/pelvis and shoulder, indicating a need for other preventive measures in these types of sports.
In the present study the overall injury incidence was comparable between males and females, which is in line with previous reports during the Olympic Games [19,20,21,22]. In team sports, however, the overall injury incidence is higher among males [28], and this difference may be due to the fact that the present study mainly included individual sports. While certain knee injuries, such as anterior cruciate ligament injuries, are more common in female than in male team sport athletes [28], overall knee injuries were equally common in males and females in the present study (detailed diagnoses were not available for all knee injuries).
Comparing age groups, the highest overall injury incidence was seen among athletes ≤ 20 years, with a trend that the injury incidence decreases with higher age. This age–injury relationship was evident in the mixed and skill sport categories, but not in power and endurance sports. It should be noted, however, that comparison within single sports were not possible due to small samples, and large variations may exist. Further, there were differences in the number of athlete-years in different sports within the sport categories and age groups (Online Resource 4), and the reason for the observed age-injury relationship is unclear.
The observed variation in injury incidence and characteristics between sports and subgroups emphasises the importance of considering the contextual factors—such as environmental factors and sport and athlete characteristics—when implementing injury prevention interventions [3].
Time trends
A significant time trend was noted with a three percent annual increase in injury incidence over the full 20-years period, which was evident in both males and females. However, when analysing time trends for the first and second 10-years periods separately, the increasing trend was evident only during the first decade of 2001 to 2010, after which the injury incidence remained fairly stable between 2011 and 2020. This indicates that there is currently no trend of increasing injury incidence in the Swedish Top and Talent athlete population. Looking at the time trends year-by-year, some variations could be seen within subgroups. For example, in winter sports, there was a tendency towards a high injury incidence the year prior to each Winter Olympic Games, and low incidence the year of the Olympic Games. While not as obvious, this tendency was also seen in summer sports in relation to the Summer Olympic Games. Based on the data it is not possible to explain the observed increasing time trend or year-by-year fluctuations in injury incidence with any certainty. It may be the result of sporting factors; e.g. changes in sporting/physical demands, competition and training schedules, or rules or equipment, but also due to methodological factors such as varying population characteristics or reporting patterns.
Strengths and limitations
Strengths of the study include the long time period of data collection, and a large sample of athletes who had participated in Top and Talent between 1999 and 2020. In contrast to most previous research of injuries in Olympic athletes [19,20,21,22], but similar to Ranson et al. [18] and Clarsen et al. [4], the present study included also injuries sustained outside the Olympic game period, taking into consideration seasonal differences in injury rates and better reflecting the full athlete year cycle. Furthermore, the same inclusion criteria to Top and Talent were used over the 22 years, and the injury definition remained consistent over the years, allowing for comparable data over time. Another strength is the inclusion of sport-specific injury data, also providing data on injuries in sports with very little, or non-existent, previous research. To allow for meaningful comparison between groups with sufficient samples, sports and athletes were classified into subgroups. A limitation of this approach is that sports and athletes within the same subgroup may differ, and certain sports or athletes may be responsible for the majority of injury cases within the group, thus skewing the data. For example, within the mixed sport category in the present study, athletics was responsible for approximately 59% of injuries. Also, some sports, such as athletics, consist of different disciplines with varying injury burdens and patterns.
Another limitation is that many injuries were registered in the insurance registry as unspecified for injury type. Information about these injuries is therefore limited, and it is possible that the proportion of injuries in specific injury types would be different if all injuries had more specified information. More specific injury registration is important to increase the quality of the registry and to allow more definitive conclusions about injury rates and patterns.
Registry data from 1999, shortly after the inception of Top and Talent in 1998, was included. Due to low awareness of the health insurance in the initial years and likely some missing injury data, this results in underestimation of the injury incidence in these years, and to a smaller extent also the overall injury incidence. It is likely that insurance registry data includes primarily more severe injuries. Minor injuries—for example certain gradual onset injuries, or injuries not resulting in time-loss or affecting athlete performance—may go unreported to the insurance company. Given the insurance registry-based data collection, the generalisability of the findings to other populations and surveillance methods is unclear. Gradual onset injuries and non-time loss injuries dominate the injury pattern in Olympic sports [4, 19, 20], and gathering information about these injuries in a structured and systematic manner is important to get a complete understanding of injuries in Olympic athletes.
Conclusions
The overall injury incidence increased by six percent annually between 2001 and 2010, after which the curve flattened with no change between 2011 and 2020. Swedish Olympic athletes report approximately one injury to the insurance registry every second year, where most injuries affect the knee, foot/ankle, and spine/pelvis. The highest injury incidence was seen in gymnastics, tennis, and athletics, and for specific subgroups, in mixed and power sports and younger age groups. Injury prevention interventions should be a high priority in these sports and subgroups. The findings may support health and performance teams working with Olympic athletes in their work to improve athlete health, by highlighting incidence rates and common injury locations in different subgroups and sports.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- CI:
-
Confidence interval
- Folksam:
-
Folksam Insurance Group
- IQR:
-
Interquartile range
- SD:
-
Standard deviation
- SOC:
-
Swedish Olympic Committee
References
Bahr R, Clarsen B, Derman W, Dvorak J, Emery CA, Finch CF et al (2020) International Olympic Committee consensus statement: methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br J Sports Med 54:372–389
Beaudouin F, Aus der Fünten K, Tröß T, Reinsberger C, Meyer T (2019) Head injuries in professional male football (soccer) over 13 years: 29% lower incidence rates after a rule change (red card). Br J Sports Med 53:948–952
Bolling C, van Mechelen W, Pasman HR, Verhagen E (2018) Context matters: revisiting the first step of the ‘sequence of prevention’ of sports injuries. Sports Med 48:2227–2234
Clarsen B, Steffen K, Berge HM, Bendiksen F, Fossan B, Fredriksen H et al (2021) Methods, challenges and benefits of a health monitoring programme for Norwegian Olympic and Paralympic athletes: the road from London 2012 to Tokyo 2020. Br J Sports Med 55:1342–1349
Drew MK, Raysmith BP, Charlton PC (2017) Injuries impair the chance of successful performance by sportspeople: a systematic review. Br J Sports Med 51:1209–1214
Edouard P, Navarro L, Pruvost J, Branco P, Junge A (2021) In-competition injuries and performance success in combined events during major international athletics championships. J Sci Med Sport 24:152–158
Ekegren CL, Gabbe BJ, Finch CF (2016) Sports injury surveillance systems: a review of methods and data quality. Sports Med 46:49–65
Ekstrand J, Spreco A, Bengtsson H, Bahr R (2021) Injury rates decreased in men’s professional football: an 18-year prospective cohort study of almost 12 000 injuries sustained during 1.8 million hours of play. Br J Sports Med 55:1084–1091
Engebretsen L, Soligard T, Steffen K, Alonso JM, Aubry M, Budgett R et al (2013) Sports injuries and illnesses during the London Summer Olympic Games 2012. Br J Sports Med 47:407–414
Engebretsen L, Steffen K, Alonso JM, Aubry M, Dvorak J, Junge A et al (2010) Sports injuries and illnesses during the Winter Olympic Games 2010. Br J Sports Med 44:772–780
Feddermann-Demont N, Junge A, Edouard P, Branco P, Alonso J-M (2014) Injuries in 13 international Athletics championships between 2007–2012. Br J Sports Med 48:513–522
Hägglund M, Waldén M, Magnusson H, Kristenson K, Bengtsson H, Ekstrand J (2013) Injuries affect team performance negatively in professional football: an 11-year follow-up of the UEFA Champions League injury study. Br J Sports Med 47:738–742
Joseph C, Naughton G, Antcliff A (2019) Australian netball injuries in 2016: an overview of insurance data. J Sci Med Sport 22:1304–1308
Junge A, Dvorak J (2013) Injury surveillance in the World Football Tournaments 1998–2012. Br J Sports Med 47:782–788
Junge A, Engebretsen L, Mountjoy ML, Alonso JM, Renström PA, Aubry MJ et al (2009) Sports injuries during the Summer Olympic Games 2008. Am J Sports Med 37:2165–2172
King D, Hume PA, Hardaker N, Cummins C, Gissane C, Clark T (2019) Sports-related injuries in New Zealand: National Insurance (Accident Compensation Corporation) claims for five sporting codes from 2012 to 2016. Br J Sports Med 53:1026–1033
Niebauer J, Borjesson M, Carre F, Caselli S, Palatini P, Quattrini F et al (2018) Recommendations for participation in competitive sports of athletes with arterial hypertension: a position statement from the sports cardiology section of the European Association of Preventive Cardiology (EAPC). Eur Heart J 39:3664–3671
Ranson C, Wootten M, Biswas A, Herrington L, Gallimore D, Jackson PD et al (2023) Year-round longitudinal health surveillance in UK Olympic Summer Sport Athletes 2016–2019. Br J Sports Med. https://doi.org/10.1136/bjsports-2022-105992
Soligard T, Palmer D, Steffen K, Lopes AD, Grant ME, Kim D et al (2019) Sports injury and illness incidence in the PyeongChang 2018 Olympic Winter Games: a prospective study of 2914 athletes from 92 countries. Br J Sports Med 53:1085–1092
Soligard T, Palmer D, Steffen K, Lopes AD, Grek N, Onishi K et al (2022) New sports, COVID-19 and the heat: sports injuries and illnesses in the Tokyo 2020 Summer Olympics. Br J Sports Med 57:46–54
Soligard T, Steffen K, Palmer-Green D, Aubry M, Grant ME, Meeuwisse W et al (2015) Sports injuries and illnesses in the Sochi 2014 Olympic Winter Games. Br J Sports Med 49:441–447
Soligard T, Steffen K, Palmer D, Alonso JM, Bahr R, Lopes AD et al (2017) Sports injury and illness incidence in the Rio de Janeiro 2016 Olympic Summer Games: a prospective study of 11274 athletes from 207 countries. Br J Sports Med 51:1265–1271
Sveriges Olympiska Kommitté. Topp och Talang. https://sok.se/idrottsstod---topp-och-talang/topp-och-talang.html. Accessed 30 May 2023
van Mechelen W, Hlobil H, Kemper HC (1992) Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med 14:82–99
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP (2007) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370:1453–1457
von Rosen P, Heijne A (2018) Substantial injuries influence ranking position in young elite athletes of athletics, cross-country skiing and orienteering. Scand J Med Sci Sports 28:1435–1442
West SW, Starling L, Kemp S, Williams S, Cross M, Taylor A et al (2021) Trends in match injury risk in professional male rugby union: a 16-season review of 10 851 match injuries in the English Premiership (2002–2019): the Professional Rugby Injury Surveillance Project. Br J Sports Med 55:676–682
Zech A, Hollander K, Junge A, Steib S, Groll A, Heiner J et al (2022) Sex differences in injury rates in team-sport athletes: a systematic review and meta-regression analysis. J Sport Health Sci 11:104–114
Åman M, Forssblad M, Henriksson-Larsén K (2016) Incidence and severity of reported acute sports injuries in 35 sports using insurance registry data. Scand J Med Sci Sports 26:451–462
Åman M, Forssblad M, Henriksson-Larsén K (2014) Insurance claims data: a possible solution for a national sports injury surveillance system? An evaluation of data information against ASIDD and consensus statements on sports injury surveillance. BMJ Open 4:e005056
Acknowledgements
We would like to thank Henrik Hedevik, statistician, for support with the database construction and analyses.
Funding
Open access funding provided by Linköping University. The research was partially funded by the Swedish Olympic Committee.
Author information
Authors and Affiliations
Contributions
MH and KT planned and designed the study. KT and MH analysed the data. KT drafted the manuscript that was read and critically revised by MH, HL, SS, EHS, HS, LT, and JS. All authors read and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
Folksam Insurance Group and the Swedish Olympic Committee were involved in providing data for the study. HS is employed by Folksam Insurance Group, and LT and JS are employed by the Swedish Olympic Committee. Neither organisation had any influence over analysis or presentation of results. All authors declare no conflict of interest.
Ethical approval
The study was approved by the Swedish Ethical Review Authority (reg. no 2022 00438 01).
Informed consent
This registry-based study using only pseudonymized data were conducted without written consent from participants, as authorized by the Swedish Ethical Review Authority.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Torvaldsson, K., Lindblom, H., Sonesson, S. et al. Swedish Olympic athletes report one injury insurance claim every second year: a 22-year insurance registry-based cohort study. Knee Surg Sports Traumatol Arthrosc 31, 4607–4617 (2023). https://doi.org/10.1007/s00167-023-07511-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-023-07511-y