
Abstract
Purpose
To compare the effect of ‘intermittent’ central venous oxygen saturation (ScvO2) monitoring with ‘continuous’ ScvO2 monitoring on shock resolution and mortality in children with septic shock.
Methods
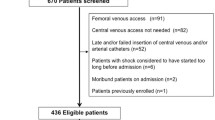
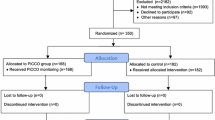
Primary outcome was the achievement of therapeutic goals or shock resolution in the first 6 h. We randomly assigned children < 17 years’ age with septic shock to ‘intermittent ScvO2’ or ‘continuous ScvO2’ groups. All children were subjected to subclavian/internal jugular line insertion and managed as per Surviving Sepsis Campaign Guidelines. To guide resuscitation, we used ScvO2 estimated at other clinical and laboratory parameters were monitored similarly in both groups.
Results
We enrolled 75 and 77 children [median (IQR) age: 6 (1.5–10) years] in the ‘intermittent’ and ‘continuous’ groups, respectively. Baseline characteristics were comparable between the groups. When compared to the ‘continuous’ group, fewer children in the ‘intermittent’ group achieved shock resolution within first 6 h [19% vs. 36%; relative risk (RR) 0.51; 95% CI 0.29–0.89; risk difference − 18.0%; 95% CI − 32.0 to − 4.0]. The lower bound of confidence interval, however, crossed the pre-specified non-inferiority margin. There was no difference in the proportion of children attaining shock resolution within 24 h (63% vs. 69%; RR 0.86; 95% CI 0.68–1.08) or risk of mortality between the groups (47% vs. 43%; RR 1.06; 95% CI 0.74–1.51).
Conclusions
Given that a greater proportion of children attained therapeutic end points in the first 6 h, continuous monitoring of ScvO2 should preferably be used to titrate therapy in the first few hours in children with septic shock. In the absence of such facility, intermittent monitoring of ScvO2 can be used to titrate therapy in these children, given the lack of difference in the proportion of patients achieving shock resolution at 24 h or in risk of mortality between the intermittent and continuous groups.


Similar content being viewed by others

References
Jaramillo-Bustamante JC, Marín-Agudelo A, Fernández-Laverde M, Bareño-Silva J (2012) Epidemiology of sepsis in pediatric intensive care units: first Colombian multicenter study. Pediatr Crit Care Med 13:501–508
Sankar J, Dhochak N, Kumar K, Singh M, Sankar MJ, Lodha R (2019) Comparison of international pediatric sepsis consensus conference versus sepsis-3 definitions for children presenting with septic shock to a tertiary care center in India: a retrospective study. Pediatr Crit Care Med 20:e122–e129
Hartman ME, Linde-Zwirble WT, Angus DC, Watson RS (2013) Trends in the epidemiology of pediatric severe sepsis. Pediatr Crit Care Med 14:686–693
Weiss SL, Fitzgerald JC, Pappachan J et al (2017) Australian and New Zealand Intensive Care Society (ANZICS) Centre for Outcomes and Resource Evaluation (CORE) and Australian and New Zealand Intensive Care Society (ANZICS) Paediatric Study Group. Prediction of pediatric sepsis mortality within 1 h of intensive care admission. Prediction of pediatric sepsis mortality within 1 h of intensive care admission. Intensiv Care Med 43:1085–1096
Wiens MO, Larson CP, Kumbakumba E et al (2016) Application of Sepsis definitions to pediatric patients admitted with suspected infections in uganda. Pediatr Crit Care Med 17:400–405
Rivers E, Nguyen B, Havstad S et al (2001) Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 345:1368–1377
Focht A, Jones AE, Lowe TJ (2009) Early goal-directed therapy: improving mortality and morbidity of sepsis in the emergency department. Jt Comm J Qual Patient Saf 35:186–191
Chelkeba L, Ahmadi A, Abdollahi M, Najafi A, Mojtahedzadeh M (2015) Early goal-directed therapy reduces mortality in adult patients with severe sepsis and septic shock: systematic review and meta-analysis. Indian J Crit Care Med 19:401–411
Davis AL, Carcillo JA, Aneja RK et al (2017) American College of Critical Care Medicine clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock. Crit Care Med 45:1061–1093
Liu B, Ding X, Yang J (2016) Effect of early goal directed therapy in the treatment of severe sepsis and/or septic shock. Curr Med Res Opin 32:1773–1782
ARISE Investigators; ANZICS Clinical Trials Group (2014) Goal-directed resuscitation for patients with early septic shock. N Engl J Med 371:1496–1506
Investigators ProCESS, Yealy DM, Kellum JA, Huang DT et al (2014) A randomized trial of protocol-based care for early septic shock. N Engl J Med 370:1683–1693
Mouncey PR, Osborn TM, Power GS, ProMISe Trial Investigators et al (2015) Trial of early, goal-directed resuscitation for septic shock. N Engl J Med 372:1301–1311
de Oliveira CF, de Oliveira DS, Gottschald AF et al (2008) ACCM/PALS haemodynamic support guidelines for paediatric septic shock: an outcomes comparison with and without monitoring central venous oxygen saturation. Intensiv Care Med 34:1065–1075
Sankar J, Sankar MJ, Suresh CP, Sankar MJ, Dubey N (2014) Early goal-directed therapy in pediatric septic shock: comparison of outcomes “with” and “without” intermittent superior venacaval oxygen saturation monitoring: a prospective cohort study. Pediatr Crit Care Med 15:e157–e167
Gross PA (2006) Hypotension and mortality in septic shock: the “golden hour”. Crit Care Med 34:1819–1820
Han YY, Carcillo JA, Dragotta MA, Bills DM, Watson RS, Westerman ME, Orr RA (2003) Early reversal of pediatric-neonatal septic shock by community physicians is associated with improved outcome. Pediatrics 112:793–799
Huh JW, Oh BJ, Lim CM, Hong SB, Koh Y (2013) Comparison of clinical outcomes between intermittent and continuous monitoring of central venous oxygen saturation (ScvO2) in patients with severe sepsis and septic shock: a pilot study. Emerg Med J 30:906–909
Paula IRN, Timothy WS, Steven QS (2009) Effect of intermittent vs continuous scvo2 monitoring on sepsis bundle compliance and mortality. October 2009, Vol 136, No. 4 MeetingAbstracts
Goldstein B, Giroir B, Randolph A (2005) International Consensus Conference on Pediatric Sepsis. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med J Soc Crit Care Med World Fed Pediatr Intensiv Crit Care Soc 6: 2–8
Haque IU, Zaritsky AL (2007) Analysis of the evidence for the lower limit of systolic and mean arterial pressure in children. Pediatr Crit Care Med 8:138–144
Dellinger RP, Levy MM, Rhodes A et al (2012) Surviving Sepsis Campaign Guidelines Committee including The Pediatric Subgroup. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensiv Care Med 39:165–228
Carcillo JA, Fields A (2002) Clinical practice parameters for hemodynamic support of pediatric and neonatal patients in septic shock. J Pediatr (Rio J) 78:449–466
Pediatric Advanced Life Support Provider Manual, Chameides L, Samson RA, Schexnayder SM, Hazinski MF (Eds) (2012) American Heart Association, Dallas
Perner A, Haase N, Wiis J, White JO, Delaney A (2010) Central venous oxygen saturation for the diagnosis of low cardiac output in septic shock patients. Acta Anaesthesiol Scand 54:98–102
Walley KR (2011) Use of central venous oxygen saturation to guide therapy. Am J Respir Crit Care Med 184:514–520
Ding XF, Yang ZY, Xu ZT et al (2018) Early goal-directed and lactate-guided therapy in adult patients with severe sepsis and septic shock: a meta-analysis of randomized controlled trials. J Transl Med 16:331
Acknowledgements
We would like to sincerely thank the contributions of Dr Vijay and the staff of the PICU towards the conduct of the trial.
Funding
The authors received Intramural Research Grant (No.F. 8-335/A-335/2-15/RS) from All India Institute of Medical Sciences for this project (~ 7000 USD).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Sankar, J., Singh, M., Kumar, K. et al. ‘Intermittent’ versus ‘continuous’ ScvO2 monitoring in children with septic shock: a randomised, non-inferiority trial. Intensive Care Med 46, 82–92 (2020). https://doi.org/10.1007/s00134-019-05858-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-019-05858-w