
Abstract
Aims/hypothesis
Validated biomarkers are needed to monitor the effects of immune intervention in individuals with type 1 diabetes. Despite their importance, few options exist for monitoring antigen-specific T cells. Previous reports described a combinatorial approach that enables the simultaneous detection and quantification of multiple islet-specific CD8+ T cell populations. Here, we set out to evaluate the performance of a combinatorial HLA-A2 multimer assay in a multi-centre setting.
Methods
The combinatorial HLA-A2 multimer assay was applied in five participating centres using centralised reagents and blinded replicate samples. In preliminary experiments, samples from healthy donors were analysed using recall antigen multimers. In subsequent experiments, samples from healthy donors and individuals with type 1 diabetes were analysed using beta cell antigen and recall antigen multimers.
Results
The combinatorial assay was successfully implemented in each participating centre, with CVs between replicate samples that indicated good reproducibility for viral epitopes (mean %CV = 33.8). For beta cell epitopes, the assay was very effective in a single-centre setting (mean %CV = 18.4), but showed sixfold greater variability across multi-centre replicates (mean %CV = 119). In general, beta cell antigen-specific CD8+ T cells were detected more commonly in individuals with type 1 diabetes than in healthy donors. Furthermore, CD8+ T cells recognising HLA-A2-restricted insulin and glutamate decarboxylase epitopes were found to occur at higher frequencies in individuals with type 1 diabetes than in healthy donors.
Conclusions/interpretation
Our results suggest that, although combinatorial multimer assays are challenging, they can be implemented in multiple laboratories, providing relevant T cell frequency measurements. Assay reproducibility was notably higher in the single-centre setting, suggesting that biomarker analysis of clinical trial samples would be most successful when assays are performed in a single laboratory. Technical improvements, including further standardisation of cytometry platforms, will likely be necessary to reduce assay variability in the multi-centre setting.
Similar content being viewed by others


Introduction
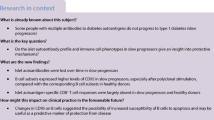
Effective biomarkers are needed to monitor autoimmune progression in individuals at risk of developing type 1 diabetes mellitus and to monitor interventions in those with established disease [1]. This need is particularly compelling in light of the increasing number of clinical trials designed to test the efficacy of therapies to halt autoimmune destruction of pancreatic beta cells [2]. However, there is a dearth of reproducible assays that can be applied to frozen peripheral blood mononuclear cells (PBMCs). For successful trials, surrogate biomarkers may enable the identification of immune profiles associated with favourable outcomes, allowing stratification of subgroups based on predicted response to therapy. Immune biomarkers are equally important for mechanistic explorations in the context of trials that failed to achieve significant clinical outcomes. Such biomarkers may help to differentiate between lack of biological effect and immune modifications that did not translate into clinical benefit, thereby informing the design of subsequent trials [3].
Assays that measure the frequencies of beta cell-reactive CD8+ T cells provide attractive options for the detection of candidate biomarkers. Such autoreactive CD8+ T cells have been identified in pancreatic biopsies from people with newly diagnosed and long-term diabetes [4]. Furthermore, CD8+ T cells are the most abundant lymphocyte population in insulitic lesions [5] and occur in the pancreatic transplants of recipients with recurrent autoimmune disease [6]. Preproinsulin (PPI)-reactive CD8+ T cells have also been shown to kill beta cells in vitro [7]. In addition, non-obese diabetic mice lacking expression of MHC class I molecules are resistant to diabetes [8], whereas adoptive transfer of CD8+ T cells causes disease in recipient mice [9,10,11]. These observations suggest a pathogenic role for CD8+ T cells in the autoimmune process, consistent with the identification of multiple HLA class I alleles as risk variants for the development of diabetes [12, 13].
Although other assay formats are available, HLA class I multimer staining is an attractive option that allows direct ex vivo detection of autoreactive CD8+ T cells using relatively small numbers of PBMCs [14]. Previous studies have validated this method and demonstrated clear visualisation of CD8+ T cells specific for recall antigens [15]. In contrast, self-antigen-specific CD8+ T cells typically display lower avidities and tend to stain less distinctly with HLA class I multimers [16]. Combinatorial staining solves these problems by assigning a pair of fluorochromes to each epitope specificity [17]. Such dual staining more readily separates background from multimer-specific signals, allowing efficient interrogation of multiple specificities within a single assay tube. Consequently, this approach has been advanced to monitor immune responses in various settings [17, 18] and further extended on a mass cytometry platform to interrogate a vast number of specificities [19].
Using this strategy, autoreactive CD8+ T cells have been detected in frozen samples from individuals with type 1 diabetes, first-degree relatives, healthy donors and islet cell-transplant recipients [1]. However, it remains unclear whether this assay can be implemented reliably across different laboratories. We therefore sought to test the potential utility of combinatorial HLA class I multimer staining by assessing reproducibility in a single centre vs multiple centres. To aid visualisation, we modified the staining protocol to include the tyrosine kinase inhibitor dasatinib, which helps stabilise T cell receptor expression to maximise the uptake of HLA class I multimers [20].
Methods
Human samples
Three sets of frozen HLA-A*02:01+ (designated HLA-A2+ hereafter) samples were obtained with informed consent within approved studies coordinated by the Benaroya Research Institute (BRI). Sample set 1 consisted of replicate vials of 5 × 106 PBMCs from five healthy donors obtained through the BRI Control Repository. Sample set 2 consisted of replicate vials of 10 × 106 PBMCs from five individuals with type 1 diabetes (mean age 25 ± 5.6 years; 40% female; disease duration 1.7 to 6.6 years; all insulin treated) obtained through the BRI Diabetes Repository. Sample set 3 consisted of replicate vials of 10 × 106 PBMCs from ten healthy donors (mean age 36 ± 12 years; 60% female; all screened to exclude autoantibody-positive individuals and first-degree relatives of autoimmune individuals) obtained through the BRI and nine individuals with type 1 diabetes (mean age 30 ± 9.6 years; 33% female; disease duration <5 years; all insulin treated) obtained through the BRI Diabetes Repository, together with a spiked sample prepared by mixing a cytomegalovirus (CMV)-specific T cell clone (2F3) and a PPI-specific T cell clone (2D5; both clones obtained from King’s College London, London, UK) with PBMCs from an HLA-A2− donor at frequencies of approximately 0.55% and 0.38%, respectively. All sample vials were transferred between centres using a liquid nitrogen dry shipper. Characteristics of the individuals who provided samples are summarised in ESM Tables 1, 2 and 3.
Peptides and HLA class I multimers
Peptides representing immunodominant beta cell and recall epitopes (Table 1) were synthesised by Genscript (Piscataway, NJ, USA). HLA-A2 monomers were obtained through the National Institutes of Health (NIH) Tetramer Core Facility (Atlanta, GA, USA) and distributed to participating centres together with Qdot-labelled streptavidins and antibodies. Qdot multimers were prepared essentially as described previously [14]. Briefly, 20 μl of each monomer (0.1 μg/μl) in PBS was multimerised by adding 2.2 μl of the appropriate Qdot-labelled streptavidin (Thermo Fisher Scientific, Waltham, MA, USA) for 30 min at 4°C. d-biotin (final concentration 25 μmol/l; Avidity, Aurora, CO, USA) was subsequently added for 20 min at 4°C, followed by 1 μl of 12.5% (wt/vol.) BSA/PBS solution. Multimers were stored at 4°C and used within 2 weeks.
Thawing and viability assessment of PBMC samples
PBMCs were handled according to Immunology of Diabetes Society T Cell Workshop recommendations [21, 22]. Briefly, heparinised blood was fractionated by Ficoll underlay, and PBMCs were frozen gradually at a concentration of 1 × 107/ml in fetal bovine serum supplemented with 10% dimethyl sulfoxide. After storage and shipment, cryovials were transferred to a 37°C water bath, agitated until the cells were just thawed, and topped up with 1 ml medium (Iscove’s Modified Dulbecco’s Medium or RPMI + 50% [vol./vol.] fetal calf serum). Cells were then transferred to a 15 ml sterile tube prefilled with 1 ml medium, washed, pelleted, rested for 15 min, assessed for viability using Trypan Blue and re-suspended after a final wash at 20 × 106 cells/ml in PBA buffer (PBS + 0.5% [wt/vol.] BSA + 0.01% [wt/vol.] sodium azide). Samples with viability and recovery counts >50% were considered acceptable and used for multimer staining.
Combinatorial multimer staining
Combinatorial staining was performed on all recovered cells essentially as described previously [14]. In addition, cells were treated for 15 min at 37°C with 50 nmol/l dasatinib prior to assay. Batches of five samples were processed in parallel. For each batch, a Qdot master mix was prepared by combining 5 μl of each Qdot-labelled multimer (summarised in Table 1) with 200 μl PBA. Each sample was pelleted, re-suspended in 57 μl Qdot master mix and incubated for 15 min at 37°C. Cells were then stained for 30 min at 4°C with: 1.5 μl anti-CD8 allophycocyanin (BD Biosciences, San Jose, CA, USA), 2.5 μl each of anti-CD4/CD14/CD16/CD20/CD40-FITC (dump channel; eBioscience, Waltham, MA, USA), and 3 μl 7-aminoactinomycin D (7-AAD). Single-colour compensation controls were generated using cells disrupted with 1% Tween 20 (for the 7-AAD control) and BD CompBeads coated either with one of the directly conjugated antibodies or with a biotin-conjugated anti-CD8 antibody followed by one of the relevant streptavidins. After staining, cells were washed and acquired by flow cytometry, with the equipment configurations detailed in ESM Table 4. Each cytometer was optimised daily using CS&T research beads (BD Biosciences). Data were analysed centrally (in a sample-blinded fashion) in Seattle using a Boolean gating strategy [14] (summarised in ESM Fig. 1) to enumerate viable dump-negative CD8+ singlets that were uniquely positive for each pair of Qdot labels. A 0.05% cut-off for positive responses was chosen based on the level of staining observed for the non-interfacing control multimer (mean ±3 SDs). Each centre also analysed their own data in a blinded fashion, setting thresholds for positive staining using their own specific cut-offs, again with reference to the non-interfacing multimer together with qualitative criteria such as the distribution pattern of staining (i.e. clustering vs spread). In both analyses, blind calls were made by classifying an individual with positive staining for at least one beta cell antigen multimer as an individual with type 1 diabetes, and an individual without positive staining for beta cell antigen multimers as a healthy donor.
Statistical methods
Systematic variations between centres were evaluated using one-way ANOVA (with centres as columns and matched observations in each row). Where p values were <0.05, column means were compared using Tukey’s multiple comparisons test. Agreement between replicate samples (assayed either in a single centre or between centres) was assessed using %CV, calculated as the ratio of the SD and mean × 100. Aggregated multimer data were arranged as a contingency table, and the association of positive responses in samples from individuals with type 1 diabetes vs healthy donors was evaluated using the Fisher exact test. Contingency analysis was performed using the VassarStats online contingency table resource (http://vassarstats.net/newcs.html). All other statistical analyses were carried out using Prism version 6.01 (GraphPad Software, La Jolla, CA, USA).
Results
Viability and cell recovery for shipped PBMC samples
Replicate cryovials from healthy donors (sample set 1) for analysis with recall antigen multimers (ESM Table 1) and replicate cryovials from healthy donors and individuals with type 1 diabetes (sample set 3) for analysis with beta cell and recall antigen multimers (ESM Table 3) were thawed at each participating centre and assessed for viability (Fig. 1). For sample set 1, no differences in recovery were observed among centres (median 64.0%; range 52.5–65.6%), and differences in viability were modest (median 91.5%; range 86.4–95.0%), potentially reflecting a systematic counting bias across centres. For sample set 3, significantly lower viability and recovery rates were obtained in Denver, possibly because the samples were stored for longer before analysis. Despite these differences, each vial provided sufficient material for analysis.

PBMC viability and recovery at each centre. (a) Post-thaw viability of sample set 1 at each centre, as measured by live/dead counting. Each symbol (circle, square, triangle, inverted triangle, diamond and hexagon) indicates a unique sample. The short horizontal lines show the mean values. Sample viability was significantly lower in Leiden than in Cardiff and Denver. (b) Post-thaw recovery of sample set 1 at each centre, estimated by comparing the live count with the total number of frozen cells. Symbols are identical to part (a). No significant differences were observed. (c) Post-thaw viability of sample set 2 at each centre. Each symbol indicates a unique sample. Sample viability was significantly lower in Denver than in other centres. (d) Post-thaw recovery of sample set 2 at each centre. Symbols are identical to part (c). Sample recovery was significantly lower in Denver than in other centres. **p < 0.01 and ***p < 0.001
Reproducibility of multimer analysis of recall antigen-reactive CD8+ T cells
To implement the combinatorial assay in each centre, five samples from HLA-A2+ healthy donors (sample set 1) were distributed as identical replicate vials and assessed qualitatively and quantitatively for responses to CMV, Epstein–Barr virus (EBV) and influenza epitopes. All samples were pre-treated with dasatinib and stained using multimer panel 1 (listed in Table 1). Representative data are shown in Fig. 2a. Although some numerical differences were observed (Fig. 2b), the staining results were statistically equivalent among centres for all three viral epitopes, with acceptable %CVs (mean 33.8; SD 12.5) for specificities above the positive threshold of 0.05%. The panel was designed to include five different Qdots (585, 605, 655, 705 and 800) to verify that each centre was able to detect signals in each channel despite the use of different cytometer configurations (ESM Table 4). This sample set also included an HLA-A2− control sample, for which the numbers of positive events detected with recall antigen multimers were consistently lower than or equivalent to those detected with the non-interfacing control multimer in all channels.

Multimer analysis for recall antigens. (a) Dot plots show representative data for sample 1 of sample set 1, stained in Leiden using the CMV, non-interfacing (Neg), EBV and influenza M1 (Flu) multimers. Each subpart depicts staining of live CD8+ T cells by the Qdot pair of interest after combinatorial gating. For this sample, positive double staining was virtually absent for the CMV and control multimers, but a clear signal was detected with the EBV and influenza multimers. (b) Multi-centre CMV staining results. The %CV was 20 for sample 3. Remaining samples were negative. (c) Multi-centre EBV staining results. The %CV values were 42 for sample 1 and 48 for sample 4. Remaining samples were negative. (d) Multi-centre influenza staining results. The %CV values were 23 for sample 1, 45 for sample 2 and 25 for sample 3. Remaining samples were negative. Each y-axis indicates the observed percentage of live CD8+ T cells labelled with the corresponding Qdot pair after combinatorial gating. Symbols indicate different centres. No significant differences were observed across centres. Circles, Cardiff; squares, Leiden; triangles, Paris; inverted triangles, Seattle; hexagons, Denver
Single-centre reproducibility of multimer analysis of beta cell antigen-reactive CD8+ T cells
To validate the detection of beta cell antigen-specific CD8+ T cells, we first evaluated assay reproducibility in a single laboratory (Seattle) by staining three identical replicate vials from five HLA-A2+ individuals with type 1 diabetes (sample set 2). Each blind-coded sample was thawed, pre-treated with dasatinib, stained using multimer panel 2 (listed in Table 1) and analysed before unblinding. As summarised in Table 2, the assay exhibited good agreement between replicate samples based on the observed %CVs. The mean %CV across specificities for beta cell antigen multimers was 18.4. As expected, assay precision was better for viral specificities, with a mean %CV of 6.2. For replicate beta cell epitope-specific frequency measurements, SDs were consistent, ranging from 0.005 to 0.010. As a consequence, %CV values were highest for those specificities with the lowest frequencies in the sample set, such as islet-specific glucose-6-phosphatase catalytic subunit-related protein (IGRP), which yielded a mean %CV of 45.1.
Multi-centre reproducibility of multimer analysis of beta cell antigen-reactive CD8+ T cells
To evaluate assay reproducibility across multiple centres, nine samples from HLA-A2+ individuals with type 1 diabetes, ten samples from HLA-A2+ healthy donors and a clone-spiked sample (sample set 3) were distributed as identical replicate vials in a blinded fashion, pre-treated with dasatinib and stained using multimer panel 2 (listed in Table 1). Staining results for the spiked control and a representative sample are shown in Fig. 3a,b, respectively. For the spiked control sample, each centre observed positive staining (>0.1% of total CD8+ T cells) for the CMV- and PPI-specific clones (Fig. 3c) at percentages close to the theoretical spiked values (0.58% for CMV and 0.34% for PPI vs theoretical values of 0.55% and 0.38%, respectively).

Multimer analysis for beta cell antigens. (a) Dot plots show representative data for the clone-spiked sample, stained using beta cell antigen multimers and a pool of recall antigen multimers in Leiden. Each subpart depicts staining of live CD8+ T cells by the Qdot pair of interest after combinatorial gating. The sample was spiked with CMV- and PPI-specific CD8+ T cell clones. A clear signal was detected for each clone. (b) Dot plots show representative data for sample 16 (individual 338), stained using beta cell antigen multimers and a pool of recall antigen multimers in Leiden. Each subpart depicts staining for Qdot pairs as in part (a). Strong positive staining was observed with the recall antigen multimers, moderate positive staining was observed with the insulin B multimer and weak staining was observed with the GAD multimer. (c) Multimer staining results for the clone-spiked sample in each centre. The line indicates the mean value observed across all five centres. The %CV values were 20 for the non-interfacing multimer, 34 for the pool of recall antigen multimers, 47 for the insulin B multimer, 43 for the PPI multimer, 76 for the GAD multimer, 65 for the IA-2 multimer, 89 for the IGRP multimer and 68 for the IAPP multimer. Circles, Cardiff; squares, Leiden; triangles, Paris; inverted triangles, Seattle; hexagons, Denver. Flu, influenza M1; Ins B, insulin B; Neg, non-interfacing
Multimer staining results for each individual sample across all participating centres are shown in Fig. 4. Across all centres, background staining was typically low (with an overall mean of 0.0082% and an SD of 0.01% across all samples), and high positive results tended to be more consistent. To assess the technical reproducibility of the assay, we calculated %CVs across all multi-centre replicates for each multimer specificity (Table 3). The overall mean %CV was 119 for beta cell antigen multimers. As such, the multi-centre beta cell antigen data were 3.5-fold more dispersed than the multi-centre recall antigen data and approximately sixfold more dispersed than the single-centre beta cell antigen data. For replicate beta cell epitope-specific frequency measurements, SDs for the multi-centre data were also higher compared with the single-centre data, ranging from 0.007 to 0.11. %CV values were highest for the PPI epitope, which also had the highest SD, and lowest for the GAD and insulin B epitopes. The decreased precision of the multi-centre data is illustrative of the technical challenges associated with implementing a complex multi-parameter flow assay to perform rare-event analysis using non-identical cytometer configurations.

Multimer staining results for each individual sample across all participating centres. Each figure part depicts the percentage of live CD8+ T cells positive for the Qdot pair corresponding to (a) the non-interfacing control multimer, (b) the pool of recall antigen multimers, (c) the insulin B multimer, (d) the PPI multimer, (e) the GAD multimer, (f) the IA-2 multimer, (g) the IGRP multimer and (h) the IAPP multimer after combinatorial gating. In each graph, symbols indicate the corresponding % observed at each centre for samples 1–10 (healthy donors) and 11–19 (individuals with type 1 diabetes). Circles, Cardiff; squares, Leiden; triangles, Paris; inverted triangles, Seattle; hexagons, Denver
To further evaluate assay reproducibility across multiple centres, we analysed the data using one-way ANOVA. Systematic variation was not evident for the viral recall antigens or for the beta cell antigens GAD, islet antigen-2 (IA-2), IGRP or islet amyloid polypeptide (IAPP) (Fig. 5). However, significant differences were detected for the insulin B and PPI epitopes (Fig. 6). Specifically, higher frequencies of insulin B-specific CD8+ T cells were detected in Paris compared with Seattle or Leiden, and higher frequencies of PPI-specific CD8+ T cells were detected in Denver compared with all other participating centres. Equivalent differences were not observed for the spiked control sample. As the insulin B and PPI multimer staining data also had the highest SDs, it is likely that systematic error or technical issues contributed to the observed differences between centres.

Beta cell antigen multimer staining results with no significant differences between centres. Although staining levels differed substantially for different individuals, no significant differences were observed in the magnitude of staining with (a) the non-interfacing control multimer, (b) pooled CMV, EBV and influenza multimers, (c) the GAD multimer, (d) the IA-2 multimer, (e) the IGRP multimer or (f) the IAPP multimer. In each figure part, each symbol indicates the staining observed for a single individual (numbered as in ESM Table 3). Healthy donors (1–10) and individuals with type 1 diabetes (11–20) are designated consecutively in blue and red symbols, respectively, as follows: circle, square, upward triangle, downward triangle, diamond, half-filled circle, half-filled square, half-filled upward triangle, half-filled downward triangle and half-filled diamond

Beta cell antigen multimer staining results with significant differences between centres. (a) The magnitude of insulin B multimer staining was significantly lower in Leiden and Seattle than in Paris. (b) The magnitude of PPI multimer staining was significantly higher in Denver than in Cardiff, Leiden, Paris and Seattle. In each part, each symbol indicates the staining observed for a single individual, with the same colours and symbol designations as in Fig. 5. In all figure parts, * p < 0.05
Central calls were made for each sample before unblinding to assign individuals as having type 1 diabetes or healthy donor based on the presence or absence of multimer-positive populations (>0.05% of viable CD8+ T cells). As summarised in Table 4, these qualitative calls were moderately accurate, with average sensitivity of 68% and specificity of 76% (SDs were 11% and 10%, respectively). The same analysis was repeated in each individual centre (Table 5), but these qualitative calls were less favourable, with average sensitivity of 64% and specificity of 65% (SDs were 16% and 13%, respectively).
Aggregated analysis of beta cell antigen-reactive CD8+ T cells
To evaluate assay results in the context of disease status, multimer staining data from all centres were aggregated (barring data from the spiked sample and PPI-specific frequency measurements from Denver), and pairwise comparisons were performed between individuals with type 1 diabetes and healthy donors. The magnitude of staining with the insulin B and GAD multimers was significantly higher in samples from people with type 1 diabetes compared with samples from healthy donors (ESM Fig. 2). In contrast, no significant differences were observed between groups for PPI, IA-2, IGRP or IAPP. A contingency analysis was also performed by aggregating qualitative calls (ESM Table 5). Samples with GAD multimer-positive populations (>0.05% of viable CD8+ T cells) were significantly enriched in the type 1 diabetes group (21/45 vs 8/50, p = 0.001). Samples with at least one detectable beta cell antigen-reactive CD8+ T cell population were also significantly enriched in the diabetes group (32/45 vs 20/50, p = 0.002). Accordingly, beta cell antigen reactivity within the peripheral CD8+ T cell compartment appears to be more common in individuals with type 1 diabetes relative to a healthy control group.
Discussion
The importance of autoreactive CD8+ T cells is established in autoimmune diabetes. However, the availability of assays to enumerate beta cell antigen-specific CD8+ T cells remains limited. Here, we report the findings of a multi-centre study designed to test the reproducibility of a combinatorial HLA class I multimer assay for the detection and quantification of beta cell antigen-reactive CD8+ T cells in cryopreserved samples of PBMCs. From a logistical standpoint, the study was satisfactory. Acceptable post-thaw viability and sample recovery rates were observed across participating centres, and technically reproducible results were achieved for measurements of recall antigen-specific CD8+ T cells, which typically circulate in high numbers. These data concur with previous studies [14, 15, 23]. Similarly consistent results were achieved in a single-centre setting, where low %CVs across technical replicates were apparent not only for recall antigens, but also for beta cell antigens. Of note, the corresponding %CV values were approximately sixfold higher in multi-centre replicates, indicating greater technical variability.
ANOVA suggested that systematic error or technical issues contributed to the observed differences between centres. The most notable disparities were apparent for measurements of PPI-specific CD8+ T cells in Denver. For logistical reasons, these samples were processed several months after the corresponding analyses in other centres. It is therefore possible that degradation of the PPI monomer over time contributed to increased levels of background staining. Alternatively, this site-specific difference could reflect a technical issue with the relevant combination of Qdots, linked to minor differences in cytometer configuration. This issue was not discernible for the spiked control sample, probably because of a stronger positive signal in that detection channel. Future studies may benefit from the incorporation of a non-spiked negative control or two partially spiked controls to screen for such technical issues. Significant differences in variance were also observed for insulin B-specific CD8+ T cell frequencies, suggesting a separate technical issue. However, it is difficult to establish whether the magnitude of this multimer-positive population was systematically underestimated in Seattle and Leiden or overestimated in Paris.
Direct comparisons revealed that two beta cell antigen-specific CD8+ T cell populations occurred at higher frequencies in individuals with diabetes vs healthy donors. The most significant difference was observed for insulin B. This epitope is present in exogenous insulin, which is injected daily by individuals with type 1 diabetes. GAD-specific cells were also present in elevated numbers. Dasatinib may have affected the distinction between individuals with diabetes and healthy donors by enhancing detection of low-affinity T cells, thereby potentially increasing the level of staining observed in the absence of active disease. As some beta cell antigen-specific CD8+ T cell populations occurred at comparatively low frequencies that did not differ significantly between individuals with diabetes and healthy donors, further efforts to improve assay harmonisation through protocol standardisation may be worthwhile. In addition, pre-enrichment strategies may facilitate the detection of low-frequency beta cell antigen-reactive CD8+ T cells. However, further research is required to determine if the measurement of such low-frequency specificities is informative, especially across longitudinal series of samples. Comparing the prevalence of aggregated positive multimer stains, we detected GAD-specific CD8+ T cells more commonly in individuals with diabetes vs healthy donors, as reported previously using different assays [7, 24,25,26,27]. Furthermore, across all beta cell epitopes, the prevalence of positive multimer stains was higher in individuals with diabetes vs healthy donors. These findings suggest that analysis of beta cell antigen-reactive CD8+ T cells for the purposes of disease classification would be most successful if multiple specificities were measured in parallel.
The disease specificity of the insulin B epitope was limited by the occurrence of positive results in some healthy donors. However, several of these control samples were only weakly positive, whereas a slightly higher number of samples from individuals with diabetes were more strongly positive. Assay specificity may therefore be improved further by increasing the positive threshold for this particular multimer. Indeed, future studies could benefit from setting unique thresholds for each beta cell epitope. As our staining panel did not include additional phenotypic markers, it was not possible to determine whether healthy individuals harbour unprimed naive T cells that recognise the insulin B epitope or whether the corresponding multimer displays a high level of background staining, possibly reflecting unexpected cross-reactivity with another specificity unrelated to the disease process. Although it is possible that dasatinib may obscure some differences between individuals with diabetes and healthy donors as a consequence of its enhancement of detection thresholds [20], a recent study has suggested otherwise [27]. Accordingly, future work may benefit from the incorporation of additional phenotypic markers and systematic evaluation of the effects of dasatinib.
The goal of our study was to demonstrate that a complex HLA class I multimer assay could be implemented to provide technically reproducible results in multiple laboratories. Although our results are promising, assay reproducibility was higher in a single-centre setting. It may therefore be advisable to perform comparative evaluations in one laboratory, at least pending further standardisation of cytometry platforms, for example, via the introduction of photonic scales. Conceptually, multimer-based assays will be most informative for the evaluation of immune interventions designed to alter the frequencies of antigen-specific T cells, although further studies will be required to support the clinical relevance of such measurements. Such assays may also be well suited to investigate the phenomenon of epitope spreading, where different epitopes are recognised as a consequence of disease progression [28]. In this setting, combinatorial multimer assays may allow the identification of ‘at-risk’ individuals and facilitate the stratification of individuals with established disease. The simultaneous evaluation of T cell phenotype, allowing inferences about memory status and functional attributes, may further enhance the utility of combinatorial multimer assays. In response to this suggestion, three of the groups that participated in this project are developing staining panels that include C-C motif chemokine receptor 7 (CCR7) and CD45RA to partition beta cell antigen-specific CD8+ T cells into naive, central memory, effector memory and terminally differentiated effector memory compartments. Other additions to the assay should be technically feasible, and downstream gene expression studies of multimer-positive T cells may provide further useful information [25, 29]. It will also be important to extend this approach to other HLA class I molecules that present disease-relevant epitopes. Indeed, published data have already shown that multimer-based assays can be used to detect beta cell antigen-specific CD8+ T cells restricted by HLA-A*01, HLA-A*03, HLA-A*11 and HLA-B*07 [30,31,32].
In conclusion, the present study supports the feasibility of monitoring beta cell antigen-reactive CD8+ T cells using a combinatorial multimer staining approach. The assay was very effective in a single-centre setting, but showed greater variability across multi-centre replicates. Furthermore, the enumeration of beta cell antigen-specific CD8+ T cells revealed quantitative differences between individuals with diabetes and healthy donors. Collectively, these data highlight the potential utility and current limitations of combinatorial multimer staining in the context of type 1 diabetes.
Abbreviations
- BRI:
-
Benaroya Research Institute
- CMV:
-
Cytomegalovirus
- EBV:
-
Epstein–Barr virus
- HLA-A2+ :
-
HLA-A*02:01+
- IA-2:
-
Islet antigen-2
- IAPP:
-
Islet amyloid polypeptide
- IGRP:
-
Islet-specific glucose-6-phosphatase catalytic subunit-related protein
- NIH:
-
National Institutes of Health
- PBMC:
-
Peripheral blood mononuclear cell
- PPI:
-
Preproinsulin
References
Roep BO, Peakman M (2010) Surrogate end points in the design of immunotherapy trials: emerging lessons from type 1 diabetes. Nat Rev Immunol 10:145–152
Culina S, Boitard C, Mallone R (2011) Antigen-based immune therapeutics for type 1 diabetes: magic bullets or ordinary blanks? Clin Dev Immunol 2011:286248
Mallone R, Roep BO (2013) Biomarkers for immune intervention trials in type 1 diabetes. Clin Immunol 149:286–296
Coppieters KT, Dotta F, Amirian N et al (2012) Demonstration of islet-autoreactive CD8 T cells in insulitic lesions from recent onset and long-term type 1 diabetes patients. J Exp Med 209:51–60
Willcox A, Richardson SJ, Bone AJ, Foulis AK, Morgan NG (2009) Analysis of islet inflammation in human type 1 diabetes. Clin Exp Immunol 155:173–181
Sibley RK, Sutherland DE, Goetz F, Michael AF (1985) Recurrent diabetes mellitus in the pancreas iso- and allograft. A light and electron microscopic and immunohistochemical analysis of four cases. Lab Inv J Tech Methods Path 53:132–144
Skowera A, Ellis RJ, Varela-Calvino R et al (2008) CTLs are targeted to kill beta cells in patients with type 1 diabetes through recognition of a glucose-regulated preproinsulin epitope. J Clin Invest 118:3390–3402
Katz J, Benoist C, Mathis D (1993) Major histocompatibility complex class I molecules are required for the development of insulitis in non-obese diabetic mice. Eur J Immunol 23:3358–3360
Nagata M, Santamaria P, Kawamura T, Utsugi T, Yoon JW (1994) Evidence for the role of CD8+ cytotoxic T cells in the destruction of pancreatic beta-cells in nonobese diabetic mice. J Immunol 152:2042–2050
Graser RT, DiLorenzo TP, Wang F et al (2000) Identification of a CD8 T cell that can independently mediate autoimmune diabetes development in the complete absence of CD4 T cell helper functions. J Immunol 164:3913–3918
Wong FS, Visintin I, Wen L, Flavell RA, Janeway CA Jr (1996) CD8 T cell clones from young nonobese diabetic (NOD) islets can transfer rapid onset of diabetes in NOD mice in the absence of CD4 cells. J Exp Med 183:67–76
Nejentsev S, Howson JM, Walker NM et al (2007) Localization of type 1 diabetes susceptibility to the MHC class I genes HLA-B and HLA-A. Nature 450:887–892
Noble JA, Valdes AM, Varney MD et al (2010) HLA class I and genetic susceptibility to type 1 diabetes: results from the Type 1 Diabetes Genetics Consortium. Diabetes 59:2972–2979
Velthuis JH, Unger WW, Abreu JR et al (2010) Simultaneous detection of circulating autoreactive CD8+ T cells specific for different islet cell-associated epitopes using combinatorial MHC multimers. Diabetes 59:1721–1730
Newell EW, Klein LO, Yu W, Davis MM (2009) Simultaneous detection of many T cell specificities using combinatorial tetramer staining. Nat Methods 6:497–499
Mallone R, Scotto M, Janicki CN et al (2011) Immunology of Diabetes Society T-Cell Workshop: HLA class I tetramer-directed epitope validation initiative T-Cell Workshop Report-HLA Class I Tetramer Validation Initiative. Diabetes Metab Res Rev 27:720–726
Hadrup SR, Bakker AH, Shu CJ et al (2009) Parallel detection of antigen-specific T cell responses by multidimensional encoding of MHC multimers. Nat Methods 6:520–526
Andersen RS, Kvistborg P, Frosig TM et al (2012) Parallel detection of antigen-specific T cell responses by combinatorial encoding of MHC multimers. Nat Protoc 7:891–902
Newell EW, Sigal N, Nair N, Kidd BA, Greenberg HB, Davis MM (2013) Combinatorial tetramer staining and mass cytometry analysis facilitate T cell epitope mapping and characterization. Nat Biotechnol 31:623–629
Lissina A, Ladell K, Skowera A et al (2009) Protein kinase inhibitors substantially improve the physical detection of T cells with peptide-MHC tetramers. J Immunol Methods 340:11–24
Brooks-Worrell B, Tree T, Mannering SI et al (2011) Comparison of cryopreservation methods on T cell responses to islet and control antigens from type 1 diabetic patients and controls. Diabetes Metab Res Rev 27:737–745
Mallone R, Mannering SI, Brooks-Worrell BM et al (2011) Isolation and preservation of peripheral blood mononuclear cells for analysis of islet antigen-reactive T cell responses: position statement of the T-Cell Workshop Committee of the Immunology of Diabetes Society. Clin Exp Immunol 163:33–49
Roep BO, Solvason N, Gottlieb PA et al (2013) Plasmid-encoded proinsulin preserves C-peptide while specifically reducing proinsulin-specific CD8(+) T cells in type 1 diabetes. Sci Transl Med 5:191ra182
Toma A, Laika T, Haddouk S et al (2009) Recognition of human proinsulin leader sequence by class I-restricted T cells in HLA-A*0201 transgenic mice and in human type 1 diabetes. Diabetes 58:394–402
Luce S, Lemonnier F, Briand JP et al (2011) Single insulin-specific CD8+ T cells show characteristic gene expression profiles in human type 1 diabetes. Diabetes 60:3289–3299
Mallone R, Martinuzzi E, Blancou P et al (2007) CD8+ T cell responses identify beta-cell autoimmunity in human type 1 diabetes. Diabetes 56:613–621
Skowera A, Ladell K, McLaren JE et al (2015) beta-cell-specific CD8 T cell phenotype in type 1 diabetes reflects chronic autoantigen exposure. Diabetes 64:916–925
Martinuzzi E, Novelli G, Scotto M et al (2008) The frequency and immunodominance of islet-specific CD8+ T cell responses change after type 1 diabetes diagnosis and treatment. Diabetes 57:1312–1320
Eugster A, Lindner A, Heninger AK et al (2013) Measuring T cell receptor and T cell gene expression diversity in antigen-responsive human CD4+ T cells. J Immunol Methods 400-401:13–22
Sachdeva N, Paul M, Badal D et al (2015) Preproinsulin specific CD8+ T cells in subjects with latent autoimmune diabetes show lower frequency and different pathophysiological characteristics than those with type 1 diabetes. Clin Immunol 157:78–90
Scotto M, Afonso G, Osterbye T et al (2012) HLA-B7-restricted islet epitopes are differentially recognized in type 1 diabetic children and adults and form weak peptide-HLA complexes. Diabetes 61:2546–2555
Unger WW, Velthuis J, Abreu JR et al (2011) Discovery of low-affinity preproinsulin epitopes and detection of autoreactive CD8 T cells using combinatorial MHC multimers. J Autoimmun 37:151–159
Acknowledgements
We thank M. Lettau and J. Klein (Clinical Research, BRI) for assistance with recruitment, M. Scotto (Diabetes & Autoimmunity Research [DEAR] Laboratory, Inserm) for technical assistance, C. Greenbaum (Diabetes, BRI) for sample selection oversight and useful discussions, and D. Sorus (Administration, BRI) for administrative support. We also thank the JDRF Biomarker Working Group, the JDRF Core and Validation Center, and Demonstration Project investigators for useful discussions and facilitation of precision testing of replicates. All HLA-A2 monomer reagents were obtained through the NIH Tetramer Core Facility.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
The data that support the findings of this study are available from the corresponding author on reasonable request.
Funding
Funding for this research was provided by JDRF grant 17-2012-559 to EAJ and RM. DAP is funded by a Wellcome Trust Senior Investigator Award (100326/Z/12/Z).
Duality of interest
The authors declare that there is no duality of interest associated with this manuscript.
Contribution statement
EAJ and RM coordinated the study and co-wrote the manuscript. EAJ, JRFA, JWM, YEF, CNH, SC, KL, DAP, AA, MR, LFM, FSW and RM performed and/or supervised experiments and analysed results. JMO and CS assisted with study design, participant selection and provided IRB-approved human samples. AS provided T cell clones, assisted with study design and data interpretation. EAJ performed centralised data analysis. JRFA, JMO, CNH, KL, DAP, CS, PG, HWD, FSW and BR contributed to the conception and design of the study and interpretation of the data. JRFA, JMO, JWM, YEF, SC, AA, CNH, KL, DAP, CS, PG, HWD, FSW MR, LFM, AS and BR edited the manuscript. All authors have given final approval of the version to be published. EAJ is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Electronic supplementary material
ESM
(PDF 713 kb)
Rights and permissions
About this article

Cite this article
James, E.A., Abreu, J.R.F., McGinty, J.W. et al. Combinatorial detection of autoreactive CD8+ T cells with HLA-A2 multimers: a multi-centre study by the Immunology of Diabetes Society T Cell Workshop. Diabetologia 61, 658–670 (2018). https://doi.org/10.1007/s00125-017-4508-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-017-4508-8