
Abstract
Purpose
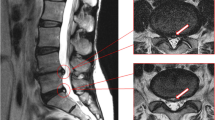
The purpose of this study is to investigate if lumbar disc pathology identified on MRI scans is more common in patients with acute, likely discogenic, low back pain than matched controls.
Methods
We compared rates of MRI findings between 30 cases with low back pain and 30 pain-free controls. Cases were patients presenting for care with likely discogenic low back pain (demonstrated centralisation with repeated movement testing), of moderate intensity and with minimal past history of back pain. Controls were matched for age, gender and past history of back pain. Cases and controls underwent MRI scanning which was read for the presence of a range of MRI findings by two blinded assessors.
Results
The presence of disc degeneration, modic changes and disc herniation significantly altered the odds of a participant being a case or control. For example subjects were 5.2 times more likely to be a case than a control when disc degeneration grade of ≥3 was present, and 6.0 times more likely with modic changes. The presence of a high-intensity zone or annular tear was found to significantly alter odds for one assessor but not the other assessor.
Conclusion
MRI findings including disc degeneration, modic changes and herniation are more common in selected people with current acute (likely discogenic) low back pain than in controls without current low back pain. Further investigation of the value of MRI findings as prognostic factors and as treatment effect modifiers is required to assess the potential clinical importance of these findings.

Similar content being viewed by others


References
van Tulder M, Becker A, Bekkering T, Breen A, del Real MTG, Hutchinson A, Koes B, Laerum E, Malmivaara A, Cost B13 Working Group on Guidelines for the Management of Acute Low Back Pain in Primary Care (2006) Chapter 3. European guidelines for the management of acute nonspecific low back pain in primary care. Eur Spine J 15(Suppl 2):S169–S191
Australian Acute Musculoskeletal Pain Guidelines Group (2004) Evidence-based management of acute musculoskeletal pain—a guide for clinicians. Australian Academic Press, Bowen Hills
Deyo RA (2004) Treatments for back pain: can we get past trivial effects? Ann Intern Med 141:957–958
Keller A, Hayden J, Bombardier C, van Tulder M (2007) Effect sizes of non-surgical treatments of non-specific low-back pain. Eur Spine J 16:1776–1788
Merskey H, Bogduk N (1994) Classification of chronic pain: descriptions of chronic pain syndromes and definitions of pain terms. IASP Press, Seattle
Standards Committee of the International Spine Intervention Society (2004) International Spine Intervention Society practice guidelines for spinal diagnostic and treatment procedures In: Bogduk N (ed) International Spine Intervention Society
Schwarzer AC, Aprill CN, Derby R, Fortin J, Kine G, Bogduk N (1995) The prevalence and clinical features of internal disc disruption in patients with chronic low back pain. Spine 20:1878–1883
Hancock MJ, Maher CG, Latimer J, Spindler MF, McAuley JH, Laslett M, Bogduk N (2007) Systematic review of tests to identify the disc, SIJ or facet joint as the source of low back pain. Eur Spine J 16:1539–1550
Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malkasian D, Ross JS (1994) Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med 331:69–73
Boden SD, Davis DO, Dina TS, Patronas NJ, Wiesel SW (1990) Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am 72:403–408
Cheung KM, Karppinen J, Chan D, Ho DW, Song YQ, Sham P, Cheah KS, Leong JC, Luk KD (2009) Prevalence and pattern of lumbar magnetic resonance imaging changes in a population study of one thousand forty-three individuals. Spine 34:934–940
Jarvik JJ, Hollingworth W, Heagerty P, Haynor DR, Deyo RA (2001) The Longitudinal Assessment of Imaging and Disability of the Back (LAIDBack) Study: baseline data. Spine 26:1158–1166
Laslett M, Aprill CN, McDonald B, Oberg B, Laslett M, Aprill CN, McDonald B, Oberg B (2006) Clinical predictors of lumbar provocation discography: a study of clinical predictors of lumbar provocation discography. Eur Spine J 15:1473–1484
Donelson R, Aprill C, Medcalf R, Grant W (1997) A prospective study of centralization of lumbar and referred pain. A predictor of symptomatic discs and anular competence. Spine 22:1115–1122
Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N (2001) Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine 26:1873–1878
Aprill C, Bogduk N (1992) High-intensity zone: a diagnostic sign of painful lumbar disc on magnetic resonance imaging. Br J Radiol 65:361–369
Fardon DF, Milette PC, Combined Task Forces of the North American Spine Society ASoSR, American Society of N (2001) Nomenclature and classification of lumbar disc pathology. Recommendations of the Combined task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. Spine 26:E93–E113
Jensen TS, Karppinen J, Sorensen JS, Niinimaki J, Leboeuf-Yde C (2008) Vertebral endplate signal changes (Modic change): a systematic literature review of prevalence and association with non-specific low back pain. Eur Spine J 17:1407–1422
Acknowledgments
This work was supported by Faculty of Health Sciences Grant, The University of Sydney.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hancock, M., Maher, C., Macaskill, P. et al. MRI findings are more common in selected patients with acute low back pain than controls?. Eur Spine J 21, 240–246 (2012). https://doi.org/10.1007/s00586-011-1955-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-011-1955-7