
Abstract
Humanized mice have recently emerged as powerful translational animal models for studying human hematopoiesis, immune interactions, and diseases of the human immune system. Several important advances in the humanized mouse technology have been reported over the last few years, thereby resulting in improved engraftment, high levels of human chimerism, and sustained human hematopoiesis. This chapter describes the detailed procedures for generating various humanized mouse models including hu-PBL, hu-HSC, and BLT models and discusses considerations for choosing the appropriate model system.
1 Introduction
The lack of an appropriate small animal model is a major impediment for investigation of the human immune system in vivo. Over the years there has been a considerable effort to develop “humanized” mouse models harboring a functional human immune system. Although technically, it is possible to enforce human transgene expression in immunocompetent mice, only immunodeficient mice are receptive to engraftment with human hematopoietic or lymphoid cells or tissues (1). Such humanized mice provide valuable new tools to translate basic research findings into clinical applications for various human diseases including autoimmunity, transplantation, infectious diseases, and cancer for which appropriate small animal model are unavailable (2). HIV research, in particular, has gained a tremendous boost with the development of humanized mouse models that are permissive to the uniquely human-tropic HIV-1 and display symptoms that closely mirror human HIV infection (3, 4).
Successful transplantation of human cells or fetal tissues with hematopoietic potential was first achieved in severe combined immunodeficient (SCID) mice, which lack functional T and B lymphocytes. However, these were not ideal animal models since they still possessed significant levels of active innate immune responses that hindered complete engraftment of human hematopoietic cells. Therefore, several other mouse strains were developed in the quest for a model that can support the stable engraftment and growth of human hematopoietic cells (extensively reviewed in (1)). NOD/SCID mice, which were created by back-crossing the SCID gene onto the non-obese diabetic (NOD) background, proved a better engrafting strain as they have impaired natural killer (NK) and antigen-presenting cell function in addition to lacking functional T and B lymphocytes. However, engraftment and long-term maintenance of human cells was still inadequate due to residual innate immune activity. A further advance that represents a major leap forward is the development of immunodeficient mouse strains lacking a functional IL-2 cytokine receptor gamma chain (IL2rγnull), including NOD/Shi-Scid IL2rγnull(5, 6), NOD/SCID IL2rγnull(7), and BALB/c-Rag2nullIL2rγnullmice (8). Since the IL2rγ functions as a common component of receptors for the interleukins 2, 4, 7, 9, 15, and 21, the IL2rγnullmice completely lack adaptive immune function and display multiple defects in innate immunity, features that allow heightened levels of human hematopoietic/lymphoid cell engraftment. In addition to better engraftment, many of the recently described IL2rγnullmouse strains also have a longer life span, so they can serve as better models for human diseases compared to the previously available strains (1).
IL2rγnullstrains can be used for short-term reconstitution with human peripheral blood mononuclear cells (PBMCs) or long-term de novo generation of immune progeny cells from engrafted human hematopoietic stem cells (HSCs). The PBMC model (hu-PBL) utilizes leukocytes isolated from peripheral whole blood for rapid reconstitution with functionally mature lymphocytes. The advantages of this model are the simple procedure of generation and quick availability for experimentation as animals are reconstituted within 3–4 days of PBMC transfer. This model is best suited for short-term experiments (upto 4 weeks) because of the short duration of human reconstitution and the development of graft-versus-host disease (GVHD). In this model, adoptively transferred human T cells undergo expansion in response to xenogenic stimulation so they display a predominantly activated phenotype. Therefore, the hu-PBL model is suitable for the study of activated human lymphocytes but not resting T cells. For example, the availability of antibodies that selectively target the activated form of the integrin leukocyte function-associated antigen-1 (LFA-1), would make it possible to evaluate targeted delivery approaches to activated leukocytes. The hu-PBL model would serve well for validating RNA interference (RNAi)-based interventions for autoimmune diseases, GVHD, and septic shock where selective delivery of small interference RNA (siRNA) to activated leukocytes can prove useful for silencing genes involved in the proinflammatory cascade and/or T cell activation (9).
The HSC model (hu-HSC) utilizes CD34+HSCs isolated from human cord blood or fetal liver tissue to reconstitute immunodeficient mice. The advantage of the hu-HSC model is that the human T and B lymphocytes that develop from human stem cells engrafted in these mice are tolerant of the mouse host, possibly because of negative selection during lymphocyte differentiation in the mouse thymus. In addition, in contrast to T cells from hu-PBL mice, which display a predominantly activated phenotype, the T cells in this hu-HSC model are predominantly naive and unactivated. This model allows for the investigations of hemato-poietic lineage development, and the generation of primary immune responses by a naive immune system. Accordingly, novel drug delivery systems driven by antibodies targeting the LFA-1 integrin receptors in a nonactivated conformation can be tested for in vivo applicability in this model (10).
Although now widely popular, this model still suffers from drawbacks of inefficient human thymopoiesis in the xenogenic recipient thymus (11). In an earlier NOD/SCID hu/HSC model, human fetal liver derived HSCs were transferred into surgically implanted human fetal thymic tissue which resulted in successful development of human T cells (human thymopoiesis) within the autologous human thymus graft. However, the usefulness of the human fetal tissue grafted mice was limited because the distribution of human cells was confined to the implant only (12, 13). To mitigate this problem, the approach has been modified recently, with the additional step of intravenous transfer of autologous CD34+HSCs obtained from fetal liver along with the surgical implantation of human fetal thymus/liver tissues (11, 14). In this humanized mouse model, referred to as BLT (for bone marrow, liver, and thymus) mice, HSCs take up residence in the mouse bone marrow and give rise to immune progeny consisting of all major human hematopoietic lineages including T and B cells, monocytes, macrophages, and dendritic cells (11). Furthermore, BLT mice also exhibit extensive infiltration of organs including liver, lung, gastrointestinal tract, and female reproductive tissues with human immune cells (4). Education in the autologous human thymic milieu provided by the surgically implanted tissue is also likely to be lead to the proper development of the T cell repertoire in these mice. All these reasons uphold the BLT mice as a useful in vivo model for an authentic study of the human immune system. In fact, this mouse model has been demonstrated to successfully support long-lasting HIV infection with both macrophage and T cell tropic strains of HIV (4, 15, 16). A disadvantage of the hu-HSC and BLT models, in comparison to the hu-PBL model, is the longer reconstitution time (10–12 weeks) for the complete development of the human immune system from engrafted HSCs. These models also involve more complicated generation procedures.
While any of the IL2rγ nullmouse strains (5–8) are good hosts for generating humanized mouse models, this chapter will detail the generation of the hu-PBL, hu-HSC, and BLT models by engraftment of immunodeficient NOD/SCID IL2rγnullmice with human PBMCs, HSCs, or fetal liver/thymus tissues and CD34+fetal liver cells, respectively.
2 Materials
2.1 hu-PBL Model (Fig. 1a)
-
1.
Healthy donor peripheral blood.
-
2.
Dulbecco’s phosphate-buffered saline (PBS) 1× sterile, without calcium and magnesium.
-
3.
Complete RPMI 1640 medium: RPMI 1640 supplemented with 10% heat-inactivated fetal bovine serum (FBS), 50 U/ml penicillin, 50 mg/ml streptomycin, 2 mM glutamine, 1 mM sodium pyruvate.
-
4.
Ficoll (GE Healthcare Bio-sciences, Piscataway, NJ).
-
5.
Nonobese diabetic–severe combined immunodeficient NOD.cg-Prkdc scidIL2rgtm/Wjl/Sz (NOD/SCID IL2rγnull) mice (male or female, 5–12 weeks old; Jackson Laboratory, Bar Harbor, ME) (see Note 1).
-
6.
25-G needles.
-
7.
1-cc syringes.
-
8.
Alcohol swab.
-
9.
Sterile gauze pad.
2.2 The hu-HSC Model (Fig. 1b)
Although successful hematopoiesis for most lineages is achieved by HSC engraftment of adult mice, T cell reconstitution is variable and not always efficient. HSC engraftment of newborn mice requires technical proficiency but results in more robust human HSC engraftment and consistent reconstitution of all hematopoietic lineages, including T cells.

Schematic representation of transplantation techniques for generation of humanized mice. (a) hu-PBL model. (b) hu-HSC model. (c) BLT model.
-
1.
Human umbilical cord blood (see Note 3).
-
2.
Dulbecco’s PBS 1× sterile, without calcium and magnesium.
-
3.
Ficoll.
-
4.
Complete RPMI 1640 medium: RPMI 1640 supplemented with 10% heat-inactivated FBS, 50 U/ml penicillin, 50 mg/ml streptomycin, 2 mM glutamine, and 1 mM sodium pyruvate.
-
5.
Anti-CD34 microbeads (Miltenyi Biotech, Auburn, CA): Used for magnetic-activated cell sorter (MACS) separation.
-
6.
MACS separation apparatus and MACS LS separation columns (Miltenyi Biotech).
-
7.
Nonobese diabetic–severe combined immunodeficient NOD.cg-Prkdc scidIL2rgtm/Wjl/Sz (NOD/SCID IL2rγ null) breeder pairs.
-
8.
Cesium gamma irradiator or X-ray biological irradiator.
-
9.
Sterile autoclaved mouse housing device for irradiation.
-
10.
27-G 1/ 2-in. winged infusion set.
-
11.
Nasal decongestant like Vicks Vaporub.
-
12.
Heat lamp.
-
13.
Alcohol swab.
-
14.
Sterile gauze pad.
2.3 BLT Model (Fig. 1c)
2.3.1 CD34+ Cell Isolation from Fetal Liver Tissue
-
1.
Human fetal thymus and liver tissues (gestational age of 17–20 weeks; Advanced Bioscience Resource, Alameda, CA).
-
2.
Complete RPMI 1640 medium.
-
3.
Collagenase/dispase solution: Complete RPMI 1640 medium supplemented with 1 mg/ml collagenase/dispase (Roche, Mannheim) and 0.5 U/ml DNase I (Roche).
-
4.
70-μm nylon mesh or cell strainer.
-
5.
Razor blade.
-
6.
Dulbecco’s PBS 1× sterile, without calcium and magnesium.
-
7.
Ficoll.
-
8.
Anti-CD34 microbeads for MACS separation.
-
9.
MACS separation apparatus and MACS LS separation columns.
2.3.2 Preconditioning and Tissue Implantation
-
1.
Nonobese diabetic–severe combined immunodeficient NOD.cg-Prkdc scidIL2rgtm/Wjl/Sz (NOD/SCID IL2rγ null) mice (female, 6–8 weeks old).
-
2.
Cesium gamma irradiator or X-ray biological irradiator.
-
3.
Ketamine/Xylazine.
-
4.
Buprenorphine: Add 200 μl of 0.3 mg/ml buprenorphine to 5.8 ml sterile saline.
-
5.
Alcohol swab.
-
6.
Ophthalmic ointment (Vetropolycin; Pharmaderm Animal Health, Melville, NY).
-
7.
Electric hair clipper.
-
8.
Temperature-controlled heating pad.
-
9.
Betadine (PDI Inc., Orengeburg, NY).
-
10.
Surgical scalpel.
-
11.
Sterile gauze pad.
-
12.
Sterile saline.
-
13.
Autoclaved tip with a blunt ball-shaped front.
-
14.
18-G blunt head spinal needles.
-
15.
4–0 absorbable vicryl and non-absorbable sutures.
-
16.
29-G needle/syringe from ultra-fine II insulin syringes.
-
17.
1-cc syringes.
-
18.
27-G needles.
-
19.
Heat lamp.
-
20.
Mouse restrainer.
2.4 Analysis of Reconstitution
-
1.
Isoflurane.
-
2.
Vacutainer heparinized blood collection tube.
-
3.
Heparinized micro-hematocrit capillary tubes.
-
4.
Red blood cell lysing buffer.
-
5.
Anti-human monoclonal antibodies to CD3, CD4, CD8, CD11c, CD19, CD34, CD45, and CD45RA; anti-mouse monoclonal antibody to CD45; and isotype control monoclonal antibodies (BD PharMingen, San Diego, CA).
-
6.
FACSCanto II and FACSDiva software (Becton Dickinson, Mountain View, CA).
3 Methods
3.1 hu-PBL Model
-
1.
Isolate PBMC from whole blood by Ficoll density gradient centrifugation.
-
2.
Resuspend cells at 5–10 × 106per 0.5 ml of sterile RPMI media.
-
3.
Inject 0.5 ml of cell suspension (5–10 × 106PBMCs) into peritoneal cavity using 1-cc syringe with 25-G needle.
-
4.
Monitor mice daily for signs of distress (see Note 2).
-
5.
Test cell engraftment 3–4 days after PBMC-transplantation.
3.2 The hu-HSC Model
-
1.
Monitor breeder pairs for the birth of new litters. Engraftment procedures are performed on 24–48 h postnatal newborn pups.
-
2.
Isolate mononuclear cells from human umbilical cord blood using Ficoll density gradient.
-
3.
Isolate CD34+cells from mononuclear cells using the MACS separation system with anti-CD34 microbeads.
-
4.
Resuspend isolated CD34+cells in a complete RPMI media (6 × 105cells per 0.1 ml RPMI media) and keep on ice until transplanted.
-
5.
Stain a small proportion of the isolated CD34+cells with the mouse anti-human monoclonal antibodies to CD34 and CD3, and analyze by flow cytometry for CD34 expression and residual CD3+ T cells to assess the efficacy of magnetic bead isolation (see Note 4).
-
6.
Place pups in autoclaved sterile irradiation container.
-
7.
Irradiate pups with 100 cGy whole-body irradiation.
-
8.
Place irradiated pups on a gauze pad on ice for 5–10 min, until gross movement ceases (ensure that there is no direct contact with ice).
-
9.
Load the CD34+ HSC cell suspension into a 1-ml syringe fitted with a 27-G 1/2-in. winged infusion set.
-
10.
CD34+ cells can be transplanted through several routes; however, the two described below are the most reproducible and yield the best efficiencies
-
(a)
Intracardiac injection: Upon sufficient anesthesia, visualize the apex of the heart and insert the needle slightly above the apex in an upward direction. A little flicker of blood will appear at the base of the needle. Slowly inject 3 × 105CD34+cells in a 50-μl volume.
-
(b)
Intrahepatic injection: 3 × 105CD34+ cells in a 50-μl volume directly into the liver taking care not to pierce the entire liver.
-
(a)
-
11.
Place the pups on a warming pad or under an incandescent lamp for 1–2 min.
-
12.
Apply a small amount of nasal decongestant to the snout of both parents before returning pups to prevent scents that have transferred to the pups during handling.
-
13.
Wean pups between 3–4 weeks of age and verify engraftment at 12 weeks of age.
3.3 BLT Model
3.3.1 CD34+ Cell Isolation from Fetal Liver Tissue
-
1.
Cut fetal liver tissue into small pieces (∼1 mm3) using an autoclaved surgical scalpel (see Notes 5and 6).
-
2.
Digest small tissue pieces using sterile filtered complete RPMI supplemented with 1 mg/ml collagenase/dispase and 0.5 U/ml DNase I at 37°C for 1 h.
-
3.
Gently disrupt the tissues by mixing every 15 min.
-
4.
Filter the cell suspension through a 70-μm mesh.
-
5.
Apply filtered cells on Ficoll to separate mononuclear cells.
-
6.
Isolate CD34+cells from mononuclear cells using the magnetic-activated cell sorter (MACS) separation system with anti-CD34 microbeads.
-
7.
Resuspend cells in a complete RPMI media (1–5 × 105cells per 0.2 ml RPMI media) and keep on ice until transplanted.
-
8.
Stain a small proportion of the isolated CD34+cells with the mouse anti-human monoclonal antibodies to CD34 and CD3, and analyze by flow cytometry for CD34 expression and residual CD3+ T cells to assess the efficacy of magnetic bead isolation.
3.3.2 Preparation of Immunodeficient Mice
-
1.
Place mice in an autoclaved irradiation container and condition with sublethal whole-body irradiation using X-ray Biological Irradiator or Cesium gamma irradiator.
-
2.
The dose of irradiation varies from 240 to 375 cGy depending on the mouse strain and irradiation source (see Note 7).
-
3.
Anesthetize mice with ketamine (80 mg/kg) and xylazine (12 mg/kg) by intraperitoneal injection in PBS (10 ml/kg) based on individual animal body weight (see Notes 8and 9).
3.3.3 Human Fetal Tissue Implantation
-
1.
After inducing anesthesia, shave anterior abdominal skin using an electric hair clipper.
-
2.
Place the body on a sterile support and fix the limbs with scotch tape.
-
3.
Disinfect the skin of abdomen with betadine.
-
4.
Make a 2–3 cm long midline incision of the abdominal skin and peritoneal membrane using a surgical scalpel.
-
5.
Gently pull the intestines and spleen to the opposite side of the kidney and cover them with pre-warmed moisturized gauze pad.
-
6.
After exposing the surface of the left kidney completely, gently puncture the renal capsule and make a tiny hole (1 mm) with a pair of fine forceps.
-
7.
Insert an autoclaved micropipette tip with a blunt ball-shaped front (made by melting a normal pipette tip) into the hole to gently separate the renal capsule from the kidney parenchyma in order to make space to contain the fetal tissue.
-
8.
Suck both the human fetal thymus and liver fragments measuring about 1 mm3together into an 18-G blunt head spinal needle attached to a 1 ml syringe.
-
9.
Insert the needle through the hole into the space between the renal capsule and kidney parenchyma.
-
10.
Push the fetal liver and thymus tissues deep inside the renal capsule and slowly remove the needle from the kidney (see Note 10).
-
11.
Allow the bleeding in the surgical area to coagulate and carefully put back replace all the intestines into the abdominal cavity.
-
12.
Clean the muscle and skin and separately suture with absorbable sutures.
-
13.
Administer 40 mg/kg dose of gentamycin (intramuscular) and 0.05 mg/kg dose of buprenorphine (subcutaneous) after the surgery (see Note 11).
-
14.
Keep the animals warm with a temperature-controlled heating pad until the mice regain consciousness.
3.3.4 Intravenous Transfer of CD34+Cells
-
1.
Mice subjected to tissue implantation receive cell preparations that were purified from the same donor on the day of human tissue transplantation.
-
2.
Put mice under a heat lamp to increase blood flow to the tail vein and then transfer to a holding device, which restrains the mouse while allowing access to the tail vein.
-
3.
Inject 0.2 ml cell suspension (1–5 × 105CD34+cells) into the lateral tail vein of recipient mouse (maximum volume 10% body weight) using 1-cc syringe with 27-G needle (see Note 12).
-
4.
Monitor mice daily for signs of distress.
-
5.
Allow human HSCs to engraft in mice for 10–12 weeks.
-
6.
Test human cell engraftment.
3.4 Analysis of Reconstitution
-
1.
Mice should be monitored for engraftment levels of human cells over a 5–15 day period for Hu-PBL mice and 10- to 12-week period for Hu-HSC by multicolor flow cytometric analysis for detection of lineage markers on human hemato-poietic cells in the mouse peripheral blood.
-
2.
Induce anesthesia using isoflurane chamber.
-
3.
Collect whole blood (∼100 μl) from all mice to be tested by retro-orbital bleeding using a heparinized capillary tube.
-
4.
Isolate mononuclear cells by ficoll centrifugation of peripheral blood after lysing red blood cells using red blood cell lysing buffer and resuspend in PBS containing 2% FBS.
-
5.
Add appropriate antibody mix to the cell suspension and incubate for 30 min at 4°C to label the antibody.
-
6.
Wash cells in PBS containing 2% FBS.
-
7.
Resuspend cells in 200 μl of PBS containing 2% FBS for flow cytometric analysis.
-
8.
Collect and analyze flow cytometric data using FACSCanto II and FACSDiva software (Fig. 2).
Fig. 2. 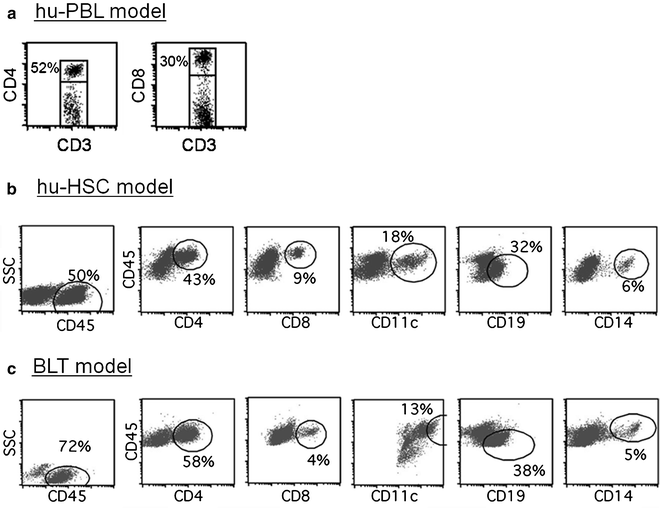
Flow cytometric analysis showing reconstitution efficiencies in (a) Hu-PBL mice and (b) Hu-HSC and (c) BLT mice. Data were obtained 5 days (a) and 12 weeks (band c) after the transplantation.

4 Notes
-
1.
Immunodeficient mice should be housed in a specific pathogen free (SPF) environment, using sterile techniques and in microisolator cages. All the animals are fed with sterile food and water. General health monitoring. Mice should be monitored daily and must be cared for if they show signs of ill health such as hunched posture, inactivity or loss in appetite/dehydration.
-
2.
The use of human hematopoietic stem cells requires appropriate Institutional Review Board (IRB) approval.
-
3.
Most experiments should be done within 4 weeks post-PBMC injection before xenogenic GVHD symptoms develop. If there are signs of GVHD development (weight loss of >15%), animals should be euthanized.
-
4.
This protocol yields greater than 90–95% pure CD34+ cells and less than 1.0% CD3+ T cells. If necessary, depletion of CD3 T cells can be performed using anti-CD3 MACS beads.
-
5.
Human tissues and mice engrafted with human tissues should be considered potential biological hazards and handled with proper personal protective equipment at animal biosafety level 2 (ABSL2), in accordance with governmental and institutional biosafety guidelines.
-
6.
All cell isolation and surgical procedure must use sterile techniques.
-
7.
The sublethal irradiation dose should be adapted based on the irradiator and age of the mouse used. The transfer of mice from the microisolator cages to the sterile autoclaved container should be done in a laminar flow biocontainment hood to minimize exposure of the immunodeficient mice to environmental infectious agents.
-
8.
General anesthesia suppresses the heat-regulating mechanisms of the body. Thus, it is important to maintain body temperature in appropriate thermostatically controlled incubators or by other heat sources during and after operative procedures.
-
9.
Smear sterile ophthalmic ointment onto the eyes to prevent drying during anesthesia.
-
10.
The fetal tissues can be easily seen through the kidney capsule after injection and should remain compact after injection.
-
11.
Buprenorphine is given as an analgesic and additional doses should be given every 6–8 h during the first 48 h following the surgery.
-
12.
Surgical implantation of fetal tissue for the BLT protocol may be performed on the same day as, or up to 72 h following irradiation.
References
Shultz, L. D., Ishikawa, F., and Greiner, D. L. (2007) Humanized mice in translational biomedical research. Nat. Rev. Immunol. 7, 118–130.
Legrand, N., Ploss, A., Balling, R., Becker, P. D., Borsotti, C., Brezillon, N., Debarry, J., de Jong, Y., Deng, H., Di Santo, J. P., Eisenbarth, S., Eynon, E., Flavell, R. A., Guzman, C. A., Huntington, N. D., Kremsdorf, D., Manns, M. P., Manz, M. G., Mention, J. J., Ott, M., Rathinam, C., Rice, C. M., Rongvaux, A., Stevens, S., Spits, H., Strick-Marchand, H., Takizawa, H., van Lent, A. U., Wang, C., Weijer, K., Willinger, T., and Ziegler, P. (2009) Humanized mice for modeling human infectious disease: challenges, progress, and outlook. Cell Host Microbe. 6, 5–9.
Kumar, P., Ban, H. S., Kim, S. S., Wu, H., Pearson, T., Greiner, D. L., Laouar, A., Yao, J., Haridas, V., Habiro, K., Yang, Y. G., Jeong, J. H., Lee, K. Y., Kim, Y. H., Kim, S. W., Peipp, M., Fey, G. H., Manjunath, N., Shultz, L. D., Lee, S. K., and Shankar, P. (2008) T cell-specific siRNA delivery suppresses HIV-1 infection in humanized mice. Cell 134, 577–586.
Denton, P. W., Estes, J. D., Sun, Z., Othieno, F. A., Wei, B. L., Wege, A. K., Powell, D. A., Payne, D., Haase, A. T., and Garcia, J. V. (2008) Antiretroviral pre-exposure prophylaxis prevents vaginal transmission of HIV-1 in humanized BLT mice. PLoS Med. 5, e16.
Hiramatsu, H., Nishikomori, R., Heike, T., Ito, M., Kobayashi, K., Katamura, K., and Nakahata, T. (2003) Complete reconstitution of human lymphocytes from cord blood CD34+ cells using the NOD/SCID/gammacnull mice model. Blood 102, 873–880.
Yahata, T., Ando, K., Nakamura, Y., Ueyama, Y., Shimamura, K., Tamaoki, N., Kato, S., and Hotta, T. (2002) Functional human T lymphocyte development from cord blood CD34+ cells in nonobese diabetic/Shi-scid, IL-2 receptor gamma null mice. J. Immunol. 169, 204–209.
Ishikawa, F., Yasukawa, M., Lyons, B., Yoshida, S., Miyamoto, T., Yoshimoto, G., Watanabe, T., Akashi, K., Shultz, L. D., and Harada, M. (2005) Development of functional human blood and immune systems in NOD/SCID/IL2 receptor {gamma} chain(null) mice. Blood 106, 1565–1573.
Traggiai, E., Chicha, L., Mazzucchelli, L., Bronz, L., Piffaretti, J. C., Lanzavecchia, A., and Manz, M. G. (2004) Development of a human adaptive immune system in cord blood cell-transplanted mice. Science 304, 104–107.
Peer, D., Park, E. J., Morishita, Y., Carman, C. V., and Shimaoka, M. (2008) Systemic leukocyte-directed siRNA delivery revealing cyclin D1 as an anti-inflammatory target. Science 319, 627–630.
Peer, D., Zhu, P., Carman, C. V., Lieberman, J., and Shimaoka, M. (2007) Selective gene silencing in activated leukocytes by targeting siRNAs to the integrin lymphocyte function-associated antigen-1. Proc. Natl. Acad. Sci. USA. 104, 4095–4100.
Lan, P., Tonomura, N., Shimizu, A., Wang, S., and Yang, Y. G. (2006) Reconstitution of a functional human immune system in immunodeficient mice through combined human fetal thymus/liver and CD34+ cell transplantation. Blood 108, 487–492.
McCune, J. M., Namikawa, R., Kaneshima, H., Shultz, L. D., Lieberman, M., and Weissman, I. L. (1988) The SCID-hu mouse: murine model for the analysis of human hematolymphoid differentiation and function. Science 241, 1632–1639.
McCune, J. M. (1997) Animal models of HIV-1 disease. Science 278, 2141–2142.
Brainard, D. M., Seung, E., Frahm, N., Cariappa, A., Bailey, C. C., Hart, W. K., Shin, H. S., Brooks, S. F., Knight, H. L., Eichbaum, Q., Yang, Y. G., Sykes, M., Walker, B. D., Freeman, G. J., Pillai, S., Westmoreland, S. V., Brander, C., Luster, A. D., and Tager, A. M. (2009) Induction of robust cellular and humoral virus-specific adaptive immune responses in human immunodeficiency virus-infected humanized BLT mice. J. Virol. 83, 7305–7321.
Berges, B. K., Akkina, S. R., Folkvord, J. M., Connick, E., and Akkina, R. (2008) Mucosal transmission of R5 and X4 tropic HIV-1 via vaginal and rectal routes in humanized Rag2−/− gammac −/− (RAG-hu) mice. Virology 373, 342–351.
Melkus, M. W., Estes, J. D., Padgett-Thomas, A., Gatlin, J., Denton, P. W., Othieno, F. A., Wege, A. K., Haase, A. T., and Garcia, J. V. (2006) Humanized mice mount specific adaptive and innate immune responses to EBV and TSST-1. Nat. Med. 12, 1316–1322.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer Science+Business Media, LLC
About this protocol
Cite this protocol
Kim, SS., Kumar, P., Ye, C., Shankar, P. (2011). Humanized Mice for Studying Human Leukocyte Integrins In Vivo. In: Shimaoka, M. (eds) Integrin and Cell Adhesion Molecules. Methods in Molecular Biology, vol 757. Humana Press, Totowa, NJ. https://doi.org/10.1007/978-1-61779-166-6_30
Download citation
DOI: https://doi.org/10.1007/978-1-61779-166-6_30
Published:
Publisher Name: Humana Press, Totowa, NJ
Print ISBN: 978-1-61779-165-9
Online ISBN: 978-1-61779-166-6
eBook Packages: Springer Protocols