
Abstract
Antimicrobial resistance (AMR) is a pressing issue in China, with antibiotic therapy becoming less effective against bacterial infections. To address this challenge, the China Antimicrobial Surveillance Network (CHINET) was established in 2005 to monitor antimicrobial resistance in the country. This study analyzed the CHINET data from teaching hospitals and evaluated the trends of AMR in China from 2018 to 2022. A range of 163,636 to 301,917 isolates was obtained per year, with the majority being Gram-negative bacilli (69.0% to 71.8%). The proportion of important multidrug-resistant pathogens remained stable over the years. While the analysis showed diverse AMR profiles for different bacterial species. Over the five years, generally decreased resistance rates were observed from the majority of the tested species. For example, resistance to ceftriaxone decreased in Escherichia coli and Klebsiella pneumoniae, while resistance to imipenem and meropenem decreased in Pseudomonas aeruginosa. Moreover, resistance to methicillin, gentamicin, fosfomycin, and clindamycin also decreased in clinical Staphylococcus aureus isolates. On the other hand, resistance levels of Acinetobacter baumannii remained stable. Our study provides a comprehensive overview of the AMR profiles of common bacterial species in China and highlights the ongoing efforts to address this challenge.
Similar content being viewed by others
Introduction
Antimicrobial resistance surveillance is essential in understanding the antimicrobial susceptibility of pathogenic bacteria and their resistance trends to important antimicrobial drugs. This is crucial for clinical anti-infection empirical management and precise treatment [1, 2]. In 2004, starting with eight hospitals, Huashan Hospital of Fudan University established the China Antimicrobial Surveillance Network (CHINET, www.chinets.com) [3]. Currently, the network has expanded to 71 hospitals across 29 provinces, municipalities and autonomous regions, including 55 tertiary and 16 secondary hospitals (or 51 general and 20 children’s hospitals). The CHINET has established "CHINET Cloud", an online information system for antimicrobial susceptibility testing data, which provides a yearly release of surveillance data [3]. Thus far, the CHINET system has become one of the most influential antimicrobial surveillance networks in China. In 2018, CHINET reported the antimicrobial resistance trends of clinically important bacteria in China from 2005 to 2017 [4, 5]. In this study, we analyzed the antimicrobial susceptibility and resistance trends of clinically Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, Acinetobacter baumannii, and Staphylococcus aureus isolated from 2018–2022. Our study highlights the current resistance trends in the above five target species, demonstrates the importance of bacterial surveillance studies, and plays a critical role in guiding empirical antimicrobial therapy in clinical practice.
Results
Percentage of targeted five bacterial species
The total number of bacterial isolates was 1,232,028, ranging from 163,636 to 301,917 per year (Fig. 1). The distribution of specimen sources for the different bacterial species varied considerably (Fig. 2). The main specimen sources for E. coli were urinary tract (48.0%, n = 112,487), blood (17.3%, n = 40,452) and respiratory tract (9.8%, n = 22,966). K. pneumoniae was mainly isolated from the respiratory tract (51.9%, n = 91,132), blood (16.1%, n = 28,270) and urinary tract (14.1%, n = 24,758). P. aeruginosa was mainly isolated from the respiratory tract (66.3%, n = 68,685), urinary tract (8.5%, n = 8,805) and pus (6.4%, n = 6,630). A. baumannii was mainly isolated from respiratory tract (76.6%, n = 75,414), blood (5.4%, n = 5,316) and urinary tract (4.8%, n = 4,725). S. aureus was mainly isolated from respiratory tract (38.7%, n = 44,059), pus (17.2%, n = 19,582) and blood (12.4%, n = 14,117). The ratio of Gram-negative bacilli and Gram-positive cocci was 69.0%–71.8% and 28.2%–31.0%, respectively (Fig. 1). There were no changes in the ratio between specimen types during the study period. The percentage of the five target species in the total number of all reported isolates is shown in Fig. 1 and Supplementary Appendix Table 1.

Percentages of Gram-negative bacilli, Gram-positive cocci, and targeted five species among total number of all reported isolates

Prevalence of E. coli, K. pneumoniae, P. aeruginosa, A. baumannii, and S. aureus among specimen type
Escherichia coli
The resistance rates of E. coli to most antimicrobial agents decreased over the five years. Specifically, the resistance rate of clinical E. coli isolates to ceftriaxone decreased from 57.5% to 50.8% (Fig. 3). The rate of imipenem-resistant isolates also decreased from 2% in 2018 to 1.5% in 2022 (Fig. 3). Moreover, the resistance rates of E. coli to amikacin, piperacillin-tazobactam, cefoperazone-sulbactam, meropenem, ciprofloxacin and levofloxacin decreased from 2.7% to 2.2%, from 5.3% to 4.3%, from 6.5% to 5.5%, from 2.1% to 1.6%, from 66% to 61.4% and from 58.9% to 53.2%, respectively. Additionally, the resistance rates of E. coli to cefepime, cefoxitin, trimethoprim-sulfamethoxazole, and fosfomycin decreased from 27.3% to 25.1%, 13.5% to 9.7%, 56.2% to 51.8% and 5% to 4.4%, respectively. However, the resistance rates of colistin and tigecycline fluctuated around 1.0% and 0.1%, respectively. Notably, the resistance rate of E. coli to polymyxin B increased from 0.7% in 2018 to 1.0% in 2022 (Fig. 4 and Supplementary Appendix Table 2).

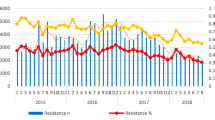
Rates of ceftriaxone-resistant E. coli and K. pneumoniae, imipenem-resistant Gram-negative bacilli, and oxacillin-resistant S. aureus clinical isolates from 2018 to 2022

Resistance profile of E. coli for eight representative antimicrobial agents
Klebsiella pneumoniae
The resistance rate of K. pneumoniae isolates to ceftriaxone decreased from 46.0% to 42.7% during the five-year period (Fig. 3). While K. pneumoniae isolates showed a relatively stable resistance rates to imipenem, meropenem, amikacin, piperacillin-tazobactam, cefepime and tigecycline (Figs. 3 and 5). While the resistance rates to cefoperazone-sulbactam, levofloxacin and trimethoprim-sulfamethoxazole decreased from 33% to 30.9%, from 38% to 35.2% and from 38.2% to 32.9% respectively. However, a significant decrease in resistance was observed for ceftazidime-avibactam and ciprofloxacin, from 9.8% to 4.8% and from 50.2% to 38.3%, respectively. A significant increase in resistance was observed for polymyxin B, from 1.0% to 5.1%. The resistance rate of K. pneumoniae to cefoxitin increased from 25.2% to 27.9%. Colistin and tigecycline resistance rates fluctuated around 2.5% and 4.0%, respectively. (Fig. 5 and Supplementary Appendix Table 3).

Resistance profile of K. pneumoniae for eight representative antimicrobial agents
Pseudomonas aeruginosa
P. aeruginosa resistance decreased for all antimicrobial agents, during the five-year period. The rates of imipenem- and meropenem-resistant isolates decreased from 30.7% to 23.8% and from 25.8% to 19.2%, respectively, during the 5-year sampling period (Fig. 3 and Supplementary Appendix Table 4). Resistance to ceftazidime-avibactam significantly decreased from 11.1% to 6.3%. Furthermore, the resistance rates to cefoperazone-sulbactam, piperacillin-tazobactam, ceftazidime, ciprofloxacin and amikacin decreased from 17.1% to 15%, 16.7% to 13.5%, 19.3% to 14.9%, 24.1% to 15.3%, and 6.2% to 3.8%, respectively. The resistance rates of colistin and polymyxin B fluctuated around 1.5% and 0.5% respectively (Fig. 6 and Supplementary Appendix Table 4).

Resistance profile of P. aeruginosa for eight representative antimicrobial agents
Acinetobacter baumannii
During the five-year period, the resistance levels of A. baumannii isolates to imipenem and meropenem remained relatively stable, decreasing from 78% to 75.6% and from 78.8% to 76.6%, respectively (Fig. 3). Resistance to cefoperazone-sulbactam, amikacin, and levofloxacin increased from 52.5% to 58.7%, 57.8% to 59.2% and 61.5% to 63.1%, respectively. Resistance to ampicillin-sulbactam, piperacillin-tazobactam, ceftazidime, ciprofloxacin, and tigecycline decreased from 72.6% to 68.7%, from 77.9% to 77.4%, from 77.7% to 74.5%, from 79.1% to 75.4% and from 5.1% to 2.5%, respectively. Colistin and polymyxin B resistance rates were fluctuated around 1% and 0.5%, respectively (Fig. 7 and Supplementary Appendix Table 5).

Resistance profile of A. baumannii for six representative antimicrobial agents
Staphylococcus aureus
The prevalence of methicillin resistance in S. aureus isolates decreased from 34.4% in 2018 to 30.5% in 2022 (Fig. 3). Furthermore, a significant reduction in resistance rates was noted for several antibiotics. For instance, the percentage of S. aureus isolates resistant to gentamicin, fosfomycin and clindamycin decreased from 17%, 13%, and 38.9% to 8.4%, 3.4%, and 26.7%, respectively. Similarly, resistance rates to rifampicin, ciprofloxacin, trimethoprim-sulfamethoxazole, and erythromycin decreased from 4.9% to 1.7%, 19.5% to 12.7%, 14.7% to 10.4% and 64.3% to 52.7% respectively. Notably, no isolates were observed resistant to vancomycin and linezolid. On the other hand, resistance rates to teicoplanin and tigecycline remained relatively low, fluctuating around 0.1% and 0.3%, respectively (Fig. 8 and Supplementary Appendix Table 6).

Resistance profile of S. aureus for eight representative antimicrobial agents
Discussion
In summary, the resistance status and trends of most antimicrobials against the five target species were relatively stable. The resistance level of some antimicrobials showed a decreasing trend, but each species still had its characteristic antimicrobial resistance. For E. coli, the resistance trends of all cephalosporins were relatively stable and decreased to some extent. For the third-generation cephalosporins, the resistance rate in China showed a decreasing trend, whereas the resistance rate increased in the EU/EAA in 2001 to 2018, which kept below 15% [6]. The resistance rates of carbapenems, amikacin, polymyxin B, colistin, fosfomycin, and partial β-lactam-β-lactamase inhibitor combinations remained relatively low, the sensitivity of tigecycline was above 99.7%.
Conversely, the overall resistance status of K. pneumoniae was more severe than that of E. coli. The resistance rates of carbapenems have been increasing since the CHINET surveillance data were collected in 2005. According to CHINET data from 2018 to 2022, the resistance rates of carbapenems, including ertapenem, imipenem and meropenem, increased significantly, up to 26.9%, 26% and 27.5%, respectively. Compared with CHINET data from 2005 to 2017 [5], the resistance to carbapenems still grew rapidly. Compared with the resistance status of carbapenems from several global surveillance studies [7, 8], the resistance rates of carbapenems ranged from 3.5% to 8.4% in Latin America, 3.2% to 3.7% in Europe, 1.2% to 1.9% in North America, and some countries had higher proportions of carbapenem-resistant K. pneumoniae > 40%, including India (54.9%), Greece (53.6%), Argentina (46.4%). Therefore, the carbapenem resistance rates in China remained at the hyper-average level in a global context. In addition, only colistin, polymyxin B, ceftazidime-avibactam, and tigecycline maintained relatively high susceptibility to K. pneumoniae. It should be noted that the increasing trends of polymyxin B resistance were observed in both K. pneumoniae (from 1% to 5.1%) and E. coli (from 0.7% to 1%) isolates during 2018–2022. As China approved the use of polymyxin B in clinics in 2017 [9], further surveillance of polymyxin B resistance in both K. pneumoniae and E. coli in Chinese clinics is urgently needed to ensure the prudent use of this last resort antimicrobial agent.
For P. aeruginosa, resistance levels decreased for most antimicrobials. In addition, P. aeruginosa is a common pathogen associated with carbapenem-resistant phenotypes and showed resistance rates of around 20% to 30%. Currently, the Antimicrobial Testing Leadership and Surveillance (ATLAS) programme is investigating resistance patterns of P. aeruginosa in the Asia–Pacific region from 2015 to 2019, and the overall rate of carbapenem-resistant P. aeruginosa was 18.9%, ranging from the lowest in Australia (6.5%) to the highest in India (29.3%) [10]. There is no doubt that the resistance of A. baumannii to most antimicrobials, including carbapenems and β-lactam-β-lactamase inhibitor combinations, remains at high levels. While the proportion of carbapenem resistance in clinical A. baumannii isolates in European countries varied from 10% to 30% in Germany, it was relatively lower than in China ranging from 75.6% to 78.8% [11]. Regarding the prevalence of MRSA in China, the detection rate of MRSA has continuously decreased from 69.0% in 2005 to 30.5% in 2022. Data from EARS-Net showed that the prevalence of MRSA in European countries also showed a significant decreasing trend, from 24.4% in 2005 to 14.1% in 2018 [12].
From the above analysis of the five target bacterial species, the most intuitive change is that antimicrobial resistance showed a decreasing trend for some species. This is a positive confirmation of the work that has been done to address the serious antimicrobial resistance status. Over the past decade, China has established a relatively comprehensive management system and technical support framework for antimicrobial stewardship [13]. Firstly, based on One Health, several guidelines and documents are issued and strictly implemented to regulate the use of antimicrobials in both humans and animals and to strengthen antimicrobial surveillance in the environment. Secondly, antimicrobial resistance surveillance networks, such as CHINET and CARSS, established in China, provide high-quality, comprehensive and real-time surveillance data, which are essential to reducing the burden of antimicrobial resistance [14]. Third, professional staff training and advanced techniques also provide more opportunities to identify unusual resistance phenotypes, genotypes of resistance genes, or other resistance mechanisms, so that precision therapy can be used to reduce the burden of antimicrobial use.
From the above analysis, it can be concluded that the resistance status of clinical isolates in China remains serious. Some important multidrug-resistant bacteria, such as carbapenem-resistant K. pneumoniae, carbapenem-resistant P. aeruginosa and carbapenem-resistant A. baumannii, are widespread in China and have been highlighted as an urgent threat to global public health [15]. As this type of multidrug-resistant bacteria spreads around the world in the absence of alternative drugs, patients are often left without effective treatment, resulting in significant morbidity and mortality. New antibiotics and drug combinations based on antimicrobial susceptibility testing have been developed to address this threat, including ceftazidime-avibactam, meropenem-vaborbactam, cefiderocol, and others [16,17,18].
From the retrospective study of CHINET, we can learn the holistic antimicrobial resistance profile of China. First, CHINET consists of 71 hospitals from 29 provinces, municipalities and autonomous regions covering 960 million people in China. Second, CHINET conducts active surveillance studies and responds to the comprehensive status and trends of antimicrobial resistance in China. Third, hospital-level surveillance of bacterial resistance is needed as part of antimicrobial stewardship activities in China, as local data on antimicrobial resistance are critical to guide the rational use of antimicrobials, such as the empirical use of antimicrobials for hospital-acquired and ventilator-associated pneumonia [19]. The present study still has some limitations, including the short time period, which covered variations in many antimicrobials, and the large fluctuations over time. Finally, there is a need to strengthen the CHINET surveillance system, especially for important drug-resistant pathogens, and to conduct molecular biological studies to clarify the susceptibility of different genotypes of strains to antibacterial agents, especially new antibacterial agents, in order to understand the epidemiological characteristics of important drug-resistant bacteria. With the development of molecular biology techniques, a promising approach that combines the resistant phenotype with the genotype of virulence and resistance genes, which can be an effective strategy to reduce the burden of antimicrobial use.
Conclusion
The antimicrobial resistance status of clinical isolates in China remains stable but serious. Although the isolation rate of MRSA is decreasing, the Gram-negative bacilli have higher antimicrobial resistance profiles, especially ceftriaxone-resistant E. coli, carbapenem-resistant K. pneumoniae, carbapenem-resistant P. aeruginosa and multidrug-resistant A. baumannii. These pose great challenges to antimicrobial chemotherapy in clinics in China. We need to strengthen the CHINET surveillance system and make efforts to curb the rise of antimicrobial resistance.
Materials and methods
Bacterial strains and species identification
All clinical isolates of E. coli, K. pneumoniae, P. aeruginosa, A. baumannii and S. aureus collected from outpatients and inpatients in 71 hospitals were included in CHINET for five years between 2018–2022. To avoid duplicate counts, only one isolate of the same species was included per patient per year based on their personal identification code and hospital. Species identification was performed at each participating site and confirmed by the central laboratory using matrix-assisted laser desorption ionisation-time of flight mass spectrometry (BioMérieux, Marcy I’Etoile, France). E. coli ATCC 25922, P. aeruginosa ATCC 27853 and S. aureus ATCC 29213 were used as quality control strains for antimicrobial susceptibility testing to ensure the reproducibility of the testing procedure.
Antimicrobial susceptibility testing
According to a CHINET uniform protocol, antimicrobial susceptibility testing was performed using automated systems, supplemented by a disc diffusion method for some antimicrobial agents that were not available in automated systems. Quality control and test results were interpreted according to Clinical and Laboratory Standards Institute (CLSI) 2022 breakpoints for all agents tested, except for tigecycline and polymyxin B [20]. Tigecycline minimum inhibitory concentrations (MICs) were interpreted using US Food and Drug Administration (FDA) MIC breakpoints for which CLSI criteria were not available [21]. Colistin and polymyxin B were interpreted using the European Committee on Antimicrobial Susceptibility Testing (EUCAST) MIC interpretive breakpoints for colistin [22]. During the 5-year sampling period, the methods used were consistent in all participating hospitals.
Data analysis
Data were collected in a standardized format from microbiology laboratories and entered into a central database using WHONET software [23]. Statistical analysis and calculations were performed using the WHONET software.
Availability of data and materials
The datasets used or analyzed during the current study are available in CHINET, www.chinets.com.
References
National Health Commission. National action plan to combat antimicrobial resistance (2022–2025). 2022. http://www.nhc.gov.cn/yzygj/s7659/202210/2875ad7e2b2e46a2a672240ed9ee750f.shtml. Accessed 25 Oct 2022.
Ding L, Hu F. China’s new national action plan to combat antimicrobial resistance (2022–25). J Antimicrob Chemother. 2023;78(2):558–60.
China Antimicrobial Surveillance Network. www.chinets.com. Accessed 1 Feb 2023.
Hu FP, Guo Y, Zhu DM, Wang F, Jiang XF, Xu YC, et al. Resistance trends among clinical isolates in China reported from CHINET surveillance of bacterial resistance, 2005–2014. Clin Microbiol Infect. 2016;22(Suppl 1):S9–14.
Hu F, Zhu D, Wang F, Wang M. Current status and trends of antibacterial resistance in China. Clin Infect Dis. 2018;67(suppl_2):S128–34.
Peñalva G, Högberg LD, Weist K, Vlahović-Palčevski V, Heuer O, Monnet DL. Decreasing and stabilising trends of antimicrobial consumption and resistance in and in segmented regression analysis, European Union/European Economic Area, 2001 to 2018. Euro Surveill. 2019;24(46):1900656.
Lee Y-L, Ko W-C, Hsueh P-R. Geographic patterns of global isolates of carbapenem-resistant Klebsiella pneumoniae and the activity of ceftazidime/avibactam, meropenem/vaborbactam, and comparators against these isolates: results from the antimicrobial testing leadership and surveillance (ATLAS) program, 2020. Int J Antimicrob Agents. 2022;60(5–6):106679.
Kazmierczak KM, Karlowsky JA, de Jonge BLM, Stone GG, Sahm DF. Epidemiology of carbapenem resistance determinants identified in meropenem-nonsusceptible collected as part of a global surveillance program, 2012 to 2017. Antimicrob Agents Chemother. 2021;65(7):e0200020.
Zhang R, Shen Y, Walsh TR, Wang Y, Hu F. Use of polymyxins in Chinese hospitals. Lancet Infect Dis. 2020;20(10):1125–6.
Lee Y-L, Ko W-C, Hsueh P-R. Geographic patterns of carbapenem-resistant Pseudomonas aeruginosa in the Asia-Pacific region: results from the antimicrobial testing leadership and surveillance (ATLAS) program, 2015–2019. Antimicrob Agents Chemother. 2022;66(2):e0200021.
Wohlfarth E, Kresken M, Higgins PG, Stefanik D, Wille J, Hafner D, et al. The evolution of carbapenem resistance determinants and major epidemiological lineages among carbapenem-resistant Acinetobacter baumannii isolates in Germany, 2010–2019. Int J Antimicrob Agents. 2022;60(5–6):106689.
Gagliotti C, Högberg LD, Billström H, Eckmanns T, Giske CG, Heuer OE, et al. Staphylococcus aureus bloodstream infections: diverging trends of meticillin-resistant and meticillin-susceptible isolates, EU/EEA, 2005 to 2018. Euro Surveill. 2021;26(46):2002094.
Xiao Y. Antimicrobial stewardship in China: systems, actions and future strategies. Clin Infect Dis. 2018;67(suppl_2):S135–41.
Tacconelli E, Sifakis F, Harbarth S, Schrijver R, van Mourik M, Voss A, et al. Surveillance for control of antimicrobial resistance. Lancet Infect Dis. 2018;18(3):e99–106.
Grundmann H, Glasner C, Albiger B, Aanensen DM, Tomlinson CT, Andrasević AT, et al. Occurrence of carbapenemase-producing Klebsiella pneumoniae and Escherichia coli in the European survey of carbapenemase-producing Enterobacteriaceae (EuSCAPE): a prospective, multinational study. Lancet Infect Dis. 2017;17(2):153–63.
Kanj SS, Bassetti M, Kiratisin P, Rodrigues C, Villegas MV, Yu Y, et al. Clinical data from studies involving novel antibiotics to treat multidrug-resistant Gram-negative bacterial infections. Int J Antimicrob Agents. 2022;60(3):106633.
Zhanel GG, Golden AR, Zelenitsky S, Wiebe K, Lawrence CK, Adam HJ, et al. Cefiderocol: a siderophore cephalosporin with activity against carbapenem-resistant and multidrug-resistant Gram-negative bacilli. Drugs. 2019;79(3):271–89.
Yahav D, Giske CG, Grāmatniece A, Abodakpi H, Tam VH, Leibovici L. New β-Lactam-β-Lactamase inhibitor combinations. Clin Microbiol Rev. 2020;34(1):e00115–20
Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, et al. Management of adults with hospital-acquired and ventilator-associated Pneumonia: 2016 clinical practice guidelines by the infectious diseases society of America and the American thoracic society. Clin Infect Dis. 2016;63(5):e61–111.
Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. CLSI supplement M100. 32th ed. Wayne(PA): Clinical and Laboratory Standards Institute; 2022.
Food and Drug Administration. Tigecycline-injection products. 2019. https://www.fda.gov/drugs/development-resources/tigecycline-injection-products. Accessed 26 Jan 2023.
The European Committee on Antimicrobial Susceptibility Testing (EUCAST). Clinical breakpoints tables for interpretation of MICs and zone diameters. Version 12.0. 2022. https://eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_12.0_Breakpoint_Tables.pdf. Accessed 1 Jan 2022.
WHO Collaborating Centre for Surveillance of Antimicrobial Resistance. The microbiology laboratory database software. 2022. https://whonet.org/software.html. Accessed 18 Jul 2022.
Acknowledgements
We would like to express our thanks to members of CHINET for their contribution in the collection of the isolates in this study, including the following: Yingchun Xu and Xiaojiang Zhang from Peking Union Medical College Hospital; Zhaoxia Zhang and Ping Ji from the First Affiliated Hospital of Xinjiang Medical University; Mei Kang and Chao He from West China Hospital, Sichuan University; Chuanqing Wang and Pan Fu from Children’s Hospital of Fudan University; Yuanhong Xu and Ying Huang from the First Affiliated Hospital of Anhui Medical University; Zhongju Chen and Ziyong Sun from Tongji Hospital, Tongji Medical College, Huazhong University of Science & Technology; Yuxing Ni and Jingyong Sun from Ruijin Hospital, Shanghai Jiaotong University School of Medicine; Yunzhuo Chu and Sufei Tian from the First Affiliated Hospital of China Medical University; Zhidong Hu and Jin Li from Tianjin Medical University General Hospital; Yunsong Yu and Jie Lin from Sir Run Run Shaw Hospital, Zhejiang University School of Medicine; Bin Shan and Yan Du from the First Affiliated Hospital of Kunming Medical University; Sufang Guo and Yanyan Wang from the First Affiliated Hospital of Inner Mongolia Medical University; Lianhua Wei and Xin Wang from Gansu Provincial Hospital; Hong Zhang and Chun Wang from Children’s Hospital of Shanghai; Yunjian Hu and Xiaoman Ai from Beijing Hospital; Chao Zhuo and Danhong Su from the First Affiliated Hospital of Guangzhou Medical University; Ruizhong Wang and Hua Fang from Pudong New Area People’s Hospital; Bixia Yu from Zhejiang Ningbo Zhenhai Longsai Hospital; Ping Gong and Miao Song from the People’s Hospital of Zigui, Hubei Province; Dawen Guo and Jinying Zhao from the First Affiliated Hospital of Harbin Medical University; Wen’en Liu and Yanming Li from Xiangya Hospital, Central South University; Yan Jin and Yueling Wang from Shandong Provincial Hospital; Kaizhen Weng and Yirong Zhang from Jinjiang Municipal Hospital; Xuesong Xu and Chao Yan from China-Japan Union Hospital, Jilin University; Xiangning Huang and Hua Yu from Sichuan Provincial People’s Hospital; Yi Li and Shanmei Wang from Henan Provincial People’s Hospital; Lixia Zhang and Juan Ma from Shaanxi Provincial People’s Hospital; Shuping Zhou and Jiangwei Ke from Jiangxi Provincial Children’s Hospital; Lei Zhu and Jinhua Meng from Children’s Hospital of Shanxi; Han Shen and Wanqing Zhou from Nanjing Drum Tower Hospital, Affiliated Hospital of Nanjing; Gang Li and Wei Jia from General Hospital of Ningxia Medical University; Jinsong Wu and Yuemei Lu from Shenzhen People’s Hospital; Jihong Li from the Second Hospital of Hebei Medical University; Jiangshan Liu from Jinchang Hospital of Integrated Traditional Chinese and Western Medicine; Longfeng Liao from the People’s Hospital of Ganxian; Hongqin Gu from Guangrao County People’s Hospital; Lin Jiang from the People’s Hospital of Huixian, Henan Province; Wen He from Central Hospital of Yingkou Development Zone, Liaoning Province; Shunhong Xue from Huzhu County People’s Hospital, Qinghai Province; Jiao Feng from the People’s Hospital of Linshui, Sichuan Province; Rui Dou from Lixin County People’s Hospital; Chunlei Yue from Jiutai People’s Hospital; Ruyi Guo and Yan Jin from Quanzhou First Hospital, Fujian; Xiaobo Ma and Yanping Zheng from The First Affiliated Hospital of Xiamen University; Fangfang Hu from Guizhou Provincial People’s Hospital; and Yunsheng Chen and Qing Meng from Shenzhen Children’s Hospital; Yun Xia and Shan Sun from The First Affiliated Hospital of Chongqing Medical University.
Funding
This work was funded by the National Key Research and Development Program of China (2021YFC2701800 and 2021YFC2701803), the National Natural Science Foundation of China (grant no. 81861138052), the China Antimicrobial Surveillance Network (independent medical grants from Pfizer, 2018QD100), and the Shanghai Antimicrobial Surveillance Network (3030231003). The funders had no role in study design, data collection, analysis, decision to publish, or manuscript preparation.
Author information
Authors and Affiliations
Consortia
Contributions
F.H., Y.G. and D.Z. designed the study. W.Y., L.D., S.W., R.H., D.Y., and Y.Y. performed the experiments and wrote the manuscript. All authors contributed to the article and approved the submitted version.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board of Huashan Hospital, Fudan University (no. 2019–460).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author order was determined by the corresponding author after negotiation.
Supplementary Information
Additional file 1: Table 1.
Percentages of targeted 5 species among total number of all reported isolates. Table 2. Resistance rates and susceptibility rates of E. coli to antimicrobial agents. Table 3. Resistance rates and susceptibility rates of K. pneumoniae to antimicrobial agents. Table 4. Resistance rates and susceptibility rates of P. aeruginosa to antimicrobial agents. Table 5. Resistance rates and susceptibility rates of A. baumannii to antimicrobial agents. Table 6. Resistance rates and susceptibility rates of S. aureus to antimicrobial agents.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yang, W., Ding, L., Han, R. et al. Current status and trends of antimicrobial resistance among clinical isolates in China: a retrospective study of CHINET from 2018 to 2022. One Health Adv. 1, 8 (2023). https://doi.org/10.1186/s44280-023-00009-9
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s44280-023-00009-9