
Abstract
Background
End stage renal disease (ESRD) is emerging as a major health issues across developing countries with limited access and awareness about the importance of exercises in daily life. People on prolong hemodialysis has difficulty in performing their activities of daily living (ADL). Loss of muscle mass is inevitable among patients on hemodialysis that leads to morbidity and mortality. Exercise is feasible during dialysis and can enhance quality of life. Increase in aerobic endurance by various combined protocol of aerobic and resistive exercises can improve compliance to regular exercise that underlines the theme of present study.
Methods
A total of 31 participants were recruited during November 2019 to February 2020, after screening of 65 participants for selection criteria from Indraprastha Apollo Hospital’s dialysis unit. The average age of the participants was 52.36 ± 11.56 years. A single-blinded, pre-test–post-test quasi-experimental clinical trial for intradialytic exercise program involving lower limb ergometer and resistance training for lower limbs and non-fistula hand for 24 sessions, in 3 months, twice a week was conducted.
Results
The exercise program was well tolerated and all patients completed it. Aerobic and resistance intradialytic exercises (IDE) had a positive effect on maximal oxygen consumption (VO2 Max), quality of life (SF 36), and sleep quality (PSQI). IDE showed statistically significant difference from pre- to post-intervention for maximal oxygen consumption, quality of life boosting their sleep quality.
Conclusions
IDE found to benefit the patient and results showed a significant improvement in maximal oxygen consumption, sleep quality, quality of life and fatigue over a span of 12 weeks.
Trial registration
CTRI, CTRI/2019/08/020848. Registered on 22 August 2019.
Similar content being viewed by others


Introduction
Physical inactivity in end stage renal disease (ESRD) can lead to extensive deterioration of physical performance and high risk of cardiovascular disease [1]. An Indian population-based study determined the crude and age-adjusted ESRD incidence rates at 151 and 232 per million populations, respectively [2, 3]. It is estimated that there are about 175,000 patients on chronic dialysis in India, with a prevalence of 129 per million populations [4]. Anxiety, depression and sleep deprivation is common among dialysis patients. Therefore, it is important to balance emotional and physical well-being to maintain them towards their healthy counterparts [5]. Aerobic exercises and strengthening of extremity has reported reduction of physiological deterioration of hemodialysis (HD) and quality of life in comparison to same age and gender [6,7,8,9]. Lower limb ergometer during dialysis helps in improving the urea clearance by enhancing vascular beds in the lower limb muscles and exposing more tissue which allows the fluid in tissue to move into the vascular compartment. It also proves to be safe during the first two hours of dialysis and showed that the practice of physical activity with cycle ergometer increases oxygen consumption, potency, quadriceps resistance time, and strength and improves fatigability [10, 11]
Literature reviewed, indicated that aerobic exercise capacity and peripheral muscular strength had 40–50% reduction compared to same age and gender [12] which resulted from metabolic disorders and physiological deterioration of HD [13]. Then, cardiorespiratory capacity and muscle functionality declined and reflected in the reduction of physical fitness that is a risk factor of poor renal prognosis and poor quality of life (QOL) [14, 15].
During dialysis, patients are considered a somewhat “captive audience,” given they have little else to do during their treatment. The clinic staff is also available to help implement the program. This should lead to higher exercise compliance and less patient burden. However, there is little empirical evidence to support this, as exercise programs are found in less than 10% of HD clinics worldwide, and enrolment and adherence in these are generally low [16, 17]). There are also many inherent disadvantages associated with exercising while confined to a chair or bed. In particular, the intensity and variety of activities that can be performed during dialysis are limited, with the most practical being cycling and lower-body resistance training. There are also concerns that intradialytic exercise may exacerbate hemodynamic instability and other issues that are common during treatment, including intradialytic hypertension, hypotension, cramping, and fatigue, though there is little evidence for this [18]. Moreover, since dialysis is a catabolic process, there is a theoretical risk that the increased energy expenditure associated with intradialytic exercise could exacerbate muscle protein breakdown [19], though this has not been directly tested.
In human beings, sleep is a physical need for maintaining physical-mental health. A poor quality of sleep can negatively affect personal emotions, cognitive processes, motivations, and the ability to focus, leading to loss of appetite, anxiety, nervousness, and depression [20,21,22]. Sleep disorders disrupt normal sleep cycle and create dissipated sleep patterns, leading to an inadequate sleep quantity and quality, daytime malfunctioning, fatigue, and insomnia [21]. Restless leg syndrome is one of the subjective complaints in patients under HD. Patients often describe an irritating sensation in the muscle of the lower legs, which relieves by moving their legs and feet. The restless leg syndrome also contributes to psychiatric symptoms, confusion, anemia and iron, calcium, and phosphorus deficiencies, which is associated with increased mortality in patients undergoing HD. Apnoea is defined as the cessation of respiration for at least 10 s, which is observed in 30–60% of patients undergoing dialysis, and in 2–4% of the general population [23]. As the size of the neck base increases in patients with chronic kidney complications, there will be an increase in the sleep apnoea syndrome [24]. With the premise of the above mentioned understanding about the clinical symptomatology associated with ESRD patient on dialysis, the present research work is a modest attempt to assess and evaluate the effect of intradialytic exercises (IDE) on maximal oxygen consumption, sleep quality, quality of life and fatigue undergoing hemodialysis
Materials and methods
The present study is a single-blinded, pre-test post-test quasi-experimental design, and clinical trial was approved by the Institutional ethics committee-clinical studies (Reg no.: ECR/5/Inst/DL/2013/RR-16) Indraprastha Apollo Hospitals, New Delhi. This study has been registered in the clinical trial Registry-India. Trial registration: CTRI, CTRI/2019/08/020848. Registered on 22 August 2019, http://ctri.nic.in/Clinicaltrials/rmaindet.php?trialid=32760&EncHid=16973.21266&modid=1&compid=19). The study was performed in accordance with the guidelines of Helsinki (2013) and National guidelines for biomedical and health research involving human participants (2017).
Participants
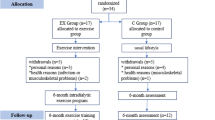
Participants gave written informed consent before data collection began. In this clinical trial presentation, Transparent Reporting of Evaluations with Nonrandomized Designs (TREND) guidelines were used as shown in Fig. 1. A total of 31 participants were recruited during November 2019 to February 2020, after screening of 65 participants for selection criteria.

Flow chart of the Transparent Reporting of Evaluations with Nonrandomized Designs (TREND)
After receiving an information sheet about the study, patients were screened by physiotherapist and excluded if they had acute infectious or other inflammatory illnesses, congestive heart failure, lung failure, severe liver disease, or active cancer except basal cell carcinoma, myocardial infarction or angina pectoris within the past 12 months, disapproval by physician, pregnancy, kidney transplant within 6 months, visual or hearing impairment, inability to give informed consent, and patient having femoral fistula as access for HD.
Procedure and purpose was explained to each individual prior to study.
Participants gave written informed consent before data collection began. The same evaluator, equipment, and procedure were used for all study participants. Each participant was given the opportunity to familiarize themselves with the equipment through the use of a visual demonstration. Detailed history and vitals were monitored pre- and post-session. (BP, HR, Temperature, SpO2, respiratory rate). All biochemical hematological and physiological parameters from patient’s record were also obtained and collected. Pre-assessment of all participants was taken in dialysis department where they were undergoing hemodialysis. All participants were asked to perform a 6-minute walk test (6-MWT) pre-dialysis and scales (PSQI, SF-36, RPE) were filled.
Six-minute walk test
It was conducted in accordance to ATS guidelines 2002 in the dialysis department. Thirty-meter lap distance was taken in hallway, with marking at every 3 m and cones were put at the turn around points. Two chairs were kept on either end. Patient was informed regarding the procedure as instruction to walk at his/her comfortable pace for 6 min around the cones, in case of difficulty can rest/ sit and resume walking as soon as they recover. Patient was made to sit for 10 min, SpO2, pulse rate and fatigue (Borg scale) was measured before commencing the test. Set the lap counter at 0 and timer at 6 min and start. No other command was given except information on remaining time at every passing minute. After completion of 6 min, patient was made to sit and post-SpO2, pulse rate, and fatigue were measured [25].
The outcomes measures were maximal oxygen consumption–VO2 max, Pittsburgh Sleep Quality Index (PSQI), rating of perceived exertion (RPE), and Quality of life-SF-36.
VO2max–Maximal oxygen consumption or VO2max is the gold standard to determine level of aerobic endurance and cardiorespiratory fitness. It is the measure to define the maximum amount of oxygen utilized by muscles of an individual during intense or maximal exercise [26].
VO2max (mL kg (− 1)·min(− 1)) = 70.161 + (0.023 × 6MWT [m]) − (0.276 × weight [kg]) (6.79 × sex, where m = 0, f = 1) − (0.193 × resting HR [beats per minute]) − (0.191 × age [y])
Sleep quality
The Pittsburgh Sleep Quality Index (PSQI) is a subjective measure of sleep quality and patterns. It covers seven areas of sleep problem having 18 questions [27].
Fatigue
Fatigue is an important symptom to patients with advanced chronic kidney disease (CKD). To measure exertional fatigue rate of perceived exertion (RPE) 6–20 scale has been used [28].
Quality of life
End stage renal failure, a chronic disease imposes limitations almost in all domains of quality of life impacting negatively on patient’s health due to accompanied impairments. SF36 is a predictive indicator of assessing effectiveness of treatment to measure health-related quality of life [29].
Progressive resistance training consist of 2 sets of supervised training of 8–10 repetitions. Repetition maximum (RM) was used to guide the intensity of exercise. RM is defined as the most weight one can lift for a defined number of exercise movements. All subject performed a combined exercise training protocol, where aerobic exercise was divided into 3 stages: warm-up, conditioning, and cool down. Resistance training was composed of a total of 10 exercises. Lower extremity strengthening with weighted ankle cuffs, or use of the Thera-band stretch strap, upper extremity strengthening with progressive resistance training (PRT) with free-weight dumbbells. Resistance exercise was lower extremity strengthening-supine hip flexion, supine hip abduction, supine straight-legged raise (up to 30°), hip knee flexion, and bilateral straight-leg raises in a supine position for abdominal strengthening. Upper extremity strengthening-shoulder press, side shoulder raise, triceps extension, biceps curl, and shoulder external rotation for upper extremity strengthening.
Precautions were taken for arm with AV fistula, and it remained stationary during exercises and exercise program was not performed on the arm of fistula during dialysis.
The intradialytic exercise protocol (Table 1) was performed on a lower limb ergometer, where exercise intensity was controlled by the participant’s rate of perceived exertion, through Borg scale (moderate levels, slightly tiring). Cycle ergometer was used for aerobic exercise (Wakeman Portable Folding Fitness Pedal Stationary under Desk Indoor Exercise Bike Arms, Legs, Physical Therapy Calorie Counter). Exercise program was designed on different exercise frequencies, intensities, and duration. When aerobic exercise was planned, heart rate reserve (HRR) or rating of perceived exertion (RPE) was considered to tailor exercise intensity in individual patients.
HRR was calculated by a modification of the Karvonen method:
Statistical analysis
Statistical analysis was performed by using IBM SPSS Statistical Software version 24. Continuous variable were represented using mean and standard deviation. Within Group Analysis was done using Repeated measure ANOVA to study the differences from baseline to post-4th, 8th, and 12th week of intervention. Multiple pairwise comparison was done to analyze the significant difference between the different intervals of pre- to post-intervention. Level of statistical significance was taken as p < 0.05.
Results
Subjective details
Between November 2019 to February 2020, 65 participants were screened. Out of the 65 screened participants, 31 were recruited for the study. The results presented here are of a pilot study done before the commencement of the main trial. The mean age of the participants was 51 + 10.92 years. About 17 participants were females and 14 were males.
Effect of intervention on VO2, PSQI, and RPE pre- to post-intervention
The VO2, PSQI and RPE showed statistically significant improvement (P < 0.001) from baseline to 12 weeks post-intervention as mentioned in Table 2. The variables found to be statistically significant (p < 0.001) when compared between different intervals (baseline, post-4 weeks intervention, post-8 weeks intervention and post-12 weeks intervention) on pairwise comparison as showed in Table 3.
Effect of intervention on quality of life
The secondary outcomes mean estimates that favored the study intervention shows that significant improvement from week 0 to 12, in all parameters of quality of life. The eight domains of SF36 quality of life scale showed statistically significant (p < 0.001) result when compared baseline to 12 weeks post-intervention as mentioned in Table 4. The eight domains of SF-36 found to be statistically significant (p <0.001) when compared between different intervals (baseline, post-4 weeks intervention, post-8 weeks intervention, and post-12 weeks intervention) on pairwise comparison except emotional well-being, pain, and general health that are not statistically significant when compared between baseline and post-4 weeks intervention as showed in Tables 4 and 5
Discussion
The present study examined the effectiveness of intradialytic exercises on maximal oxygen consumption, sleep, quality of life, and fatigue among the patients undergoing the study. The baseline level of functional capacity of our patients undergoing hemodialysis was markedly impaired, limiting their activities of daily living reflecting on their sleep and quality of life. Physical activity in hemodialysis patients is very less in comparison to healthy sedentary individuals and they are less driven towards exercises. Physical activity results in better pulmonary, physical function, and well-being [30]. The within group (pre- to post-intervention) comparison of VO2 max, quality of life, sleep questionnaire, and rate of perceived exertion showed significant difference. The result of the present study is in accordance with the findings of Wu et al. (2014) that showed significant improvement in the aerobic capacity and HRQOL of patients within a short time period with exercise during hemodialysis [31].
Issues in HD patients is inflammation, which is indicated by elevated C-reactive protein (CRP) and other inflammatory markers, and can be used as a predictor of forthcoming cardiovascular morbidity and mortality. Exercise is also crucial for retaining physical independence. Exercises have shown to have various positive effects on HD patients. Some of the important benefits linked to exercise include an improvement in physical fitness, aerobic capacity, dialysis adequacy (measured as urea Kt/V), quality of life, and reduced depressive symptoms [6, 32,33,34,35].
In the present study, all the ESRD enrolled patients showed remarkable improvement in maximal oxygen consumption, highlighting the beneficial effect of both aerobic and strengthening components of exercise. These findings match those of a recent meta-analysis, which showed that both aerobic and combined training significantly improved VO2max [36].
Each hemodialysis treatment in ESRD patients has a catabolic effect on their muscles altering muscle hemostasis leading to secondary sarcopenia with decreased muscle capacity and fatigability impacting quality of life [37]. Hemodialysis patients have skeletal muscle dysfunction due to anemia, malnutrition, uremic myopathy, acidosis, uremic neuropathy, and impaired oxidative capacity and capillarity in all muscle fiber types. In the present study, therefore, resistance training was performed in both lower limbs and in the contralateral upper limb to arteriovenous fistula. Considering some complications of arteriovenous fistulas, such as infection, aneurysm, stenosis, thrombosis, and ischemic polyneuropathy, the hemodialysis patients were advised to protect their fistula arm [38]. The improvement in muscle capacity was accompanied by better quality of life. Studies also suggest that exercise during dialysis helps in improving efficiency of dialysis. Increased blood flow promoted by the exercise is associated with the elimination of toxins during hemodialysis.
Quality of life depends on dialysis efficacy and literature review shows that there are many factors that influence dialysis efficacy like the type of dialyzer machine, dialyzer membrane, the frequency of dialysis, duration of dialysis, and physiological variations among patients. The present study examined the effectiveness of intradialytic exercise in every domain of QOL and our study results reveal that a significant difference in the quality of life when measured pre- to post-intervention. The findings are consistent with the findings of Wu et al (2014) which showed exercise during maintenance HD significantly improved the exercise capacity and HRQOL for uremic patients within a short time period [31]. Furthermore, the findings substantiated the result of the study done by Shemy et al. (2016) that showed significant difference and improvement in studied patients of all domains of QOL scores, and also strong statistically significant positive correlations in all domains of SF-36 [39].
Johansen (2007) had reported that aerobic exercises improves peak oxygen consumption (VO2peak) in ESRD patients and showed that there was about 17% improvement in VO2peak through aerobic exercise lasting from 8 weeks to 6 months in patients with ESRD [40]. In addition, study reported that 9 weeks of leg-cycling during HD improves not only cardiopulmonary fitness and endurance but also muscle strength, power, fatigability, and physical function [41]. Afshar et al. (2010) in their study reported exercises improve perfusion and enhance blood circulation and toxin elimination, improved muscle strength, lowering level of fatigue and impotence expecting improvement in QOL of patients undergoing HD [42]. Zhao et al. (2017) reported mood disorder specially depression score and anxiety negatively impact treatment in ESRD, medicines prescribed might have many physical and emotional undesirable effects and his recent meta-analysis in 2019 confirmed that exercise intervention are best non pharmacological treatment for reducing depression score in renal patients [43]. In the present study also, we found improvement in quality of life after intradialytic exercises in hemodialytic patient. In quality of life SF 36 emotional component, emotional wellbeing did not show significant improvement in initial 4 weeks as HD patients could not believe that exercises could make a difference but with regular regimen they could feel improvement and showed significant improvements in further weeks. Similarly, the pain in the physical component initially did not have significant change in 4 weeks as muscle soreness was felt by patients with minimal activity with commencement of exercises. In general health domain the study showed plateau after 8 weeks and did not report significant difference from post-intervention 8 weeks to post-intervention 12 weeks as ceiling effect had been achieved. This specific domain wise analysis of quality of life as well as to document pre- to post-changes after administering the IDE protocol makes the present study unique and different from the studies previously done that have just reported the quality of life of ESRD patient [44, 45]. However, the study had limited number of the subjects which can be taken up further to explore future scope with a larger size.
Conclusion
Conclusively, IDE found to benefit the patient and results showed a significant improvement in maximal oxygen consumption, sleep quality, Quality of life and fatigue over a span of 12 weeks. Furthermore, the future research specifically utilizing randomized controlled trials, longitudinal trials and comparative studies of aerobic and strength training are desirable.
Availability of data and materials
The findings and data of the study are available with the corresponding author upon reasonable request.
References
Broers NJ, Martens RJ, Cornelis T, van der Sande FM, Diederen NM, Hermans MM, et al. Physical activity in end-stage renal disease patients: the effects of starting dialysis in the first 6 months after the transition period. Nephron. 2017;137(1):47–56.
Modi GK, Jha V. The incidence of end-stage renal disease in India: a population-based study. Kidney Int. 2006;70(12):2131–3.
Varughese S, Abraham G. Chronic kidney disease in India: a clarion call for change. Clin J Am Soc Nephrol. 2018;13(5):802–4.
Jha V, Ur-Rashid H, Agarwal SK, Akhtar SF, Kafle RK, Sheriff R. The state of nephrology in South Asia. Kidney Int. 2019;95(1):31–7.
Salhab N, Karavetian M, Kooman J, Fiaccadori E, El Khoury CF. Effects of intradialytic aerobic exercise on hemodialysis patients: a systematic review and meta-analysis. J Nephrol. 2019;1:1–8.
Sheng K, Zhang P, Chen L, Cheng J, Wu C, Chen J. Intradialytic exercise in hemodialysis patients: a systematic review and meta-analysis. Am J Nephrol. 2014;40(5):478–90.
Chan D, Cheema BS. Progressive resistance training in end-stage renal disease: systematic review. Am J Nephrol. 2016;44(1):32–45.
Young HM, March DS, Graham-Brown MP, Jones AW, Curtis F, Grantham CS, et al. Effects of intradialytic cycling exercise on exercise capacity, quality of life, physical function and cardiovascular measures in adult haemodialysis patients: a systematic review and meta-analysis. Nephrol Dial Transplant. 2018;33(8):1436–45.
Clarkson MJ, Bennett PN, Fraser SF, Warmington SA. Exercise interventions for improving objective physical function in patients with end-stage kidney disease on dialysis: a systematic review and meta-analysis. Am J Physiol Renal Physiol. 2019;316(5):F856–72.
Segura-Ortí E. Exercise in hemodialysis patients: systematic review of the literature. Nephrology (Madrid). 2010;30(2):236–46.
Heiwe S, Jacobson SH. Exercise training in adults with CKD: a systematic review and meta-analysis. Am J Kidney Dis. 2014;64(3):383–93.
Anding K, Bär T, Trojniak-Hennig J, Kuchinke S, Krause R, Rost JM, et al. A structured exercise programme during haemodialysis for patients with chronic kidney disease: clinical benefit and long-term adherence. BMJ open. 2015;5(8):e008709.
Johansen KL, Doyle J, Sakkas GK, Kent-Braun JA. Neural and metabolic mechanisms of excessive muscle fatigue in maintenance hemodialysis patients. Am J Physiol Regulat Integrative Comp Physiol. 2005;289(3):R805–13.
Barcellos FC, Santos IS, Umpierre D, Bohlke M, Hallal PC. Effects of exercise in the whole spectrum of chronic kidney disease: a systematic review. Clin Kidney J. 2015;8(6):753–65.
Roshanravan B, Gamboa J, Wilund K. Exercise and CKD: skeletal muscle dysfunction and practical application of exercise to prevent and treat physical impairments in CKD. Am J Kidney Dis. 2017;69(6):837–52.
Tentori F, Elder SJ, Thumma J, Pisoni RL, Bommer J, Fissell RB, et al. Physical exercise among participants in the Dialysis Outcomes and Practice Patterns Study (DOPPS): correlates and associated outcomes. Nephrol Dial Transplant. 2010;25(9):3050–62.
Ma S, Lui J, Brooks D, Parsons TL. The availability of exercise rehabilitation programs in hemodialysis centres in Ontario. CANNT Journal. 2012;22(4):26–32.
Wilund KR, Jeong JH, Greenwood SA. Addressing myths about exercise in hemodialysis patients. Semin Dial. 2019;32(4):297–302.
McKenna CF, Salvador AF, Hendriks FK, Harris AP, Van Loon LJ, Burd NA. Exercising to offset muscle mass loss in hemodialysis patients: the disconnect between intention and intervention. Sem Dial. 2019;32(4):379–85.
Merlino G, Piani A, Dolso P, Adorati M, Cancelli I, Valente M, et al. Sleep disorders in patients with end-stage renal disease undergoing dialysis therapy. Nephrol Dial Transplant. 2006;21(1):184–90.
Novak M, Shapiro CM, Mendelssohn D, Mucsi I. Reviews: Diagnosis and management of insomnia in dialysis patients. In Seminars in dialysis 2006 19, 1, 25-31). Malden: Blackwell Science Inc.
Tel H, Tel H, Esmek M. Quality of sleep in hemodialysis patients. Dial Transplant. 2007;36(9):479–84.
Čengić B, Resić H, Spasovski G, Avdić E, Alajbegović A. Quality of sleep in patients undergoing hemodialysis. Int Urol Nephrol. 2012;44(2):557–67.
Elias RM, Bradley TD, Kasai T, Motwani SS, Chan CT. Rostral overnight fluid shift in end-stage renal disease: relationship with obstructive sleep apnea. Nephrol Dial Transplant. 2012;27(4):1569–73.
Brooks D, Solway S, Gibbons WJ. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–7.
Burr JF, Bredin SS, Faktor MD, Warburton DE. The 6-minute walk test as a predictor of objectively measured aerobic fitness in healthy working-aged adults. Physician Sports Med. 2011;39(2):133–9.
Mehrabi S, Sarikhani S, Roozbeh J. Sleep quality in patients undergoing long-term hemodialysis using the Pittsburgh sleep quality index. Nephro Urol Monthly. 2017;9(2):e13137.
Macdonald JH, Fearn L, Jibani M, Marcora SM. Exertional fatigue in patients with CKD. Am J Kidney Dis. 2012;60(6):930–9.
Gerasimoula K, Lefkothea L, Maria L, Victoria A, Paraskevi T, Maria P. Quality of life in hemodialysis patients. Materia Socio Medica. 2015;27(5):305.
Fang HY, Burrows BT, King AC, Wilund KR. Microcirculation: Physiology, Pathophysiology, and Clinical Application. Blood Purification. 2020;49(1-2):151–7.
Wu Y, He Q, Yin X, He Q, Cao S, Ying G. Effect of individualized exercise during maintenance haemodialysis on exercise capacity and health-related quality of life in patients with uraemia. J Int Med Res. 2014;42(3):718–27.
Heidari B. C-reactive protein and other markers of inflammation in hemodialysis patients. Caspian J Internal Med. 2013;4(1):611.
Smart N, McFarlane J, Cornelissen VAV. The effect of exercise therapy on physical function, biochemistry and dialysis adequacy in haemodialysis patients: a systematic review and meta-analysis. Open J Nephrol. 2013;3(1):25–36.
Kang SH, Do JY, Jeong HY, Lee SY, Kim JC. The clinical significance of physical activity in maintenance dialysis patients. Kidney Blood Pressure Res. 2017;42(3):575–86.
Scapini KB, Bohlke M, Moraes OA, Rodrigues CG, Inácio JF, Sbruzzi G, et al. Combined training is the most effective training modality to improve aerobic capacity and blood pressure control in people requiring haemodialysis for end-stage renal disease: systematic review and network meta-analysis. J Physiotherapy. 2019;65(1):4–15.
Yamagata K, Hoshino J, Sugiyama H, Hanafusa N, Shibagaki Y, Komatsu Y, et al. Clinical practice guideline for renal rehabilitation: systematic reviews and recommendations of exercise therapies in patients with kidney diseases. Renal Replacement Therapy. 2019;5(1):1–9.
Ikizler TA, Pupim LB, Brouillette JR, Levenhagen DK, Farmer K, Hakim RM, et al. Hemodialysis stimulates muscle and whole body protein loss and alters substrate oxidation. Am J Physiol Endocrinol Metab. 2002;282(1):E107–16.
Sawant A, Garland SJ, House AA, Overend TJ. Morphological, electrophysiological, and metabolic characteristics of skeletal muscle in people with end-stage renal disease: a critical review. Physiotherapy Canada. 2011;63(3):355–76.
Shemy MB, ElghiteElhossinyElkazeh EA, Radwa EL. Efficacy of exercise program in intra hemodialysis on patients’ quality of life. IOSR J Nurs Health Sci. 2016;5:17–30.
Johansen KL. Exercise in the end-stage renal disease population. J Am Soc Nephrol. 2007;18(6):1845–54.
Storer TW, Casaburi R, Sawelson S, Kopple JD. Endurance exercise training during haemodialysis improves strength, power, fatigability and physical performance in maintenance haemodialysis patients. Nephrol Dial Transplant. 2005;20(7):1429–37.
Afshar R, Shegarfy L, Shavandi N, Sanavi S. Effects of aerobic exercise and resistance training on lipid profiles and inflammation status in patients on maintenance hemodialysis. Indian J Nephrol. 2010;20(4):185.
Zhao C, Ma H, Yang L, Xiao Y. Long-term bicycle riding ameliorates the depression of the patients undergoing hemodialysis by affecting the levels of interleukin-6 and interleukin-18. Neuropsychiatric Dis Treatment. 2017;13:91.
Visweswaran K, Shaffi M, Mathew P, Abraham M, Lordson J, Rajeev P, et al. Quality of life of end stage renal disease patients undergoing dialysis in southern part of Kerala, India: financial stability and inter-dialysis weight gain as key determinants. J Epidemiol Global Health. 2020;10(4):344.
Sethi S, Menon A, Dhooria HP, Makkar V, Dhooria GS, Chaudhary R. Evaluation of health-related quality of life in adult patients on hemodialysis. Int J Appl Basic Med Res. 2021;11(4):221.
Acknowledgements
We are thankful to our funding agency AHERF and nephrologist K.N. Singh, S. Jasuja, D.K. Agarwal, A. K. Sarin, and J. K. Hota for their kind reference of their patients for this study. We also appreciate the contribution of Anjali Sharma in our study. We the authors are grateful to our patients for cooperating and supporting us throughout our study. We owe our gratitude to Indraprastha Apollo Hospitals for providing us all the necessary support from inception to completion of this study.
Funding
Funding from AHERF-Apollo hospitals educational research foundation for providing us monetary support required for the study.
Author information
Authors and Affiliations
Contributions
Seema Grover facilitated the design, compliance related to research, ensured data quality, analysis, and integrity in accordance with policy and procedures. Vaishali Goyal helped in collecting the data, informed consent, data compilation, and interpretation for the study. Nirmal Kumar Ganguly and Gautam Kumar Saha helped in expert medical advice and facilitated the patient care and services. Varsha Chorsiya helped in manuscript writing, statistical analysis, and compilation. The manuscript was read and approved by all the authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted in accordance with the research Institutional ethics committee – clinical studies Indraprastha Apollo Hospitals, New Delhi, Reg No.: ECR/5/Inst/DL/2013/RR-16, IEC Application Number–IAH/022/04-19. An informed consent was taken from patients after explaining the purpose and details of the study. All queries were answered prior to the measurement.
Consent for publication
We confirm that all authors have approved the manuscript and agree with its submission to this journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Grover, S., Goyal, V., Chorsiya, V. et al. Effect of intradialytic exercises (IDE) on maximal oxygen consumption and quality of life undergoing hemodialysis in Indian population—a pilot study. Bull Fac Phys Ther 27, 27 (2022). https://doi.org/10.1186/s43161-022-00086-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43161-022-00086-8