
Abstract
Background
Smoking mainly induces COPD, but occupational threats play a significant role in the development of COPD. Previous studies concerning pulmonary rehabilitation mainly focus on COPD caused by smoking, but COPD induced by occupational hazards has not been studied yet. We aimed to identify the efficacy of IMT (Inspiratory Muscle training) using classic POWERbreathe versus DB (Diaphragmatic breathing) plus PLB (Pursed-lip Breathing) exercise in dyspnea, exercise capacity and pulmonary function parameters in occupational COPD farmers with moderate-to-severe COPD (GOLD II–III) FEV1% 30–79%.
Methods
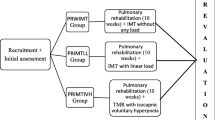
A prospective supervised RCT (Randomized Controlled Trial) included 60 farmers with COPD assigned randomly into two groups; Group A performed IMT using a classic POWERbreathe, and Group B performed DB plus PLB. Both groups completed two daily sessions for three months, seven days/week.
Results
Between-group differences outcome scores were compared, and there was a more remarkable significant improvement in exercise capacity, lung parameters, and dyspnea using the mMRC scale in the IMT group compared to DB plus PLB group. The 6MWT distance (effect size Cohen’s d: 1.69), FEV1 (effect size Cohen’s d: 0.78), FEV1/FVC (effect size Cohen’s d: 0.86), FVC (effect size Cohen’s d: 1.01), and mMRC score (effect size Cohen's d: 1.12) were significantly improved in group A (p < 0.05).
Conclusion
This study demonstrated that the IMT group showed better exercise capacity, dyspnea, and pulmonary function outcomes in occupational COPD farmers. Further studies require COPD patients from different occupations.
Similar content being viewed by others


1 Background
Chronic obstructive pulmonary disease (COPD) is the primary cause of death and disability globally. It is still a vital public health concern due to the continuous increase in healthcare burdens related to recurrent patient hospitalizations [1]. The prevalence and morbidity of COPD are exaggerated with age; its burden is anticipated to progress in the next few years due to an increased population lifespan with continuous exposure to its risk factors [2].
COPD was formerly identified as a smoking disease but is now recognized as a risk of some occupational exposures [3]. About 15–20% of COPD cases are caused by occupational exposure [4]. Farming activities represent one of the occupations at higher risk of COPD [5]. Previous cohort studies illustrated that farmers with long-term exposure to organic dust for 15–40 years had a higher risk for COPD [6]. During their life, they are exposed to multiple agricultural exposures, including organic and inorganic dust, bacteria, endotoxin, spores, and potentially toxic gases, such as ammonia and hydrogen sulfide, that increase their risk of COPD [7]. In general, the proportion of the population working in agriculture is rising worldwide, especially in developing countries, where workers often use pesticides with inadequate protective equipment or training [8]. Farmers use pesticides during their work to eliminate insects and weeds, a significant barrier for farmers to prevent harvest losses. Recent studies illustrated a substantial relationship between exposure to insecticides and herbicides and the risk of obstructive lung diseases [9]. Additionally, farmers are exposed to mould spores when they move or work with hay, grain, or silage materials in which mould spores have grown; mould exposures were associated with worse outcomes in COPD [10].Exposure of farmers to COPD increases economic burdens on them, their families and healthcare societies.
Crop farmers are at higher risk for developing chronic respiratory symptoms, about three-fold higher among crop farmers exposed to more than 20 years than those with shorter job exposure(odds ratio [OR] = 3.20 [0.95–11.41] at 95% CI [11]. COPD prevalence among crop farmers was 11.9% [12]. However, smoking is a risk factor for lung function decline in COPD patients and is associated with adverse outcomes [13]. The progression of occupational COPD is the same as in smoking-related COPD, where the airways aren't wholly reversed. Studies showed that never smokers with COPD, compared to COPD smokers, have fewer symptoms, milder disease and lower levels of inflammatory markers [14]. Earlier studies illustrated that dyspnea is a significant cause of disability and anxiety in COPD patients and a frequent cause of exercise intolerance [15, 16]. Crop farmers are at higher risk of developing dyspnea [11], attributed to inspiratory muscle weakness [17]. Further previous studies illustrated that forced expiratory volume at first second(FEV1) and FEV1/FVC reduced in farmers, with increased annual loss in FEV1 [18]. This yearly loss could deteriorate their QOL (quality of life), impair their working abilities, and cause their productivity loss.
According to GOLD (Global Initiative for Chronic Obstructive Lung Disease) guidelines in 2022, no pharmacotherapy is conclusive enough to reduce the rate of FEV1 decline in COPD patients [19]. GOLD recommendations aimed to improve patients' QOL and functional status by maintaining optimal lung function, reducing disease symptoms, and preventing acute exacerbations [19]. Studies illustrated that pulmonary rehabilitation is an essential component of COPD management and is associated with improvements in symptoms, exercise tolerance, and QOL [20]. Earlier studies confirmed that IMT improves inspiratory muscle strength, dyspnea, QOL and exercise capacity in COPD patients [21]. Other studies illustrated that PLB combined with DB effectively promotes pulmonary function and exercise capacity in COPD patients [22]. Although most studies were performed on COPD-induced due to smoking, its impact has not been identified in occupational COPD farmers.
The study aimed to illustrate the impact of IMT using classic POWERbreathe compared to DB plus PLB exercise in dyspnea, exercise capacity and pulmonary function parameters in COPD farmers. This study will act as a nucleus for physical therapy in occupational COPD research areas to illustrate if COPD farmers will have the same outcomes as COPD induced by smoking only. We hypothesize the study outcomes will be better than COPD caused by smoking.
2 Methods
2.1 Participants
A prospective supervised single, blinded randomized controlled trial (RCT) was conducted at Beni-Suef University Hospital, in the outpatient department of Chest disease, Beni-Suef, Egypt. All our participants were selected from Beni-Suef Governorate in Middle Egypt. Much of its economy depends on agriculture, an essential agricultural land in Egypt. Wheat, sorghum, maize and barley were the most significant crops cultivated by Egyptian farmers [23]. The patients were randomized into two groups (random numbers in sealed envelopes by a research assistant who was not involved in data collection. The participants were assigned to the IMT and DP plus PLB groups in a 1:1 ratio. Between 2019 and January 2020. One hundred and one patients with COPD enrolled in the study after being confirmed to have moderate-to-severe COPD by spirometry (GOLD II–III) FEV1 30–79%.
The inclusion and exclusion criteria of the study populations are presented in Fig. 1. One hundred and one COPD patients were screened for eligibility; 88 eligible subjects were randomized into two groups; (43 subjects) in the IMT group and (45 subjects) in DP plus PLB group participated in the study. Twenty-eight patients dropped -outs of the study. Reasons for drop-outs from the study included withdrawal (n = 12), worsening of COPD symptoms (n = 12), acute embolism (n = 2) and death (n = 2).

Follow-up diagram
Basic demographical information of study populations, in addition to clinical data, includes years of farming, and co-morbidities, e.g. HTN (Hypertension), DM (Diabetes Mellitus, and IHD (Ischemic heart disease)). Furthermore, spirometry parameters were collected by a chest physician. The same physiotherapist did a rehabilitation program for both groups. Group A; performed IMT using the classic POWERbreathe device, and Group B performed DB combined with PLB exercise training. Patients in both groups performed two sessions /day for three successive months, seven days/ week at Beni-Suef University Hospital, in the outpatient department of Chest disease, Beni-Suef, Egypt.
2.2 Inclusion and exclusion criteria of the study populations
Inclusion criteria Participants from Beni-Suef governates who only worked in crop farming throughout their life with no other labour except farming and were confirmed to have occupational COPD by a specialized Chest physician at the baseline before the start of the study and post-intervention. They have been guaranteed moderate-to-severe COPD (GOLD II–III) FEV1% 30–79% by spirometry, with no previous participation in a pulmonary rehabilitation program. And their clinical conditions are stable without any change in their medication than prescribed by their chest physician according to GOLD recommendations in the last four weeks with no physiotherapy involvement in the medication they use.
Exclusion criteria were Patients with a smoking history to avoid biased results, unstable heart diseases, psychiatric problems, and severe complications, such as previous cardiothoracic surgery.
All patients who met the eligibility criteria were randomly divided into two groups; Group A included IMT using a classic POWERbreathe device, and Group B included patients who performed DB combined with PLB exercise training. Both groups completed two sessions/day for three months, seven days per week. All patients continued to take their medication during the study duration. The structural questionnaires were written in English and then translated into Arabic.
2.3 Assessment
2.3.1 Spirometry
COPD diagnoses were confirmed with spirometry that allows the determination of the extent of airflow obstruction and monitoring progression of the disease using ATS/ERS standardization of spirometry 2019 Update [24]. FEV1 and FVC (Forced vital capacity) were expressed as the percentages of the predicted values. A trained chest physician performs this investigation. Patients with an FEV1/FVC ratio of less than 0.7 are confirmed to have airway obstruction [25]. Patients with moderate-to-severe COPD by criteria of GOLD (GOLD II–III) their FEV1% 30–79% after bronchodilator drugs [19]
2.3.2 Modified British Medical Research Council (mMRC)
It is considered a suitable method for the assessment of dyspnea symptoms [26,27,28]. It is a simple and valid tool for assessing breathlessness in COPD patients [15]. An mMRC score ≥ 2 is used to separate "less breathlessness" from "more breathlessness [15]. The ROC curve indicated a cutoff point of ≥ 2 for physical inactivity with 66%sensitivity, and 56% specificity, while for severe physical inactivity with 81% sensitivity and 66% specificity, and sedentary behaviour with 61%sensitivity and 70% specificity [29].
2.3.3 The six-minute walk test (6MWT)
The 6MWT has been used to measure the functional status of patients; it is a predictor of morbidity and mortality [30]. It was reproducible in COPD patients with an intra-class correlation coefficient of 50.93 [31]. The study was performed based on the protocol proposed by the ATS (American Thoracic Society guidelines). The corridor length was 30 m, with encouragement that should be used throughout the test [32]. All participants were encouraged to walk as far as possible for 6 min. They instructed in standard Arabic, with each patient will perform the test twice on the same day with an hour of rest between two tests. Before and directly after the test, the HR (Heart rate), BP (Blood pressure), O2 (oxygen saturation) and the maximal distance walked through the test were documented in addition to the dyspnea score measured by the modified Borg scale of each participant.
2.3.4 Modified Borg scale
It is a reliable and comprehensive scale that monitors and guides exercise intensity. It is an effective tool for predicting performance and defining strategies to increase physical performance quality. It is a valid measure of dyspnea in COPD patients [30]. It assesses baseline and post-6MWT dyspnea and overall fatigue [30]. It is rated from 0 (no dyspnea), where breathing is causing no difficulty at all, to 10 (maximum dyspnea), where breathing difficulty is maximal [32].
2.3.5 Inspiratory muscle training (IMT) using classic POWERbreathe device for (Group A)
The patients were instructed to perform IMT using a threshold inspiratory muscle trainer MTL-IMT ( POWERbreathe Medic, HaB 2 International Ltd., Southam, UK) at a resistance generating a pressure corresponding to 30% of the initial PI max for each session. The intensity was increased (+ 5%) after 14 days during the training to reach 60% of the initial PI max. The training consisted of twice daily sessions with 30 breaths (4–5 min/session) performed seven days/week for three successive months.
2.3.6 Diaphragmatic breathing (DB) combined with pursed lip breathing (PLB) group (Group B)
The patients in group B were instructed to perform DB with PLB. This training consisted of twice sessions /day with 30 breaths (4 –5 min/session) performed seven days/week for three successive months. For DB, the patient is instructed to take deep inspiration from their nose, make their abdomen like a balloon, hold their breathing and expire with a sigh [32]. Additionally, PLB consists of a soft exhalation performed for 4–6 s against the resistance of partially closed lips. The patient is ordered to inhale through the nose, moving the abdominal muscles outward so that the diaphragm lowers and the lungs fill with air and gently exhale through pursed lips [32].
2.3.7 Study outcomes
The primary outcome is to identify the impact of IMT using classic POWERbreathe compared to DB plus PLB exercise in dyspnea and exercise capacity. The secondary outcome is to compare the efficacy of IMT compared to DB plus PLB exercise on pulmonary function in COPD farmers.
2.3.8 Sample size calculation
Before the participants were included in the study, the sample size was measured using Jamovi 2.3.24 program. Based on the previous study, the dyspnea value using mMRC was taken into account among our outcome measurements, and the effect size was 0.982 [33]. According to this study, the number of participants in each group should be at least 23 with 95% CI and 90% power.
2.4 Statistical methods
Data processing and analysis using IBM SPSS Statistics 20 (SPSS Inc, Chicago, IL, USA). Descriptive statistics were analyzed, and parametric data results were reported as mean ± standard deviation (SD). Statistical assumptions are verified through tests of normality by the Kolmogorov–Smirnov Test. The independent sample t-test tested inter-group differences before treatment for parametric data and the Mann–Whitney test for non-parametric data. The effect of IMT or DP plus PLB before and after the treatment on dyspnea, lung function parameters and functional capacity using 6MWT were tested by paired t-test. The effect size between-groups differences were calculated using Cohen's d test to describe the differences in the related treatments and classified as small (d ≥ 0.20 and < 0.50), medium (d ≥ 0.50 and < 0.80), and large (d ≥ 0.80). All statistical test was statistical significance at p-values < 0.05.
3 Results
The baseline characteristics of COPD participants before intervention are illustrated in Table 1. A total of 60 patients were included. Each group contained 30 male patients. Both groups had no significant differences except in BMI (body mass index) and farming duration p < 0.05.
Between groups before the intervention, there was a significant difference in resting DBP, O2 saturation,6MWT distance,post-6MWT HR, number of stopping times during 6MWT, post-6MWT dyspnea using Borg scale, and FEV% predicted p < 0.05 illustrated in Table 2
Table 3 illustrates after three months of intervention, patients in group A showed that 6MWT distance and lung function parameters were significantly increased, but dyspnea sensation using Borg and mMRC scales significantly decreased p < 0.05.
While patients in group B showed only 6MWT distance was significantly increased, dyspnea sensation was decreased considerably using the Borg and mMRC scales with no significant improvement in lung function parameters p < 0.05.
Table 4 illustrates after three months of interventions, differences between groups demonstrated that Group A showed more significant improvement in 6MWT distance, FEV1%, FVC %, FEV1/FVC, and dyspnea scale using mMRC than Group B (p < 0.05).In group A, the 6MWT (p = 0.000, effect size Cohen’s d: 1.69), FEV1 (p = 0.001, effect size Cohen's d: 0.78), FEV1/FVC (p = 0.003, effect size Cohen’s d: 0.86), FVC(p = 0.000, effect size Cohen’s d: 1.01), and mMRC score (p < 0.005, effect size Cohen’s d: 1.12) compared to group B.
4 Discussion
The main findings of this study are that three months of intervention in COPD farmers group A showed more significant improvement in dyspnea and 6MWTD compared to group B. And only group A showed significant improvement in lung function (FEV1, FEV/FVC, and FVC) p < 0.005.
Our results showed a substantial decline of dyspnea in both groups using the mMRC scale but a more significant decrease in symptoms in group A (effect size Cohen's d: 1.12, large effect size). The mean reduction in the mMRC score was 1.5 in group A, and 1 point decline was observed in group B from the baseline. Our results were supported by results of previous studies that IMT using POWERbreathe training compared to control was associated with decreased dyspnea intensity [34, 35]. Our findings are similar to the results of another study that using IMT causes dyspnea decrease using the baseline dyspnea index score (the effect size Cohen’s d was 1.67) [36]. Furthermore, when IMT was added to manual therapy, induced dyspnea decline with a mean decrease of mMRC was 0.78 score (the effect size Cohen’s d was 0.982) [33]. Contrary to our results, previous studies showed no significant improvement in dyspnea when adding IMT to pulmonary rehabilitation [37, 38]. The differences in outcomes to IMT among these studies may be varied according to the severity of COPD, respiratory muscle strength at baseline, smoking history and duration of smoking cessions as a respiratory symptom in COPD patients was lower among ex-smokers ≥ 10 years earlier compared with current smokers [39]. Further studies are required to identify rehabilitation responses among current smokers, ex-smokers and occupational COPD patients.
On the other hand, our results showed that DB and PLB training significantly relieved dyspnea matching earlier studies that PLB exercise [40, 41] and DB exercises were associated with decreased dyspnea [41]. While contrary to the results of the previous research, where no significant differences in dyspnea were observed after the participants performed combined DB plus PLB exercise or even using DB training only [22]. The improvement of dyspnea among group B despite no significant increase in O2 saturation after rehabilitation may be attributed to none of our participants showing exercise-induced oxygen desaturation (EID) post-6MWT. O2 saturation ≤ 88% with exercise is indicated for continuous oxygen use in COPD patients with resting non-hypoxemia [42]. In addition, all of our participants were younger, with a mean age ± SD of 60.4 ± 5.3 years, had moderate to severe COPD and worked in farming only with no smoking history than previous studies [22, 38].
The explanation for a greater significant decline in dyspnea sensation in group A than in group B may be the ability to monitor applied loads' training through sessions objectively. Furthermore, the IMT protocol using POWERbreathe was nonspecific, as it encouraged the recruitment of the diaphragm and all inspiratory muscles in response to the extrinsic mechanical loading [34]. Previous studies showed dyspnea improvement is associated with decreased relative diaphragm electromyography/diaphragm electromyography maximum (EMGdi/EMGdimax) ratio and increased inspiratory muscle endurance time by about three-fold [34]. In addition to IMT, POWERbreathe was associated with significant and large increases in inspiratory mouth pressure (Pimax) [43]. However, all of these studies were performed on COPD induced by smoking—the EMG activity of the diaphragm and Pimax in occupational COPD pre and post-IMT has not been illustrated yet.
Our results revealed significant improvement in functional capacity in both groups. IMT group showed more significant improvement in 6MWTD (effect size Cohen’s d: 1.69, large effect size) than patients in group DB plus PLB exercise. The mean change in 6MWT distance pre and post-intervention was [84.2 (61.5–106.8 m), 95% CI], approximately three folds than observed in group B [24.2 (10.18–38.2 m), 95% CI], with two groups, the mean difference was [105.3 (73.3–137.2), 95% CI]. Our results matched those of previous studies that use IMT to improve functional capacity using 6MWT by 66 m (Cohen’s d: 0.91), 48 m (the effect size of Cohen’s d was 2.49), and 44 m (effect size of Cohen’s d: 0.56) respectively [33, 36, 44]. Moreover, previous studies showed that IMT showed a mean increase in 6 MWT distances by 42 m after two months of training compared to the control (17 m) [35]. And a 56m increase in 6MWT distance [45]. Additionally, the meta-analysis showed that IMT significantly enhances exercise capacity during 6MWT by 32 m [21]. Studies showed that a distance greater than 50 m improvement is considered to be the distance clinically significant for PR programs [20]. The remarkable progress among our IMT group and previous studies may have occurred due to lung pressure improvement. Previous studies showed that both MIP (max inspiratory pressure) and MEP(maximum expiratory pressure) values improved with IMT [35]. Additionally, our rehabilitation program is long-term rehabilitation training in comparison to previous studies, which is limited to 3 to 8 weeks [21, 35, 36, 45]. Long-term exercise programs induced a neural conditioning effect, improving the neuromuscular recruitment pattern and enhancing muscle strength [46]. Some studies lasted for 3 and 4 months, respectively, where the training program was three times/per week [33, 44]. The number of sessions per week could provide better improvement in functional capacity. Furthermore, all of our patients had no smoking history, as smoking was a risk factor for a decline in lung function in COPD patients and associated with poor outcomes [13]. Future studies must compare the efficacy of the combination of pulmonary rehabilitation with POWERbreathe in occupational COPD patients vs COPD induced by smoking on functional capacity and QOL.
Our results reveal that IMT only significantly improved pulmonary function parameters with a mean difference of change between both groups FEV1% [12.11 (4.16–20.06), 95%CI], FEV1/FVC [6.9 (2.8–11.16), 95%CI], and FVC% [15.44 (7.6–23.25), 95%CI], p < 0.005. Our results supported by a previous study that IMT compared to the control group showed significant improvement with a mean difference of change FEV1% [0.57 (− 0.05 to 1.20), 95%CI], FVC[ 0.65 (0.01–1.28), 95%CI], FEV1/FVC [0.24 (− 0.38–0.86), 95% CI] [35]. Contrary to our results, previous studies reported no significant difference in pulmonary function parameters in COPD patients trained by specific inspiratory muscle training (SIMT) [47]. And results of a previous study using either mechanical threshold loading (MTL) devices or electronic tapered flow resistive loading (TFRL) devices in COPD subjects GOLD II for eight weeks [48]. Additionally, despite only a previous study that included occupational COPD patients using the same IMT device, this study showed a slight increase in FEV1 values post- rehabilitation, but with no statistical significance p > 0.05[45]. However, this study performed pulmonary rehabilitation and included multidisciplinary programs, including exercise training, respiratory therapy and therapeutic education, but short-term rehabilitation lasts three weeks [45]. Other factors that could have a role in the response of pulmonary function to IMT could be varied according to smoking history, smoking index, duration of rehabilitation or genetic factor. Studies showed COPD with 20 pack-years of smoking, and those at the highest genetic risk (gene-by-smoking interactions) showed lower lung function than those with the lowest estimated genetic risk [13].
On the other hand, our patients in group B showed no significant differences in lung parameters. Our results are contrary to the results of previous studies that the combination of DP plus PLB breathing exercise played a synergistic effect and promoted lung function improvement in COPD patients[49].In addition to the meta-analysis results, PLB plus DB provided higher gains in FEV 1, FVC, and FEV1/FVC[22]. Our finding aligns with the results of two studies where individualized PLB exercise declared no significant changes in FEV 1, FVC, and FEV 1/FVC [50]. And results of earlier studies where no significant difference in FEV 1, FVC, and FEV 1/FVC between patients trained with and without DB exercise [51]. Although our research used combined exercise therapy, no significant changes occurred in pulmonary parameters like in former studies [22]. This is attributed to differences in study participants' average age, severity, course, and duration of COPD. Further studies included patients with COPD induced by smoking and occupational dust needed to illustrate these differences.
Strengthen this study This study is one of the first to focus on rehabilitating occupational COPD in farmers with a relatively large sample size with long-term rehabilitation of respiratory muscles using two different methods.
Limitation of the study This study has some limitations; we included COPD patients with moderate to severe COPD working in crop farming in Beni-Suef governates only. Further studies included farmers with COPD from different governates with different farming activities. Future studies include patients with very severe occupational COPD to identify the impact of breathing exercises on dyspnea, exercise capacity, and pulmonary function. Other studies should include rehabilitating females with occupational COPD as biomass fuel and comparison of improvement with men. In our study, we used scales to assess dyspnea, which can overestimate or underestimate results; objective measures such as EMG are required to identify the activity of accessory muscle post-intervention in occupational COPD patients.
5 Conclusion
The results showed that applying IMT through the threshold POWERbreathe device is practical to enhance dyspnea sensation, exercise capacity and lung function in farmers with occupational COPD Farmers. Increasing awareness among farmers about the hazards of organic dust on the respiratory system by using interventions such as wearing protective equipment during dealing with pesticides to reduce exposure to these chemicals could contribute to lowering the global burden of COPD. In addition, pulmonary rehabilitation is essential to improve QOL and home-based exercise. Future studies are required with patients from different occupations, ages, gender and societies.
Availability of data and materials
Data of the present study can be made applicable upon reasonable request to the corresponding author.
Change history
23 October 2023
A Correction to this paper has been published: https://doi.org/10.1186/s43088-023-00432-2
Abbreviations
- RCT:
-
Randomized controlled trial
- COPD:
-
Chronic obstructive pulmonary disease
- OR:
-
Odds ratio
- FEV1:
-
Forced expiratory volume at first second
- QOL:
-
Quality of life
- GOLD:
-
Global Initiative for Chronic Obstructive Lung Disease
- HTN:
-
Hypertension
- DM:
-
Diabetes Mellitus
- IHD:
-
Ischemic heart disease
- IMT:
-
Inspiratory muscle training
- DB:
-
Diaphragmatic breathing
- PLB:
-
Pursed lip breathing
- mMRC:
-
Modified British Medical Research Council
- 6MWT:
-
The six-minute walk test
- ATS:
-
American Thoracic Society guidelines
- HR:
-
Heart rate
- BP:
-
Blood pressure
- FVC:
-
Forced vital capacity
- FEV1:
-
Forced expiratory volume at first second
- O2 :
-
Oxygen
- mMRC:
-
Modified British Medical Research Council
- SBP:
-
Systolic Blood pressure
- DBP:
-
Diastolic blood pressure
- EID:
-
Exercise-induced oxygen desaturation
- EMGdi/EMGdimax ratio:
-
Diaphragm electromyography/diaphragm electromyography maximum
- Pimax:
-
Inspiratory mouth pressure
- MIP:
-
Max inspiratory pressure
- MEP:
-
Maximum expiratory pressure
- SIMT:
-
Specific inspiratory muscle training
- MTL:
-
Mechanical threshold loading
- TFRL:
-
Tapered flow resistive loading
References
Vogelmeier CF et al (2017) Global strategy for the diagnosis, management, and prevention of chronic obstructive lung Disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med 195(5):557–582. https://doi.org/10.1164/rccm.201701-0218pp
Mathers CD, Loncar D, Projections of global mortality and burden of disease from 2002 to 2030 (in Eng), no. 1549–1676 (electronic)
Greskevitch M, Kullman G, Bang KM, Mazurek JM (2008) Respiratory disease in agricultural workers: mortality and morbidity statistics. J Agromedicine 12(3):5–10. https://doi.org/10.1080/10599240701881482
Terzikhan N, Verhamme KMC, Hofman A, Stricker BH, Brusselle GG, Lahousse L (2016) Prevalence and incidence of COPD in smokers and non-smokers: the Rotterdam Study (in Eng). Eur J Epidemiol 31(8):785–792. https://doi.org/10.1007/s10654-016-0132-z
Guillien A et al (2015) Prevalence and risk factors for COPD in farmers: a cross-sectional controlled study. Eur Respir J 47(1):95–103. https://doi.org/10.1183/13993003.00153-2015
Vested A et al (2019) A nationwide follow-up study of occupational organic dust exposure and risk of chronic obstructive pulmonary disease (COPD) (in Eng). Occup Environ Med 76(2):105–113. https://doi.org/10.1136/oemed-2018-105323
Kennedy S, Kullman G, Lacasse Y, Lawson B, Malmberg P, May J, McCurdy S, Merchant J, Schenker MB, Myers J, Christiani D (1998) Respiratory health hazards in agriculture. Am J Respir Crit Care Med 158(1):S1–S76. https://doi.org/10.1164/ajrccm.158.supplement_1.rccm1585s1
G. W. H. O. a. F. a. A. O. o. t. U. N. L. C. B.-N.-S. IGO. Global situation of pesticide management in agriculture and public health. Report of a 2018 WHO–FAO survey
Pourhassan B, Meysamie A, Alizadeh S, Habibian A, Beigzadeh Z (2019) "Risk of obstructive pulmonary diseases and occupational exposure to pesticides: a systematic review and meta-analysis (in Eng). Public Health 174:31–41. https://doi.org/10.1016/j.puhe.2019.05.024
Kosmidis C, Hashad R, Mathioudakis AG, McCahery T, Richardson MD, Vestbo J (2021) Impact of self-reported environmental mould exposure on COPD outcomes. Pulmonology. https://doi.org/10.1016/j.pulmoe.2021.05.003
Stoleski S, Minov J, Mijakoski D, Atanasovska A, Bislimovska D, Bislimovska J (2020) Specific work activities and exposure to respiratory hazards—predictors of lung function impairment among crop farmers. Maced J Med Sci. https://doi.org/10.3889/oamjms.2020.4641
Eduard W, Pearce N, Douwes J (2009) Chronic bronchitis, COPD, and lung function in farmers: the role of biological agents (in Eng). Chest 136(3):716–725. https://doi.org/10.1378/chest.08-2192
Kim W et al (2021) Interaction of cigarette smoking and polygenic risk score on reduced lung function (in Eng). JAMA Netw Open 4(12):e2139525. https://doi.org/10.1001/jamanetworkopen.2021.39525
Thomsen M, Nordestgaard BG, Vestbo J, Lange P (2013) Characteristics and outcomes of chronic obstructive pulmonary disease in never smokers in Denmark: a prospective population study (in Eng). Lancet Respir Med 1(7):543–550. https://doi.org/10.1016/s2213-2600(13)70137-1
Ohlson CG, Hogstedt C (1988) The MRC Questionnaire on Symptoms of Bronchitis. A comparison with medical diagnoses and lung function. Ann Occup Hyg. https://doi.org/10.1093/annhyg/32.inhaled_particles_vi.539
Gosselink R, Troosters T, Decramer M (1996) Peripheral muscle weakness contributes to exercise limitation in COPD. Am J Respir Crit Care Med 153(3):976–980. https://doi.org/10.1164/ajrccm.153.3.8630582
Killian KJ, Jones NL (1988) Respiratory muscles and dyspnea. Clin Chest Med 9(2):237–248. https://doi.org/10.1016/s0272-5231(21)00502-5
Ø. Omland (2017) Exposure and respiratory health in farming in temperate zones—a review of the literature (in Eng), pp 1232–1966
GOLD (2022) 2022 Global Strategy for Prevention, Diagnosis and Management of COPD, https://staging.goldcopd.org/2022-gold-reports-2
Spruit MA et al (2013) An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation (in Eng). Am J Respir Crit Care Med 188(8):e13-64. https://doi.org/10.1164/rccm.201309-1634ST
Gosselink R, De Vos J, van den Heuvel SP, Segers J, Decramer M, Kwakkel G (2011) Impact of inspiratory muscle training in patients with COPD: What is the evidence? Eur Respir J 37(2):416–425. https://doi.org/10.1183/09031936.00031810
Yang Y et al (2020) The effects of pursed lip breathing combined with diaphragmatic breathing on pulmonary function and exercise capacity in patients with COPD: a systematic review and meta-analysis. Physiother Theory Pract 38(7):847–857. https://doi.org/10.1080/09593985.2020.1805834
Alsherif EA (2020) Cereal weeds variation in middle Egypt: role of crop family in weed composition (in Eng). Saudi J Biol Sci 27(9):2245–2250. https://doi.org/10.1016/j.sjbs.2020.07.001
Graham BL et al (2019) Standardization of Spirometry 2019 update. An Official American Thoracic Society and European Respiratory Society Technical Statement (in Eng). Am J Respir Crit Care Med 200(8):e70–e88. https://doi.org/10.1164/rccm.201908-1590ST
GOLD (2023)Global Initiative for Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2023 report. GOLD website. Updated December 2022. Accessed December 22, 2022. https://goldcopd.org/wp-content/uploads/2022/12/GOLD-2023-ver-1.1-2Dec2022_WMV.pdf
Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA (1999) Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease (in Eng). Thorax 54(7):581–586. https://doi.org/10.1136/thx.54.7.581
Sundh J, Janson C, Lisspers K, Ställberg B, Montgomery S (2012) The dyspnoea, obstruction, smoking, exacerbation (DOSE) index is predictive of mortality in COPD (in Eng). Prim Care Respir J 21(3):295–301. https://doi.org/10.4104/pcrj.2012.00054
Nishimura K, Izumi T, Tsukino M, Oga T (2002) Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD. Chest 121(5):1434–1440. https://doi.org/10.1378/chest.121.5.1434
Munari AB et al (2021) Modified medical research council and COPD assessment test cutoff points (in Eng). Respir Care 66(12):1876–1884. https://doi.org/10.4187/respcare.08889
ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories (2002) ATS statement: guidelines for the six-minute walk test (in Eng). Am J Respir Crit Care Med 166(1):111–7. https://doi.org/10.1164/ajrccm.166.1.at1102
Hernandes NA, Wouters EF, Meijer K, Annegarn J, Pitta F, Spruit MA (2011) Reproducibility of 6-minute walking test in patients with COPD (in Eng). Eur Respir J 38(2):261–267. https://doi.org/10.1183/09031936.00142010
Geddes EL, O’Brien K, Reid WD, Brooks D, Crowe J (2008) Inspiratory muscle training in adults with chronic obstructive pulmonary disease: an update of a systematic review. Respir Med 102(12):1715–1729. https://doi.org/10.1016/j.rmed.2008.07.005
Buran Cirak Y, Yilmaz Yelvar GD, Durustkan Elbasi N (2022) Effectiveness of 12-week inspiratory muscle training with manual therapy in patients with COPD: a randomized controlled study (in Eng). Clin Respir J 16(4):317–328. https://doi.org/10.1111/crj.13486
Langer D et al. (2018) Inspiratory muscle training reduces diaphragm activation and dyspnea during exercise in COPD (in Eng), 1522–1601
Saka S, Gurses HN, Bayram M (2021) Effect of inspiratory muscle training on dyspnea-related kinesiophobia in chronic obstructive pulmonary disease: a randomized controlled trial (in Eng). Complement Ther Clin Pract 44:101418. https://doi.org/10.1016/j.ctcp.2021.101418
Chuang HY, Chang HY, Fang YY, Guo SE (2017) The effects of threshold inspiratory muscle training in patients with chronic obstructive pulmonary disease: a randomised experimental study (in Eng). J Clin Nurs 26(23–24):4830–4838. https://doi.org/10.1111/jocn.13841
Ammous O et al (2023) Inspiratory muscle training, with or without concomitant pulmonary rehabilitation, for chronic obstructive pulmonary disease (COPD) (in Eng). Cochrane Database Syst Rev 1(1):Cd013778. https://doi.org/10.1002/14651858.CD013778.pub2
Beaumont M et al (2015) Inspiratory muscle training during pulmonary rehabilitation in chronic obstructive pulmonary disease: a randomized trial (in Eng). Chron Respir Dis 12(4):305–312. https://doi.org/10.1177/1479972315594625
Liu Y et al (2015) Smoking duration, respiratory symptoms, and COPD in adults aged ≥45 years with a smoking history (in Eng). Int J Chron Obstruct Pulmon Dis 10:1409–1416. https://doi.org/10.2147/copd.S82259
Bianchi R et al (2004) Chest wall kinematics and breathlessness during pursed-lip breathing in patients with COPD. Chest 125(2):459–465. https://doi.org/10.1378/chest.125.2.459
Ceyhan Y, Tekinsoy Kartin P (2022) The effects of breathing exercises and inhaler training in patients with COPD on the severity of dyspnea and life quality: a randomized controlled trial (in Eng). Trials 23(1):707. https://doi.org/10.1186/s13063-022-06603-3
Stoller JK, Panos RJ, Krachman S, Doherty DE, Make B, Long-term Oxygen Treatment Trial Research (2010) Oxygen therapy for patients with COPD: current evidence and the long-term oxygen treatment trial (in Eng). Chest 138(1):179–187. https://doi.org/10.1378/chest.09-2555
Langer D et al. (2015) Efficacy of a novel method for inspiratory muscle training in people with chronic obstructive pulmonary disease (in Eng), no 1538–6724 (Electronic)
Basso-Vanelli RP et al (2016) Effects of inspiratory muscle training and calisthenics-and-breathing exercises in COPD with and without respiratory muscle weakness (in Eng). Respir Care 61(1):50–60. https://doi.org/10.4187/respcare.03947
Postolache P, Nemes R, Croitoru A, Constantin B (2015) The role of pulmonary rehabilitation in occupational COPD. J Environ Prot Ecol 16:521–527
Leelarungrayub J, Pinkaew D, Puntumetakul R, Klaphajone J (2017) Effects of a simple prototype respiratory muscle trainer on respiratory muscle strength, quality of life and dyspnea, and oxidative stress in COPD patients: a preliminary study (in Eng). Int J Chron Obstruct Pulmon Dis 12:1415–1425. https://doi.org/10.2147/copd.S131062
Shahin B, Germain M, Kazem A, Annat G (2008) Benefits of short inspiratory muscle training on exercise capacity, dyspnea, and inspiratory fraction in COPD patients (in Eng). Int J Chron Obstruct Pulmon Dis 3(3):423–427. https://doi.org/10.2147/copd.s1822
Langer D et al (2015) Efficacy of a novel method for inspiratory muscle training in people with chronic obstructive pulmonary disease (in Eng). Phys Ther 95(9):1264–1273. https://doi.org/10.2522/ptj.20140245
Zhang M, Xv G, Luo C, Meng D, Ji Y (2016) Qigong Yi Jinjing promotes pulmonary function, physical activity, quality of life and emotion regulation self-efficacy in patients with chronic obstructive pulmonary disease: a pilot study. J Altern Complem Med 22(10):810–817. https://doi.org/10.1089/acm.2015.0224
Bhatt SP et al (2012) Volitional pursed lips breathing in patients with stable chronic obstructive pulmonary disease improves exercise capacity. Chron Respir Dis 10(1):5–10. https://doi.org/10.1177/1479972312464244
Yamaguti WP et al (2012) Diaphragmatic breathing training program improves abdominal motion during natural breathing in patients with chronic obstructive pulmonary disease: a randomized controlled trial. Arch Phys Med Rehabil 93(4):571–577. https://doi.org/10.1016/j.apmr.2011.11.026
Acknowledgements
Great appreciation for the chest physician at the chest department, Beni-Suef university hospital. Additionally, Professor Dr Taha Hussein for his Bio-statistician analysis. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript. Additionally, they contributed sufficiently to the manuscript and approved the final manuscript. This work has not been published previously, nor is any part of its content currently under consideration for publication elsewhere; it will not be published elsewhere in the same form in English or any other language.
Funding
This research did not receive any specific grant from the public, commercial, or not-for-profit funding agencies.
Author information
Authors and Affiliations
Contributions
MM contributed to the conceptualization, data curation and methodology; SM, AA, MFM and NE were involved in the project administration and supervision; MM assisted in writing—original draft; MM, SM, AA, MFM and NE contributed to writing—review and editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study had been reviewed and approved by the Human Research Ethics Committee faculty of physical therapy, Cairo University, approval number: PT REC/1/6/2017. All participating subjects had received a verbal explanation, written detailed information on the study, and signed consent forms for the interview. The processing of sensitive personal data was based on following the Helsinki Declaration's ethical principles.
Consent for publication
Written informed consent was obtained from all individuals participating in the study.
Competing interests
All authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised to correct the second author’s name from “Sherin Hassan” to “Sherin Mehani”
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mohammed, M., Mehani, S., Aziz, A.A. et al. Efficacy of threshold inspiratory muscle trainer versus diaphragmatic plus pursed lip breathing in occupational COPD. Beni-Suef Univ J Basic Appl Sci 12, 73 (2023). https://doi.org/10.1186/s43088-023-00409-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43088-023-00409-1