
Abstract
Background
The outbreak of coronavirus infectious disease-2019 (COVID-19) is globally deemed a significant threat to human life. Researchers are searching for prevention strategies, mitigation interventions, and potential therapeutics that may reduce the infection’s severity. One such means that is highly being talked in online and in social media is vitamin C.
Main text
Vitamin C is a robust antioxidant that boosts the immune system of the human body. It helps in normal neutrophil function, scavenging of oxidative species, regeneration of vitamin E, modulation of signaling pathways, activation of pro-inflammatory transcription factors, activation of the signaling cascade, regulation of inflammatory mediators, and phagocytosis and increases neutrophil motility to the site of infection. All of these immunological functions are required for the prevention of COVID-19 infection.
Conclusion
Considering the role of vitamin C, it would be imperative to administrate vitamin C for the management of severe COVID-19. However, there is no specific clinical data available to confirm the use of vitamin C in the current pandemic.
Similar content being viewed by others


Background
Vitamin C or ascorbic acid or ascorbate is an inevitable cofactor for mediating countless enzymatic reactions that are accountable for numerous biological activities. It is deemed a robust antioxidant with strong anti-inflammatory and anti-microbial actions [1]. It possesses a wide range of biochemical and biological actions like antioxidant, phagocytosis, neutrophil chemotaxis, microbial clearance, and immunomodulatory, antiviral, and anti-inflammatory effects [2, 3] and improves natural killer cell and T cell proliferation [4]. Besides, vitamin C is required for the synthesis of nor-adrenaline [5], catecholamine [6], and adrenal steroids [7]. It also acts as a cofactor for peptidyl-glycine alpha-amidating monooxygenase that is needed for vasopressin’s endogenous synthesis [8]. Pre-operative administration of vitamin C reduces etomidate-induced adrenal suppression [9]. It has been extensively used to manage critically ill patients [10]. In addition, vitamin C enhances the immune system via several pathways, such as provoking the response of T lymphocytes, augmenting the activity of lymphocytes and phagocytes, increasing interferon levels [11], and scavenging reactive oxygen species (ROS) [12].
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is now deemed as the global health burden [13]. The World Health Organization (WHO) announced COVID-19 as a global pandemic on 11 March 2020 [14]. As of 2 August 2021, over 199.02 million confirmed cases had been identified and more than 4.24 million people died of COVID-19 [15]. All ages people are affected by this virus, and elderly patients with comorbidities are getting severely ill, even death [14]. The symptoms are usually noticed between 2 and 14 days of coronavirus infection and include fever, cough, and shortness of breath [16, 17]. Acute respiratory distress syndrome (ARDS), septic shock, sepsis, heart failure, and viral pneumonia are the most common complications in severe cases [18]. Viral pneumonia with severe acute respiratory failure may lead to death [19]. Besides, multiple organ dysfunctions may provoke cytokine storms and uncontrolled acute inflammation [20, 21].
The Strategic Advisory Group of Experts (SAGE) on immunization of WHO has recommended several COVID vaccines like Astrazeneca, Sinopharm, Pfizer, Moderna, Covax, etc., to bring out the current pandemic under control [22]. It is found that people are getting infected even after taking the vaccine and various adverse effects are noticed following vaccination [23]. So, the questions arise about the safety and efficacy of COVID vaccines. In this hectic condition, social distancing; self-quarantine or home quarantine; hygiene practices such as mouth and nose covering during sneezing, coughing, and cooking; and sustaining a strong immune system are the best measures to impede the spread of COVID-19 infection [16, 24].
Despite there is no detailed clinical record for safe and effective antiviral drugs, some antiviral drugs that target the molecular pathways of COVID-19 have been used throughout the globe [25]. Among them, the only remdesivir has exhibited to be safe and effective in reducing the time to release of hospitalized COVID-19 patients [26]. The use of corticosteroids can only be considered for acute COVID-19 pneumonia patients for the short term to prevent disease advancement toward a severe form [27]. The extensively used chloroquine and hydroxychloroquine have revealed mixed outcomes in several studies and may be harmful owing to cardiac toxicity [28, 29]. So, we should adopt varying levels of protection against the COVID-19 pandemic. In this context, vitamin C may have positive outcomes on this acute viral infection. Moreover, vitamin C may alter susceptibility to respiratory tract infections by promoting coronavirus resistance [14, 30]. In fact, vitamin C-deficient people are prehensile to severe respiratory infections [3, 31], and supplementation with vitamin C may reduce this infection [31]. Therefore, the intervention to use vitamin C to treat COVID-19 infection is not worth surprising. However, in this review, we will outline the possible role of vitamin C supplementation to minimize COVID-19 pandemic complications.
Epidemiological and clinical observations during COVID-19
Several clinical and epidemiological investigations outline the hypothesis regarding vitamin C status and its association with COVID-19. Some recent studies noted that COVID-19 is linked with the cytokine storm, pneumonia, ARDS, C-reactive protein (CRP), and heart failure [19, 32, 33]. In China, chronic fatality rates were 6–10% for individuals with cardiovascular disease, diabetes, hypertension, and chronic respiratory tract disease [34], whereas it is 1.4% in the USA [35]. Again, WHO reported that about 3.4% confirmed cases had died in COVID-19 as of March 3, 2021 (https://www.worldometers.info/coronavirus/coronavirus-death-rate).
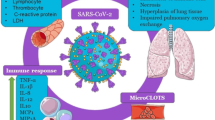
The SARS-CoV-2 virus is transmitted mainly via respiratory droplet, aerosols, contact, and fecal-oral [36]. A receptor-binding motif (RBM) of the inhaled virus binds to angiotensin-converting enzyme 2 (ACE2) of epithelial cells of the nasal cavity. ACE2 is the predominant receptor for SARS-CoV-2 binding. The aftermath of RMB and ACE2 binding is replication and propagation of coronavirus that ultimately lead to infected organ infection [37]. ACE2 is highly expressed in the bronchus, nasal mucosa, esophagus, lung, heart, kidney, bladder, stomach, and ileum, vulnerable to SARS-CoV-2 [38]. Viral replication is assumed to occur in the upper and lower respiratory tract’s mucosal epithelium following multiplication in gastrointestinal mucosa and yield to a mild viremia [39]. Older people are at high risk owing to their diminished immune response and decreased ability to regenerate the damaged epithelium [36]. Few patients remain asymptomatic through controlling the infection at this point. Some patients may develop non-respiratory symptoms, including diarrhea, kidney failure, heart, and liver injury, indicating multiple organ dysfunction [33, 40]. The hypothesized pathogenesis of COVID-19 infection is graphed in Fig. 1.

Hypothesized pathogenesis of SARS-CoV-2 infection
SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; ACE2, angiotensin-converting enzyme 2; ARDS, acute respiratory distress syndrome; RAAS, renin-angiotensin-aldosterone system
The topicality of vitamin C to the COVID-19 pandemic
Vitamin C is deemed to have conducive effects in critically ill patients. It is a free radical scavenger that influences cellular immunity, anti-inflammatory properties, and vascular integrity, and acts as a cofactor in producing endogenous catecholamines [41]. COVID-19 causes life-denunciatory respiratory diseases in humans like severe acute respiratory syndrome (SARS) and the Middle East respiratory syndrome (MERS) [42]. The virulence mechanisms underlying COVID-19 outcomes are not fully understood yet [43]. Different cellular mechanisms such as dipeptidyl peptidase-4 receptor (DPP-4) binding, retinoic acid-inducible gene-I-like receptors (RIG-I) and melanoma differentiation-associated 5 (MDA5) host-recognition, papain-like protease (PL-pro)-mediated replication, and breakdown of M-protein-mediated type-1 IFN (Interferon) initiation evasion have been identified in the closely linked COVID-MERS virus [44]. Of them, DPP-4 has been shown to closely link with COVID-19 in the case of the S1 domain of the spike glycoprotein, pointing out that it would be a primary intensive factor of COVID-19 infections [45]. During COVID-19, an expansive and unrestrained release of pro-inflammatory cytokines or cytokine storm occurs that is also observed in MERS and SARS-CoV-1 [18]. Clinically, this cytokine storm induces systemic inflammation and respiratory inflammation and multiple organ failure [20]. Vitamin C supplementation has shown conducive effects in infections and sepsis. As severe COVID-19 may induce acute respiratory distress syndrome (ARDS) and sepsis, high doses of vitamin C supplementation may contribute to ameliorating inflammation in patients with COVID-19. In fact, vitamin C-deficient individuals are highly susceptible to systemic inflammation, and severe respiratory infections observed throughout the course of COVID-19 [31].
Evidence of antiviral action of vitamin C
Vitamin C supplementation has demonstrated a wide range of antiviral effects against several types of viral infections [46]. Decreased levels of vitamin C have been observed in different viral infections [13] such as sepsis, sepsis-related acute respiratory disease syndrome (ARDS) [47], and other critical conditions of illness [3]. In viral infections, vitamin C is crucial for destroying neutrophil [48] accumulated within macrophages and is accountable for T cell maturation [49]. This enhances phagocytosis and apoptosis [3]. In several murine models, vitamin C has promoted survival from lethal infection [46]. Treatment with vitamin C (50 mg/kg) in the Venezuelan encephalitis virus-affected mice revealed 50% mortality of the controls with less nitric oxide (NO) content and lipid peroxidation products. The treatment group exhibits an increased survival rate (50%) in comparison with untreated infected mice (0%) [50]. A previous study noted that mice infected with the influenza virus could not yield vitamin C, and mice not receiving vitamin C supplementation showed higher lung pathology scores [51].
Vitamin C decreased mortality rate in dose-dependent fashion (100%, 80%, and 50% at 0, 125, and 250 mg/kg/day) in H1N1 (hemagglutinin type 1 and neuraminidase type 1) viral-induced pneumonia [52]. Mice infected with the rabies virus demonstrated nearly 50% mortality while treating intramuscular 100 mg/kg vitamin C daily in comparison with untreated infected mice [46]. Vitamin C supplementation (300 mg/day) in influenza-induced pneumonia is protected from severe infection and reduced the duration of hospital stays [46]. Another study in 133 patients demonstrated that the administration of vitamin C promotes the protection (odds ratio 0.25) from herpes simplex keratitis [53]. Some current studies reported vitamin C as a potential intervention against the coronavirus [16, 54]. Hence, it is hypothesized that vitamin C supplementation may reduce the severity of the current COVID-19 pandemic.
Immunomodulatory role of vitamin C
The immune system is a complex defense mechanism comprising innate and adaptive responses [31]. The innate immune system recognizes and destroys “non-self” rebuffs via inflammatory processes to repair the damage [55]. Vitamin C influences various pathways of immunity such as promoting epithelial barrier activity, migrating white blood cell (WBC) to infected sites (Fig. 2), controlling growth and function of innate and adaptive immune cells, killing microbes via phagocytosis (Fig. 2), and producing antibody [3, 31]. There is evidence that vitamin C may promote pneumonia patients’ health status [56, 57]. Previous findings reported that mice deficient in vitamin C, when infected with H3N2 (hemagglutinin type 3 and neuraminidase type 2) influenza, displayed worse results due to reduce IFN-a/b and increase IL (interleukin)-1a, IL-s1B, and tissue necrosis factor-a (TNF-a) levels [58]. When mice received vitamin C supplementation, these cytokine storm expression profiles were removed. A high dose of IV vitamin C (7.5–50 g) in acute Epstein-Barr virus infection (EBV) exhibited decrease EBV-IgG (immunoglobulin G) profiles, while EBV-IgM antibody profiles were negatively correlated with elevating plasma ascorbate concentration [59].

The role of vitamin C in immune cell functions
Patients with human T-cell leukemia virus, type 1 (HTLV-1)-associated myelopathy (HAM) or tropical spastic paraparesis were treated with oral vitamin C (35–40 mg/kg) for 3–5 days and exerted no changes in HTLV-1 antibody titer in serum and cerebrospinal fluid, revealing an immunomodulated effect [60]. A study reported that rabies vaccination with supplementation of oral vitamin C (2g) elevated serum IFN-a profiles, indicating that vitamin C stimulates interferon production [61]. Another study revealed that a diet containing vitamin C in a mouse model increased interferon production (62–145%) based on the inoculation of viral titer [62]. Vitamin C exhibits immunomodulatory effect by promoting interferon synthesis via signal transducers and activation of transcription 3 (STAT3) phosphorylation [58], enhancing survival in lethal infections [50], controlling cytokine storm-induced organ damage [51], and recycling oxidized quercetin and promoting its antiviral functions [63]. These immunological alterations suggest that vitamin C possesses a good immunomodulatory effect, and we should prioritize it against the current COVID-19 pandemic for pharmacological intervention.
How does vitamin C work against infections as well as COVID-19?
The key reason for severe lung injury in COVID-19 patients is the oxidative stress and excessive free radicals generated from the dysfunctional immune system to kill the virus but end up wounding the patient instead. Vitamin C can reduce oxidative damage and neutralize these free radicals in the lungs. When there is an imbalance between oxidants and antioxidants, body organs’ damage occurs and progresses patients to severe disease [64]. We can improve the antioxidant status by administering sufficient vitamin C. The white blood cells (immune cells) are highly enriched with vitamin C, implying these immune cells’ functional roles. Vitamin C influences phagocytes’ functions, replicating viruses, production of interferon, and maturation of T-lymphocytes. Vitamin C also acts as a safeguard of these immune cells against oxidative damage when they clear out viruses from the body. Based on these knowledge, many hospitals in China, New York, and Shanghai have already started administrating intravenous vitamin C to manage the COVID-19 infections. However, anecdotal evidence of positive response from these hospitals suggests promising vitamin C results against COVID-19 [64].
Clinical efficacy of vitamin C in critically ill patients without COVID-19
More than hundreds of animal studies have demonstrated that a few grams of vitamin C’s daily dose may prevent infections [65]. A pilot study on 24 critically ill patients with sepsis revealed that intravenous (IV) vitamin C administration reduces the Sequential Organ Failure Assessment (SOFA) scores and levels of pro-inflammatory markers (Table 1) significantly over the 4-day study period in patients who received 50 and 200 mg/kg per day vitamin C in comparison with patients who received placebo [66]. Interestingly, a randomized control trial did not change levels of inflammatory markers or SOFA scores in sepsis-induced ARDS patients (n = 167) after IV vitamin C 200 mg/kg per day administration for 4 days. However, the hospital stays and the mortality rate decreased significantly in the treatment group in 28 days (p = 0.03) [47]. Several controlled studies point out that the combination therapy of vitamin C, hydrocortisone, and thiamine had auspicious effects in sepsis or severe pneumonia patients [53, 67]. Again, a randomized control trial study in patients with septic shock compared the outcomes of the combination therapy of vitamin C (6 g per day), hydrocortisone (200 mg per day), and thiamine (400 mg per day) to hydrocortisone alone. The study’s findings showed that combination therapy did not affect the duration of a shock though significantly improved the SOFA score in treatment groups (p = 0.03) [68]. These clinical findings suggested that vitamin C may play a significant role in the management of COVID-19 infection.
Clinical data on vitamin C in critically ill patients with COVID-19
A series of clinical trials related to COVID-19 have been launched or announced from the very beginning of COVID-19 to evaluate the therapeutic benefit of vitamin C alone or in combination therapy with one or more substances (e.g., zinc, vitamin D, hydroxychloroquine, and azithromycin) [70]. Randomized controlled trials are currently registered in the National Institutes of Health Clinical Trials (NIHCT)/National Clinical Trial (NCT) to examine monotherapy for severe COVID-19 treatment (to treat, or prevent COVID-19 in combination with hydroxychloroquine and other supplements [70, 71]. The dosing of vitamin C varies widely in these trials, ranging from 250 to 500 mg orally to 24 g IV daily.
Researchers from China have noted that they have successfully treated the moderate to severe COVID-19 patients (n > 50) with large doses of IV vitamin C (10,000–20,000 mg/day). The findings are no incidence of death and a shorter mean hospital stay than untreated COVID-19 patients [13]. Besides, the Shanghai Medical Association has recently endorsed the use of high-dose vitamin C for the management and treatment of hospitalized patients with COVID-19 [72]. A recent review points out that higher doses of IV vitamin C may be required to deplete cytokine storms in ARDS [73]. High doses of vitamin C are deemed to be administered IV route as they are thinly tolerated orally. However, bowel tolerance for vitamin C is elevated in many patients with the severity of illness. So, some patients may tolerate oral doses up to 200 g/day [74]. However, it should be kept in mind that vitamin C is not yet a standard treatment for COVID-19 owing to a shortage of evidence.
Conclusion
In summary, vitamin C possesses positive impacts on curing of infection and this may play a protective role in the current COVID-19 pandemic through boosting the immune system. As a robust antioxidant, vitamin C helps in normal neutrophil function, scavenging of oxidative species, regeneration of vitamin E, modulation of signaling pathways, activation of pro-inflammatory transcription factors, activation of the signaling cascade, nuclear factor κB (NFκB), regulation of inflammatory mediators, gene regulation, phagocytosis, and signaling pathways in T-cells and increases neutrophil motility to the site of infection. These functions are very crucial for the prevention and treatment of COVID-19 infection. So, to develop strong immunity against COVID-19 infection, a regular administration of vitamin C is required. In healthy individuals, 200 mg/day of vitamin C is required to obtain saturated blood levels. The requirement of vitamin C increases during infection, and 1–2 g/day is recommended in this condition. Ongoing randomized clinical trials (RCT) are expected to give more definitive evidences.
Availability of data and materials
Not applicable.
Abbreviations
- COVID-19:
-
Coronavirus infectious disease-2019
- ROS:
-
Reactive oxygen species
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- WHO:
-
World Health Organization
- ARDS:
-
Acute respiratory distress syndrome
- CRP:
-
C-reactive protein
- ACE2:
-
Angiotensin-converting enzyme 2
- RAAS:
-
Renin-angiotensin-aldosterone system
- SARS:
-
Severe acute respiratory syndrome
- MERS:
-
Middle East respiratory syndrome
- DPP-4:
-
Dipeptidyl peptidase-4
- RIG-I:
-
Retinoic acid-inducible gene-I-like receptors
- MDA5:
-
Melanoma differentiation-associated 5
- PL-pro:
-
Papain-like protease
- IFN:
-
Interferon
- H1N1:
-
Hemagglutinin type 1 and neuraminidase type 1
- WBC:
-
White blood cell
- HFF:
-
Human foreskin fibroblast
- ASC-2P:
-
2-Phospho-ascorbate
- H3N2:
-
Hemagglutinin type 3 and neuraminidase type 2
- IL:
-
Interleukin
- TNF-a:
-
Tissue necrosis factor-a
- IV:
-
Intravenous
- EBV:
-
Epstein-Barr virus
- IgG:
-
Immunoglobulin G
- HAM:
-
Human T-cell leukemia virus, type 1-associated myelopathy
- HTLV-1:
-
Human T-cell leukemia virus, type 1
- STAT3:
-
Signal transducers and activation of transcription 3
- SOFA:
-
Sequential Organ Failure Assessment
- NIHCT/NCT:
-
National Institutes of Health Clinical Trials
References
Hernández A, Papadakos PJ, Torres A, González DA, Vives M, Ferrando C, et al. Two known therapies could be useful as adjuvant therapy in critical patients infected by COVID-19. Revista Española de Anestesiología y Reanimación. 2020;67(5):245–52. https://doi.org/10.1016/j.redare.2020.05.002.
Dennis JM, Witting PK. Protective role for antioxidants in acute kidney disease. Nutrients. 2017;9(7). https://doi.org/10.3390/nu9070718.
Carr AC, Maggini S. Vitamin C and immune function. Nutrients. 2017;9(11). https://doi.org/10.3390/nu9111211.
Van Gorkom GNY, Klein Wolterink RGJ, Van Elssen CHMJ, Wieten L, Germeraad WTV, Bos GMJ. Influence of vitamin C on lymphocytes: an overview. Antioxidants. 2018;7(3). https://doi.org/10.3390/ANTIOX7030041.
May JM, Qu ZC, Meredith ME. Mechanisms of ascorbic acid stimulation of norepinephrine synthesis in neuronal cells. Biochem Biophys Res Commun. 2012;426(1):148–52. https://doi.org/10.1016/j.bbrc.2012.08.054.
Bornstein SR, Yoshida-Hiroi M, Sotiriou S, Levine M, Hartwig H-G, Nussbaum RL, et al. Impaired adrenal catecholamine system function in mice with deficiency of the ascorbic acid transporter (SVCT2). FASEB J. 2003;17(13):1–13. https://doi.org/10.1096/fj.02-1167fje.
Patak P, Willenberg HS, Bornstein SR. Vitamin C is an important cofactor for both adrenal cortex and adrenal medulla. Endocrine Res. 2004;30(4):871–5. https://doi.org/10.1081/ERC-200044126.
Prigge ST, Mains RE, Eipper BA, Amzel LM. New insights into copper monooxygenases and peptide amidation: structure, mechanism and function. Cell Mol Life Sci. 2000;57(8):1236–59. https://doi.org/10.1007/PL00000763.
Das D, Sen C, Goswami A. Effect of vitamin C on adrenal suppression by etomidate induction in patients undergoing cardiac surgery: a randomized controlled trial. Ann Cardiac Anaesthesia. 2016;19(3):410–7. https://doi.org/10.4103/0971-9784.185522.
Nabzdyk CS, Bittner EA. Vitamin C in the critically ill - indications and controversies. World J Crit Care Med. 2018;7(5):52–61. https://doi.org/10.5492/wjccm.v7.i5.52.
Baladia E, Pizarro AB, Rada G. Vitamin C for the treatment of COVID-19: a living systematic review protocol. MedRxiv. 2020;2020(04):28.20083360. https://doi.org/10.1101/2020.04.28.20083360.
Bauer SR, Kapoor A, Rath M, Thomas SA. What is the role of supplementation with ascorbic acid, zinc, vitamin D, or N-acetylcysteine for prevention or treatment of COVID-19? Cleveland Clinic J Med. 2020. https://doi.org/10.3949/ccjm.87a.ccc046.
Cheng RZ. Can early and high intravenous dose of vitamin C prevent and treat coronavirus disease 2019 (COVID-19)? Med Drug Discovery. 2020;5:100028. https://doi.org/10.1016/j.medidd.2020.100028.
Infusino F, Marazzato M, Mancone M, Fedele F, Mastroianni CM, Severino P, et al. Diet supplementation, probiotics, and nutraceuticals in SARS-CoV-2 infection: a scoping review. Nutrients. 2020;12(6):1–21. https://doi.org/10.3390/nu12061718.
World Meter. COVID-19 Coronavirus Pandemic. Available from: https://www.worldometers.info/coronavirus/. Accessed 2 Aug 2021.
BourBour F, Mirzaei Dahka S, Gholamalizadeh M, Akbari ME, Shadnoush M, Haghighi M, et al. Nutrients in prevention, treatment, and management of viral infections; special focus on coronavirus. Arch Physiol Biochem. 2020:1–10. https://doi.org/10.1080/13813455.2020.1791188.
Lake MA. What we know so far: COVID-19 current clinical knowledge and research. Clin Med J R College Physicians London. 2020;20(2):124–7. https://doi.org/10.7861/clinmed.2019-coron.
Zabetakis I, Lordan R, Norton C, Tsoupras A. Covid-19: the inflammation link and the role of nutrition in potential mitigation. Nutrients. 2020;12(5). https://doi.org/10.3390/nu12051466.
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–62. https://doi.org/10.1016/S0140-6736(20)30566-3.
Zhang W, Zhao Y, Zhang F, Wang Q, Li T, Liu Z, et al. The use of anti-inflammatory drugs in the treatment of people with severe coronavirus disease 2019 (COVID-19): the experience of clinical immunologists from China. Clin Immunol. 2020;214:108393. https://doi.org/10.1016/j.clim.2020.108393.
Conti P, Ronconi G, Caraffa A, Gallenga CE, Ross R, Frydas I, et al. Induction of pro-inflammatory cytokines (IL-1 and IL-6) and lung inflammation by coronavirus-19 (COVI-19 or SARS-CoV-2): anti-inflammatory strategies. J Biol Regul Homeostatic Agents. 2020;34(2):327–31. https://doi.org/10.23812/CONTI-E.
WHO. WHO lists additional COVID-19 vaccine for emergency use and issues interim policy recommendations, May, 2021. Available from: https://www.who.int/news/item/07-05-2021-who-lists-additional-covid-19-vaccine-for-emergency-use-and-issues-interim-policy-recommendations. Accessed 3 Sept 2021.
Menni C, Klaser K, May A, Polidori L, Capdevila J, Louca P, et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: a prospective observational study. Lancet Infect Dis. 2021;27(7):939–49. https://doi.org/10.1016/S1473-3099(21)00224-3.
Jayawardena R, Sooriyaarachchi P, Chourdakis M, Jeewandara C, Ranasinghe P. Enhancing immunity in viral infections, with special emphasis on COVID-19: a review. Diab Metab Syndrome. 2020;14(4):367–82. https://doi.org/10.1016/j.dsx.2020.04.015.
Cao B, Wang Y, Wen D, Liu W, Wang J, Fan G, et al. A trial of lopinavir–ritonavir in adults hospitalized with severe Covid-19. New England J Med. 2020;382(19):1787–99. https://doi.org/10.1056/NEJMoa2001282.
Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, et al. Remdesivir for the treatment of Covid-19 — preliminary report. New England J Med. 2020;383(19):1813–26. https://doi.org/10.1056/nejmoa2007764.
Russell B, Moss C, Rigg A, Van Hemelrijck M. COVID-19 and treatment with NSAIDs and corticosteroids: should we be limiting their use in the clinical setting? Ecancermedicalscience. 2020;14. https://doi.org/10.3332/ecancer.2020.1023.
Funck-Brentano C, Salem JE. Chloroquine or hydroxychloroquine for COVID-19: why might they be hazardous? Lancet. 2020. https://doi.org/10.1016/S0140-6736(20)31174-0.
Mehra MR, Ruschitzka F, Patel AN. Retraction—“Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: a multinational registry analysis”. Lancet. 2020;395(10240):1820. https://doi.org/10.1016/S0140-6736(20)31324-6.
Hemilä H. Vitamin C and SARS coronavirus. J Antimicrobial Chemother. 2003;52(6):1049–50. https://doi.org/10.1093/jac/dkh002.
Calder PC, Carr AC, Gombart AF, Eggersdorfer M. Optimal nutritional status for a well-functioning immune system is an important factor to protect against viral infections. Nutrients. 2020;12(4). https://doi.org/10.3390/nu12041181.
Ali N. Elevated level of C-reactive protein may be an early marker to predict risk for severity of COVID-19. J Med Virol. 2020;92(11):2409–11. https://doi.org/10.1002/jmv.26097.
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. J Am Med Assoc. 2020;323(11):1061–9. https://doi.org/10.1001/jama.2020.1585.
CDC Weekly C. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) — China, 2020. China CDC Weekly. 2020;2(8):113–22. https://doi.org/10.46234/ccdcw2020.032.
World meter. Coronavirus (COVID-19) Mortality Rate. Last updated: May 14, 22:00 GMT . Available from: https://www.worldometers.info/coronavirus/coronavirus-death-rate. Accessed 3 Aug 2021.
Jin Y, Yang H, Ji W, Wu W, Chen S, Zhang W, et al. Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses. 2020;12(4). https://doi.org/10.3390/v12040372.
Wan Y, Shang J, Graham R, Baric RS, Li F. Receptor recognition by the novel coronavirus from Wuhan: an analysis based on decade-long structural studies of SARS coronavirus. J Virol. 2020;94(7). https://doi.org/10.1128/jvi.00127-20.
Zou X, Chen K, Zou J, Han P, Hao J, Han Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front Med. 2020;14(2):185–92. https://doi.org/10.1007/s11684-020-0754-0.
Xiao F, Tang M, Zheng X, Liu Y, Li X, Shan H. Evidence for gastrointestinal infection of SARS-CoV-2. Gastroenterology. 2020;158:1831–1833.e3. https://doi.org/10.1053/j.gastro.2020.02.055.
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. https://doi.org/10.1016/S0140-6736(20)30183-5.
Wei XB, Wang ZH, Liao XL, Guo WX, Wen JY, Qin TH, et al. Efficacy of vitamin C in patients with sepsis: an updated meta-analysis. Eur J Pharmacol. 2020;868. https://doi.org/10.1016/j.ejphar.2019.172889.
Hou Y, Zhao J, Martin W, Kallianpur A, Chung MK, Jehi L, et al. New insights into genetic susceptibility of COVID-19: an ACE2 and TMPRSS2 polymorphism analysis. BMC Med. 2020;18(1):216. https://doi.org/10.1186/s12916-020-01673-z.
Lau FH, Majumder R, Torabi R, Saeg F, Frank Lau RH, Hoffman R, et al. Ketidakcukupan vitamin D lazim pada COVID-19 yang parah. MedRxiv. 2020;2020(04):24.20075838. https://doi.org/10.1101/2020.04.24.20075838.
Skariyachan S, Challapilli SB, Packirisamy S, Kumargowda ST, Sridhar VS. Recent aspects on the pathogenesis mechanism, animal models and novel therapeutic interventions for middle east respiratory syndrome coronavirus infections. Front Microbiol. 2019;10:569. https://doi.org/10.3389/fmicb.2019.00569.
Vankadari N, Wilce JA. Emerging WuHan (COVID-19) coronavirus: glycan shield and structure prediction of spike glycoprotein and its interaction with human CD26. Emerg Microbes Infect. 2020;9(1):601–4. https://doi.org/10.1080/22221751.2020.1739565.
Colunga Biancatelli RML, Berrill M, Catravas JD, Marik PE. Quercetin and vitamin C: an experimental, synergistic therapy for the prevention and treatment of SARS-CoV-2 related disease (COVID-19). Front Immunol. 2020;11:1451. https://doi.org/10.3389/fimmu.2020.01451.
Fowler AA, Truwit JD, Hite RD, Morris PE, Dewilde C, Priday A, et al. Effect of vitamin C infusion on organ failure and biomarkers of inflammation and vascular injury in patients with sepsis and severe acute respiratory failure: the CITRIS-ALI randomized clinical trial. J Am Med Assoc. 2019;322(13):1261–70. https://doi.org/10.1001/jama.2019.11825.
Anderson R, Smit MJ, Joone GK, Van Staden AM. Vitamin C and cellular immune functions. Protection against hypochlorous acid-mediated inactivation of glyceraldehyde-3-phosphate dehydrogenase and ATP generation in human leukocytes as a possible mechanism of ascorbate-mediated immunostimulation. Ann New York Acad Sci. 1990;587(1):34–48. https://doi.org/10.1111/j.1749-6632.1990.tb00131.x.
Manning J, Mitchell B, Appadurai DA, Shakya A, Pierce LJ, Wang H, et al. Vitamin C promotes maturation of T-cells. Antioxidants Redox Signal. 2013;19(17):2054–67. https://doi.org/10.1089/ars.2012.4988.
Valero N, Mosquera J, Alcocer S, Bonilla E, Salazar J, Álvarez-Mon M. Melatonin, minocycline and ascorbic acid reduce oxidative stress and viral titers and increase survival rate in experimental Venezuelan equine encephalitis. Brain Res. 1622;2015:368–76. https://doi.org/10.1016/j.brainres.2015.06.034.
Li W, Maeda N, Beck MA. Vitamin C deficiency increases the lung pathology of influenza virus-infected gulo-/- mice. J Nutr. 2006;136(10):2611–6. https://doi.org/10.1093/jn/136.10.2611.
Cai Y, Li YF, Tang LP, Tsoi B, Chen M, Chen H, et al. A new mechanism of vitamin C effects on A/FM/1/47(H1N1) virus-induced pneumonia in restraint-stressed mice. BioMed Res Int. 2015;2015:675149–12. https://doi.org/10.1155/2015/675149.
Kim G-N, Yoo W-S, Park M-H, Chung J-K, Han Y-S, Chung I-Y, et al. Clinical features of herpes simplex keratitis in a Korean tertiary referral center: efficacy of oral antiviral and ascorbic acid on recurrence. Korean J Ophthalmol. 2018;32(5):353–60. https://doi.org/10.3341/kjo.2017.0131.
Zhang L, Liu Y. Potential interventions for novel coronavirus in China: a systematic review. J Med Virol. 2020;92(5):479–90. https://doi.org/10.1002/jmv.25707.
Murphy K. Janeway’s Immunobiology. Garland Sci. 2016. https://doi.org/10.1201/9781315533247.
Hemilä H, Douglas RM. Vitamin C and acute respiratory infections. Int J Tubercul Lung Dis. 1999;3:756–61.
Cinatl J, Cinatl J, Weber B, Rabenau H, Gümbel HO, Chenot JF, et al. In vitro inhibition of human cytomegalovirus replication in human foreskin fibroblasts and endothelial cells by ascorbic acid 2-phosphate. Antiviral Res. 1995;27(4):405–18. https://doi.org/10.1016/0166-3542(95)00024-G.
Kim Y, Kim H, Bae S, Choi J, Lim SY, Lee N, et al. Vitamin C is an essential factor on the anti-viral immune responses through the production of interferon-α/β at the initial stage of influenza A virus (H3N2) infection. Immune Network. 2013;13(2):70–4. https://doi.org/10.4110/in.2013.13.2.70.
Mikirova NA, Hunninghake R. Effect of high dose vitamin C on Epstein-Barr viral infection. Med Sci Monitor. 2014;20:725–32. https://doi.org/10.12659/MSM.890423.
Kataoka A, Imai H, Inayoshi S, Tsuda T. Intermittent high-dose vitamin C therapy in patients with HTLV-I associated myelopathy. J Neurol Neurosurg Psychiatry. 1993;56(11):1213–6. https://doi.org/10.1136/jnnp.56.11.1213.
Stantic-Pavlinic M, Banic S, Marin J, Klemenc P. Vitamin C--a challenge in management of rabies. Swiss Medical Weekly. 2004;134:326–7 https://doi.org/2004/21/smw-10506.
Siegel BV. Enhanced interferon response to murine leukemia virus by ascorbic acid. Infect Immunity. 1974;10(2):409–10. https://doi.org/10.1128/iai.10.2.409-410.1974.
Askari G, Ghiasvand R, Feizi A, Ghanadian SM, Karimian J. The effect of quercetin supplementation on selected markers of inflammation and oxidative stress. J Res Med Sci. 2012;17(7):637–41.
The Financial Express. The role of vitamin C in fighting COVID-19 pandemic - The Financial Express n.d. Available from: https://www.financialexpress.com/lifestyle/health/the-role-of-vitamin-c-in-fighting-covid-19-pandemic/2084387/. Accessed 8 Oct 2020.
Hemilä H. Vitamin C and infections. Nutrients. 2017;9(4). https://doi.org/10.3390/nu9040339.
Fowler AA, Syed AA, Knowlson S, Sculthorpe R, Farthing D, DeWilde C, et al. Phase I safety trial of intravenous ascorbic acid in patients with severe sepsis. J Transl Med. 2014;12(1):32. https://doi.org/10.1186/1479-5876-12-32.
Marik PE, Khangoora V, Rivera R, Hooper MH, Catravas J. Hydrocortisone, vitamin C, and thiamine for the treatment of severe sepsis and septic shock: a retrospective before-after study. Chest. 2017;151(6):1229–38. https://doi.org/10.1016/j.chest.2016.11.036.
Fujii T, Luethi N, Young PJ, Frei DR, Eastwood GM, French CJ, et al. Effect of vitamin C, hydrocortisone, and thiamine vs hydrocortisone alone on time alive and free of vasopressor support among patients with septic shock: the VITAMINS randomized clinical trial. J Am Med Assoc. 2020;323(5):423–31. https://doi.org/10.1001/jama.2019.22176.
Khan S, Faisal S, Jan H, Usman H, Zainab R, Taj F, et al. COVID-19: a brief overview on the role of vitamins specifically vitamin C as immune modulators and in prevention and treatment of SARS-Cov-2 infections. Biomed J Sci Tech Res. 2020;28(3):21580–6.
ClinicalTrials.gov. Use of ascorbic acid in patients with COVID 19 - ClinicalTrials.gov n.d. Available from: https://clinicaltrials.gov/ct2/show/NCT04323514. Accessed 7 Oct 2020.
Adams KK, Baker WL, Sobieraj DM. Myth busters: dietary supplements and COVID-19. Annals of Pharmacotherapy. 2020;54(8):820–6. https://doi.org/10.1177/1060028020928052.
Healthline. Can vitamin C protect you from COVID-19? Available from: https://www.healthline.com/nutrition/vitamin-c-coronavirus. Accessed 8 Oct 2020.
Boretti A, Banik BK. Intravenous vitamin C for reduction of cytokines storm in acute respiratory distress syndrome. PharmaNutrition. 2020;12:100190. https://doi.org/10.1016/j.phanu.2020.100190.
Cathcart RF. Vitamin C titrating to bowel tolerance, anascorbemia, and acute induced scurvy. Med Hypotheses. 1981;7(11):1359–76. https://doi.org/10.1016/0306-9877(81)90126-2.
Acknowledgements
The authors would like to express their heartiest gratefulness to Noakhali Science & Technology University for providing the technical support to carry out the article review process.
Funding
No funding was received.
Author information
Authors and Affiliations
Contributions
We declare that this narrative review was conducted by the authors named in this article: MSU, MF, and MSM designed the narrative review. MSU, MF, MSM, and PKB carried out the literature search and writing of the manuscript. MSU, MSI, and MSS helped to supervise the review writing while PKB, MGU, and MF draw the figures and table. Finally, MSU, MSI, and MSS revised and corrected the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors give the consent to publish the manuscript.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Uddin, M.S., Millat, M.S., Baral, P.K. et al. The protective role of vitamin C in the management of COVID-19: A Review. J. Egypt. Public. Health. Assoc. 96, 33 (2021). https://doi.org/10.1186/s42506-021-00095-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42506-021-00095-w