
Abstract
Background
Intravenous thrombolysis is the current therapy of choice in patients with acute ischemic stroke (AIS). While highly effective, the rate at which the procedure is employed is low. Studies evaluating the causes withholding thrombolytic treatment in developing nations remain scarce. We aim to determine the factors withholding thrombolytic treatment in AIS patients.
Methods
This is a retrospective study of AIS patients at Siloam Hospitals Lippo Village, Indonesia, in a 10-month period between April 2019 to February 2020. Patient data were collected from the medical records.
Results
One hundred and forty-five cases of AIS were found within a 10-month period (April 2019 to February 2020). Thrombolysis was performed in 6.90% of all patients with AIS (21.28% when adjusted for eligible patients with onset ≤ 4.5 h). Prehospital delay exceeding 4.5 h was the most common cause of withholding thrombolytic treatment (68.28% of patients present above 4.5 h or with unknown onset). Among patients presenting ≤ 4.5 h, causes withholding thrombolysis include clinical improvement (35.14%), mild non-disabling symptoms (32.43%), patient/family refusal (18.92%), extensive infarction (5.41%), seizures at onset (2.7%), as well as history of acute bleeding diathesis (2.7%) and gastrointestinal bleeding (2.7%).
Conclusions
Prehospital delay constitutes the primary obstacle toward receiving thrombolytic therapy for AIS, especially in developing countries. Among patients with onset below 4.5 h, other notable causes include clinical improvement, mild non-disabling symptoms, and patient/family refusal. Of note, the rate of patient/family refusal in our study was much higher compared to previous findings, which may reflect possible socio-economic, communication, or educational issues.
Similar content being viewed by others

Introduction
Intravenous thrombolysis with recombinant-tissue plasminogen activator (rtPA) constitutes the treatment of choice in acute ischemic stroke (AIS) with an onset below 4.5 h, given the criteria for inclusion and exclusion has been met [1]. In spite of previous studies that have shown that thrombolysis can improve morbidity in AIS patients [2], the employment rate at which the procedure is done is low, ranging from 3.8% to 11.8% [3,4,5,6]. Previous studies have found several factors accountable for low thrombolysis rates, such as mild severity on the National Institute of Health Stroke Scale (NIHSS), clinical improvement, uncertainty in diagnosis, and patient/familial refusal [4, 7]. To our knowledge, research evaluating the causes of limited employment of thrombolytic treatment in Indonesian stroke patients, as well as developing nations in general, remain scarce. The objective of this study is to determine the causes of withholding thrombolytic therapy in AIS patients with an onset below 4.5 h at a tertiary Indonesian hospital.
Methods
Study design and population
This is a retrospective study of AIS patients in an Indonesian hospital (Siloam Hospitals Lippo Village) utilizing secondary data taken from the medical record and emergency department (ED) registry. The study has been approved by the Research Ethics Committee of the Pelita Harapan University Faculty of Medicine. We included all patients with an initial diagnosis of acute stroke above 18 years of age admitted to our ED within a 10-month period between April 2019 and February 2020. Patients with incomplete data, a final diagnosis excluding stroke (i.e., stroke mimics), hemorrhagic stroke, and patients who died prior to intervention, were excluded from the sample. Data collected include patient identity, risk factors (history of cerebrovascular disease, coronary artery disease, atrial fibrillation, hypertension, dyslipidemia, and diabetes mellitus), smoking history, chief complaint, neuroimaging modality; computed tomography (CT) or magnetic resonance imaging (MRI); and results (hemorrhage vs. no hemorrhage), reasons for withholding thrombolysis, length of stay, and parameters of the code stroke system (durations of onset-to-door, door-to-imaging, door-to-specialist response, door-to-needle, and door-to-room). The NIHSS [8, 9] and modified Rankin scale (mRS) [10] scores at admission and discharge were also recorded. Patients received care in the stroke unit (SU), high care unit (HCU), or intensive care unit (ICU), and were managed according to the institute’s stroke clinical pathway, in accordance with standards set by the American Heart Association/American Stroke Association (AHA/ASA) guidelines [9]. Length of stay is defined as the number of days in which the patient received inpatient care, spanning from admission to discharge.
Onset is categorized into those with onset-to-door (duration spent between onset of symptoms to ED arrival) ≤ 4.5 h, those > 4.5 h, and unknown onset/wake-up-stroke. In patients with an onset-to-door/unknown onset, medical records were sought to determine whether thrombolysis was performed. Door-to-imaging, door-to-specialist response, and door-to-room durations are defined as the time the patient entered the ED until neuroimaging is performed, the patient was evaluated by the neurology or neurosurgery service, and the moment the patient enters inpatient care (SU, HCU, or ICU), respectively. Door-to-needle is defined as the time between ED arrival and initiation of thrombolytic treatment. Reasons for withholding thrombolysis were categorized according to contraindications listed on the thrombolytic therapy criteria of exclusion (Table 1), and additionally due to non-technical reasons, such as patient/family refusal.
Statistical analysis
Data were analyzed using IBM SPSS version 26.0 for Windows. Categorical data are presented as frequency and percentage. Numerical data are presented with mean and standard deviation (given that the data are normally distributed) or with median and interquartile range (IQR) (given that the data were non-normally distributed). Comparisons between groups are analyzed with the Mann–Whitney U test on continuous variables, and the Pearson’s chi-squared test or Fisher's exact test on categorical variables when appropriate.
Results
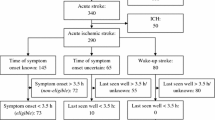
Two hundred and seventeen patients with an initial diagnosis of acute stroke were recorded in the ED registry. Seventy-two were excluded due to incomplete data (44 patients), a final diagnosis excluding stroke (8 patients), hemorrhagic stroke (18 patients), and death preceding intervention (2 patients). The demographic characteristics of patients enrolled in our study are presented below (Table 2). Most patients included in this study were male (62.07%) with a mean age of 60 years (standard deviation ± 12.39). The most frequent risk factors are hypertension (71.72%), diabetes mellitus (37.24%), dyslipdemia (31.72%), previous cerebrovascular disease (30.34%), coronary artery disease (11.03%), and atrial fibrillation (6.21%). The most common chief complaints encountered include motoric weakness (58.62%), followed by dysarthria (13.79%) and altered mental status (8.28%). Of the 145 patients included in the study (Fig. 1), 46 (31.72%) presented with onset-to-door ≤ 4.5 h, 86 (58.62%) presented with onset > 4.5 h, and 13 (8.97%) arrived with unknown onset. The median onset-to-door in the group with an onset ≤ 4.5 h was 2 h (IQR 1.00–3.35) and in the group with onset > 4.5 h was 24 h (IQR 15.5–72.00). Of 13 with unknown onset, head MRI was conducted, and 1 patient was found eligible for thrombolysis (DWI/FLAIR mismatch present). Thrombolysis was performed in 10 patients (6.90%), 9 with onset-to-door ≤ 4.5 h, and 1 with unknown onset. The causes withholding thrombolysis found in our study (Table 3) consisted of clinical improvement (35.14%), mild non-disabling symptoms (32.43%), patient/family refusal (18.92%), extensive infarction (5.41%), seizures at onset (2.7%), as well as history of acute bleeding diathesis (2.7%) and gastrointestinal bleeding (2.7%).

Flow chart depicting the enrollment of acute stroke patients
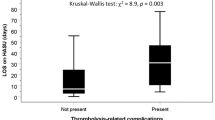
No significant relationship was found between onset-to-door and risk factors nor between onset-to-door and symptoms (p > 0.05). The median NIHSS score at admission and discharge was found to be 4 (IQR 2–9) and 2 (IQR 1–6), respectively, while the mRS scales at admission dan discharge were 2 (IQR 1–3) and 1 (IQR 1–3). National Institutes of Health Stroke Scale and mRS scales at admission and discharge was lower with onset below 4.5 h, compared to those with onset exceeding 4.5 h (p ≤ 0.05). No significant difference in length of stay was found between the two groups (p = 0.281). Head MRI was more frequently employed than CT (89.66 vs. 10.34%).
The time intervals in the management of acute stroke are summarized in Table 4. The medians of door-to-imaging, door-to-specialist, and door-to-room were 45 min (IQR 30.00–71.25), 15 min (IQR 10.00–30,00), and 4 h (IQR 3.00–5.00), respectively. The median door-to-needle time in all patients who underwent thrombolysis was 62.5 min (IQR 48.75–92.50), while the median door-to-needle in patients with known onset (9 patients) was 55 min (IQR 46.25–86.25). In the case of the one patient with wake-up stroke, door-to-needle was 100 min, due to an extended informed consent-family interval of 30 min.
Discussion
The rate of thrombolysis for cases of AIS in our study was 6.8%. When adjusted for potentially eligible patients arriving ≤ 4.5 h, the rate becomes 21.7%. These results are similar to previous studies conducted in Germany [5] (8.4%, 2009), the Netherlands [6] (11.8%, 2012), Australia [11] (4.6%, 2013), Norway [4] (7.6%, 2014), and China [3] (3.8%, 2019). Several factors may account for variations between study populations. First is the difference in volume, in which our sample size is relatively small (145 patients) compared to other studies [3, 5,6,7, 12]. Second, our sample population originates from one center located in an urban area, whereas previous studies examined multiple centers covering urban, suburban, and rural areas [3, 5,6,7, 12]. Third was the difference in thrombolysis cutoff. While our study adopted a cutoff of ≤ 4.5 h, as in studies conducted by Zhou et al. [3], Eissa et al. [6, 11], and Scherf et al. [6], the cutoff for thrombolysis used vary in studies conducted by Faiz et al. [5] (3.5 h) and Singer et al. [5] [3 h].
Of 145 acute stroke patients enrolled in our study, 86 (59.3%) arrived with onset exceeding 4.5 h, and an additional 13 (9.0%) arrived with unknown onset. Taking these into account, it is abundantly clear that prehospital delay constitutes a major obstacle toward the implementation of thrombolytic therapy in AIS. While prehospital delay is prevalent in both developed and developing nations, findings from previous studies, particularly those conducted in developed nations, report lower rates of delay compared to that found in our study: Norway (49%, 2014) [4], Greece (31.2%, 2018) [13], Saudi Arabia (54.6%, 2018) [14], and Switzerland (42%, 2019) [15]. In addition, our findings were similar to studies done in developing countries, such as China (69.2%, 2019) [3] and Egypt (71.2%, 2021) [16]. Several factors have been attributed to delays in patient presentation, such as a lack of stroke awareness, tendencies to wait in hope of spontaneous resolution, and lack of witnesses [4, 11]. However, it is more than likely that more systematic issues underlie this disparity, such as shortages of access to reliable emergency medical services (EMS) (such as ambulances and trained personnel), lack of acute stroke-ready centers to accommodate the susceptible population, absence of a proper inter-hospital referral systems, as well as inadequacies in public health services, transportation, and general education.
Of important note, while an unknown onset hinders the possibility of thrombolytic treatment, it does not absolutely negate its possibility, particularly in facilities equipped with MRI. The presence of a diffusion-weighted imaging (DWI)/fluid-attenuated inversion recovery (FLAIR) mismatch in patients with unknown onset correlates with onset below 4.5 h, and thrombolytic treatment in this subgroup has been demonstrated to be effective in improving clinical outcomes (mRS 0–1) compared to placebo (53.3% vs. 41.8%) [17, 18]. In our study, a DWI/FLAIR mismatch was found in 1 subject (25%), and intravenous thrombolysis was performed with a good clinical outcome (mRS scale 1 at discharge).
Among potentially eligible patients with onset below 4.5 h, the causes withholding thrombolysis found include clinical improvement (35.14%), mild non-disabling symptoms (32.43%), patient/family refusal (18.92%), extensive infarction (5.41%), seizures at onset (2.7%), as well as history of acute bleeding diathesis (2.7%) and gastrointestinal bleeding (2.7%). These results are comparable to results from previous studies, which demonstrate that symptomatic improvement and mild symptoms were the main reasons of withholding thrombolysis [4, 11]. Combined, these two factors account for 52.9% of reasons withholding thrombolysis in potentially eligible patients in our study. At present, the benefits of thrombolytic therapy in mild cases of stroke and spontaneous improvement remain unclear. A previous study of 313 AIS patients with an onset below 3 h and NIHSS score ≤ 5 compared IV thrombolysis and oral aspirin and found no significant difference in the mRS scales between the two groups. [19] A more recent study by Wang et al. in early 2020 demonstrated that rTPA increases clinical output (mRS 0–1) in mild strokes (NIHSS ≤ 5) with occlusion of large blood vessels without tandem lesions, but not in mild strokes without occlusion of large blood vessels, or in occlusion of large blood vessels with tandem lesions [20]. Interestingly, patient/family refusal also accounts for a significant proportion for withholding thrombolysis in potentially eligible patients at 18.92%, much higher compared to the 4.2–8% rate reported in previous studies [21,22,23]. Several factors are possibly accountable for patient/family refusal in our patient population, such as financial concerns, fears over potential complications, communicational issues, and perceived lack of rights/responsibility among family members.
We found that failure of achieving the targets set by the stroke code system did not contribute to failure of employing thrombolytic treatment. In subjects with onset below 4.5 h, door-to-imaging was significantly shorter than in subjects arriving above 4.5 h (median 39.5 vs. 60 min, p < 0.05), comparable with previous studies in Norway (51 vs. 138 min) [4] and Germany (68 vs. 108 min) [24]. While this is most likely due to implementation of stroke code program, the durations in this study still fall short of the standards set by the American Heart Association/American Stroke Association (AHA/ASA) guidelines (below 25 min) [25]. However, no significant difference in door-to-specialist response time in both patient groups with onset below and exceeding 4.5 h (p > 0.05), and the median door-to-needle time in the subject group with an onset ≤ 4.5 h (55.5 min), has met the AHA/ASA door-to-needle target of ≤ 60 min [25]. However, in one case involving wake-up stroke, the door-to-needle time exceeded the target (100 min), due to a delay in obtaining informed consent. In subjects with onset exceeding 4.5 h, the NIHSS and mRS scores at admission and discharge were found to be higher than in those presenting below 4.5 h (p ≤ 0.05), indicating that subjects with an onset > 4.5 h generally presented with more severe clinical appearance, or perhaps due to difficulties in transporting the patient, and with less clinical improvement following treatment. In subjects presenting ≤ 4.5 h, the clinical features of stroke may have not yet fully evolved as the penumbral neurons surrounding the infarct core remains viable and functional. Combined with the eligibility to implement earlier and more aggressive forms of treatment (i.e., thrombolysis), this may explain why subjects presenting below 4.5 h are more likely to have a relatively milder presentation (lower NIHSS) and a better prognosis (lower mRS). In patients with admission exceeding 4.5 h from onset, this delay allows for a greater expansion of the ischemic core and neuronal death, resulting in a more severe clinical presentation, inability to perform thrombolysis, and worse prognosis (higher NIHSS and mRS scores) [26, 27].
The authors recommend that further research be done to evaluate the causes of delayed admission following onset of stroke in developing countries, and considerable efforts (public health campaigns, healthcare system changes) must be made to reduce prehospital delay in developing countries. Furthermore, we recommend implementation of systems in the emergency department that can increase speed without reducing the quality of health services provided for stroke patients, to achieve a door-to-imaging target time of ≤ 25 min, and a door-to-needle target time of ≤ 60 min.
Limitations
A limitation of our study is that our sample volume is smaller than those in previous studies. In addition, our sample was limited to one center located in an urban area, which may lead to differences compared to data collected in suburban or rural areas. Finally, due to the retrospective design of this study, we were unable to further investigate the reasons for delay preceding patient admission.
Conclusion
We conclude that the main obstacle toward receiving thrombolytic therapy for AIS is the delay in patient admission exceeding 4.5 h from onset. In AIS patients with onset below 4.5 h, notable causes of withholding thrombolysis include clinical improvement, mild non-disabling symptoms, and patient/family refusal. Of note, the rate of patient/family refusal in our study was much higher compared to previous findings, which may reflect possible socio-economic, communication, or educational issues.
Availability of data and materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request (rocksy.situmeang@lecturer.uph.edu).
Abbreviations
- AHA/ASA:
-
American Heart Association/American Stroke Association
- AIS:
-
Acute ischemic stroke
- aPTT:
-
Activated partial thromboplastin time
- CT:
-
Computed tomography
- ED:
-
Emergency department
- EMS:
-
Emergency medical services
- DWI:
-
Diffusion-weighted imaging
- FLAIR:
-
Fluid-attenuated inversion recovery
- HCU:
-
High care unit
- ICU:
-
Intensive care unit
- INR:
-
International normalized ratio
- IQR:
-
Interquartile range
- MRI:
-
Magnetic resonance imaging
- NIHSS:
-
National Institutes of Health stroke scale
- PT:
-
Prothrombin time
- rtPA:
-
Recombinant-tissue plasminogen activator
- SD:
-
Standard deviation
- STEMI:
-
ST-elevation myocardial infarction
- SU:
-
Stroke unit
References
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49(3).
You S, Saxena A, Wang X, Tan W, Han Q, Cao Y, et al. Efficacy and safety of intravenous recombinant tissue plasminogen activator in mild ischaemic stroke: a meta-analysis. Stroke Vasc Neurol. 2018;3(1):22–7.
Zhou Y, Yan S, Song X, Gong Y, Li W, Wang M, et al. Intravenous thrombolytic therapy for acute ischemic stroke in Hubei, China: a survey of thrombolysis rate and barriers. BMC Neurol. 2019;19(1):202.
Faiz KW, Sundseth A, Thommessen B, Rønning OM. Reasons for low thrombolysis rate in a Norwegian ischemic stroke population. Neurol Sci. 2014;35(12):1977–82.
Singer OC, Hamann GF, Misselwitz B, Steinmetz H, Foerch C. Time trends in systemic thrombolysis in a large hospital-based stroke registry. Cerebrovasc Dis. 2012;33(4):316–21.
Scherf S, Limburg M, Wimmers R, Middelkoop I, Lingsma H. Increase in national intravenous thrombolysis rates for ischaemic stroke between 2005 and 2012: is bigger better? BMC Neurol. 2016;16(1):53.
Rasyid A, Harris S, Kurniawan M, Mesiano T, Hidayat R, Rilianto B, et al. The reasons acute stroke patients not receiving thrombolysis in an Indonesian referral hospital. Int J Pharm Pharm Sci. 2019;43–6.
Goldstein LB, Samsa GP. Reliability of the National Institutes of Health Stroke Scale. Stroke. 1997;28(2):307–10.
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12).
Wilson JTL, Hareendran A, Grant M, Baird T, Schulz UGR, Muir KW, et al. Improving the assessment of outcomes in stroke: use of a structured interview to assign grades on the modified Rankin scale. Stroke. 2002;33(9):2243–6.
Eissa A, Krass I, Levi C, Sturm J, Ibrahim R, Bajorek B. Understanding the reasons behind the low utilisation of thrombolysis in stroke. Australasian Med J. 2013;6(3):152–67.
Hasan TF, Rabinstein AA, Middlebrooks EH, Haranhalli N, Silliman SL, Meschia JF, et al. Diagnosis and management of acute ischemic stroke. Mayo Clin Proc. 2018;93(4):523–38.
Dimitriou P, Tziomalos K, Christou K, Kostaki S, Angelopoulou SM, Papagianni M, et al. Factors associated with delayed presentation at the emergency department in patients with acute ischemic stroke. Brain Inj. 2019;33(9):1257–61.
al Khathaami AM, al Bdah B, Tarawneh M, Alskaini M, Alotaibi F, Alshalan A, et al. Utilization of intravenous tissue plasminogen activator and reasons for nonuse in acute ischemic stroke in Saudi Arabia. J Stroke Cerebrovasc Dis. 2020;29(5): 104761.
Fladt J, Meier N, Thilemann S, Polymeris A, Traenka C, Seiffge DJ, et al. Reasons for prehospital delay in acute ischemic stroke. J Am Heart Assoc. 2019;8(20).
Aref HM, Shokri H, Roushdy TM, Fathalla F, el Nahas NM. Pre-hospital causes for delayed arrival in acute ischemic stroke before and during the COVID-19 pandemic: a study at two stroke centers in Egypt. PLoS ONE. 2021;16(7): e0254228.
Thomalla G, Simonsen CZ, Boutitie F, Andersen G, Berthezene Y, Cheng B, et al. MRI-guided thrombolysis for stroke with unknown time of onset. N Engl J Med. 2018;379(7):611–22.
Thomalla G, Cheng B, Ebinger M, Hao Q, Tourdias T, Wu O, et al. DWI-FLAIR mismatch for the identification of patients with acute ischaemic stroke within 4·5 h of symptom onset (PRE-FLAIR): a multicentre observational study. Lancet Neurol. 2011;10(11):978–86.
Khatri P, Kleindorfer DO, Devlin T, Sawyer RN, Starr M, Mejilla J, et al. Effect of alteplase vs aspirin on functional outcome for patients with acute ischemic stroke and minor nondisabling neurologic deficits. JAMA. 2018;320(2):156.
Wang D, Zhang L, Hu X, Zhu J, Tang X, Ding D, et al. Intravenous thrombolysis benefits mild stroke patients with large-artery atherosclerosis but no tandem steno-occlusion. Front Neurol. 2020;11.
Zha A, Rosero A, Malazarte R, Bozorgui S, Ankrom C, Zhu L, et al. Thrombolytic refusal over telestroke. Neurol Clin Pract. 2021;11(3):e287–93.
von Kleist T, Meyer D, Rapp K, Meyer BC, Modir R. Characteristics and outcomes of patients who refuse intravenous thrombolysis for acute ischemic stroke—the San Diego experience. J Stroke Cerebrovasc Dis. 2020;29(11): 105137.
Vahidy FS, Rahbar MH, Lal AP, Grotta JC, Savitz SI. Patient refusal of thrombolytic therapy for suspected acute ischemic stroke. Int J Stroke. 2015;10(6):882–6.
Jungehulsing GJ, Rossnagel K, Nolte CH, Muller-Nordhorn J, Roll S, Klein M, et al. Emergency department delays in acute stroke—analysis of time between ED arrival and imaging. Eur J Neurol. 2006;13(3):225–32.
Ruff IM, Ali SF, Goldstein JN, Lev M, Copen WA, McIntyre J, et al. Improving door-to-needle times. Stroke. 2014;45(2):504–8.
Saver JL. Time is brain—quantified. Stroke. 2006;37(1):263–6.
Saver JL, Fonarow GC, Smith EE, Reeves MJ, Grau-Sepulveda MV, Pan W, et al. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA. 2013;309(23):2480.
Acknowledgements
None.
Funding
No funding sources were used in the creation of this manuscript.
Author information
Authors and Affiliations
Contributions
RFVS conceived the study design. All authors (RFVS, AP, RS, YT, JH, CP) equally contributed to data collection, analysis, and in writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study has been approved by the Research Ethics Committee of the Pelita Harapan University Faculty of Medicine. Requirements for written consent for participation by individual participants have been waived by our ethical committee as our research utilizes secondary data taken from the medical record and registry and contains no identifying information.
Consent for publication
Not applicable. Our manuscript does not contain any data, in any form, belonging to an individual person.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Situmeang, R.F.V., Pangestu, A., Stevano, R. et al. Reasons withholding intravenous thrombolysis for acute ischemic stroke in an Indonesian Tertiary Center. Egypt J Neurol Psychiatry Neurosurg 59, 11 (2023). https://doi.org/10.1186/s41983-023-00613-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-023-00613-x