
Abstract
Background
Essential tremor (ET) is now considered as a slowly progressive neurodegenerative disorder with a variety of motor and non-motor manifestations. The objectives of this work were to study the existence of cognitive, mood, olfactory, and balance dysfunctions in ET patients and their relation to tremor severity as well as patients’ activity of daily livings.
Methods
This study was performed on 36 ET patients and 24 healthy controls subjects (HCS) submitted to The Essential Tremor Rating Assessment Scale (TETRAS), advanced activity of daily living scale (AADLs), Montreal cognitive assessment scale (MoCA), Montgomery–Åsberg Depression Rating Scale (MADRS), auditory mismatch negativity (MMN), Sniffin’ Sticks test (SST), computerized dynamic posturography (CDP), and brain MRI diffusion tensor tractography (DTT).
Results
ET patients showed significant decrease in AADLs, MoCA, SST (threshold, identification, and discrimination subscales) as well as visual and vestibular ratios of CDP compared to HCS. Auditory MMN showed significant reduction in the amplitude and prolongation of latencies while corticospinal tracts, thalamo-cortical connectivity, and middle cerebellar peduncles DTT revealed reduced fractional anisotropy in ET patients with normal tracts densities.
Conclusion
ET patients exhibit a wide variety of non-motor manifestations including cognitive impairment, depressive symptoms, hyposmia, and increased risk of falls with consecutive reduced activity of daily living beyond the deleterious effects of the kinetic tremor.
Similar content being viewed by others

Introduction
Essential tremor (ET) is the most common adult onset movements’ disorders affecting 1% of the general population and > 5% of those above the age of 65 years [1]. The traditional descriptions of ET as a benign monosymptomatic illness with postural and/or kinetic tremors had been given way while the disorder is now considered as a slowly progressive neurodegenerative movement disorder which is highly heterogenous in its hereditability, affected body parts, response to treatment, rate of progression, and possible existence of non-motor manifestations [2].
In 2018, The International Parkinson and Movement Disorder Society (MDS) had introduced the term ET–plus to describe patients with additional neurological signs of uncertain significance that are not enough for the assumption of comorbidity or additional diagnosis. However, the permissible spectrums and severities of these non-motor manifestations are poorly defined in objective assessments [3, 4]. These non-tremorgenic manifestations include subtle cerebellar dysfunctions, balance and gait impairments, oculomotor disturbances, cognitive decline, psychiatric abnormalities, hearing and olfactory problems, and upper airways dysfunctions and sleep disturbances [5].
Aim of the work
The aim of the work was to study the cognitive, mood, olfactory, and balance dysfunctions in ET patients and their relation to tremor severity as well as patients’ activity of daily livings (ADLs).
Subjects and methods
The study was a cross-sectional case-control study conducted on 36 ET patients and 24 age, sex, and educational level matched healthy control subjects (HCS). Inclusion criteria consisted of consecutive ET patients aged 50–65 years (to avoid the aging effect on the studied parameters) and diagnosed according to The Consensus Statement on the Classification of Tremors of the MDS [6]. Patients were recruited from the movement disorder clinic, Center of Neurology and Psychiatry, Tanta University Hospitals, in the period from 1 October 2017 to the end of December 2019.
Exclusion criteria encompassed ET patients with comorbid endocrinal, renal, or hepatic diseases as well as middle ear dysfunctions or MRI contraindications. The study protocol was approved by the Research Ethics Committee and Quality Assurance Unit, Faculty of Medicine, Tanta University; the participation was voluntary and informed consents were obtained before engagement in the study.
Included patients were subjected to tremor severity assessment using The Essential Tremor Rating Assessment Scale (TETRAS) [7] as well as history taking stressing on family history of ET, disease duration and response to propranolol (ET was considered propranolol responsive if the TETRAS improved by ≥ 50% from the baseline). Included subjects were also submitted to the Montreal Cognitive Assessment Scale (MoCA) Arabic Version, the advanced activities of daily living scale (AADLs) [8], and Montgomery–Åsberg Depression Rating Scale (MADRS) [9].
Studied subjects were also submitted to auditory mismatch negativity (MMN) test which used the oddball paradigm for speech stimuli, da/ga sounds as standard/deviant stimuli, presented at 1/s repetition rate, 15% deviant probability, and 50 dB sound level. MMN was calculated in the difference waveform according to manual specification of Smart Evoke Potential, Home Intelligence Service (HIS), USA (Additional file 1).
Computerized dynamic posturography (CDP) and sensory organization test (SOT) were also performed to examine the somatosensory (SOM), visual (VIS), and vestibular (VEST) balance systems using the Balance Quest provided by Framiral, Cannes, France (Multitest Equilibre 6.1.37.0) with static/dynamic platform by Micromedical Technologies (http://perso.wanadoo.fr/framiral/multi_gb.htm) [10] (Additional file 1).
Olfactory performance was performed using the extended n-Butanol, Burghart Sniffin’ Sticks Test (SST), LA-13-00134, Wedel, Germany, regarding Rumeau and colleagues, 2016 [11]. The test consists of three subtests: threshold (TSST), discrimination (DSST), and identification (ISST). The global TDI olfactory score (sum of threshold, discrimination, and identification) classify smell functions as follows: 31–48 normosmia, 16–30 hyposmia, and ≤ 15 functional anosmia [11] (Additional file 2).
Brain MRI images were acquired using 1.5–Tesla, General Electric Scanner with quadrature 8 channels head coil, GE Healthcare, Milwaukee, WI, USA. Diffusion tensor tractography (DTT) and 3D macroscopic orientation of the corticospinal tract (CST), middle cerebellar peduncle (MCP), and thalamo-cortical connectivity (TCC) were reconstructed through data acquired from diffusion tensor imaging (DTI). It was assessed by single-shot spin echo–planar imaging with TR 8830 ms, TE 80 ms, acquisition matrix 112 × 110 mm, acquisition voxel 2.00/2.03/2.00 mm, field of view: right–left 224 mm, anteroposterior 224 mm and feet–head 120 mm, voxel size: right–left 2 mm, anteroposterior 2 mm, and slice thickness 2 mm, reconstruction voxel size 1.75 mm, gradient direction 32, b value 1000 mm/s, and number of slices was 60 with total scan time 9:51 min [12].
Statistical analysis was conducted using SPSS Prism, version 20, 2013 created by IBM, Chicago, IL, USA. Statistical differences were tested using chi-square for categorical variables and Student’s t test for numerical ones. For bilaterally assessed parameters, all included subjects were represented by the mean measure of both sides. Correlation analysis was performed using Pearson’s correlation test. p value < 0.05 was considered statistically significant.
Results
The studied ET patients’ age was 62.6 ± 4.6 years, 20 males (55.6%), 16 females (44.4%), and 22 (61.1%) had positive family history of ET. All patients had bilateral nearly symmetrical hands tremor, 6 (16.7%) had head tremor, 5 (13.9%) had voice tremor, and 4 (11.1%) had lower limbs tremor. The mean TETRAS was 37.7 ± 11.1, disease duration was 13.4 ± 4.4 years, 24 (66.7%) were propranolol responsive, and 12 (33.3%) had weak response mainly those with head, voice, and lower limb tremors.
The results of the present study showed highly significant decrease of MoCA scale in ET patients compared to that in HCS with p < 0.001. Regarding the speech MMN, 10 (27.8%) of ET patients had absent evoked potential compared to none of the HCS. Patients with evoked responses showed highly significant prolongation of the latencies and reduction of the amplitude compared to HCS with p values < 0.001. Absent responses and higher MMN abnormalities were present among those with older ages, longer disease duration, and increased TETRAS (Table 1).
The results showed statistically significant increased depressive symptoms and decreased AADLs of ET patients compared to HCS with p value 0.004 and 0.003, respectively (Table 1). At the same time, analysis of patients’ complaints showed that 24 (66.7%), 22 (61.1%), 5 (13.9%), and 2 (5.6%) suffered subjective cognitive decline, depressive symptoms (sense of sadness and hopelessness), balance problems, and smell dysfunctions respectively.
Regarding the results of CDP, there were significant decreases in VIS and VEST ratios of ET patients compared to HCS (p values < 0.001) while SOM ratio showed non-significant difference (p value = 0.149) (Table 1, Fig. 1).

Computerized dynamic posturography sensory analysis ratios of an essential tremor patient showing impaired visual and vestibular inputs with normal somatosensory balance systems
The present study showed significant reduction in each of TSST, ISST, DSST, and TDI in ET patients compared to HCS with p values 0.001, 0.001, 0.004, and 0.001, respectively. Regarding the results of TDI sum score, 9 (25%) ET patients had normal smelling performance and 27 (75%) were hyposmic compared to 17 (70.8%) and 7 (29.2%) for HCS, respectively. None of the included subjects had functional anosmia with TDI ≤ 15 points (Table 1).
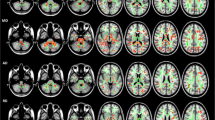
Regarding the DTT data, the results revealed highly significant reductions in mean FA for CST, TCC, and MCP of ET patients compared to HCS with p values < 0.001. On the other hand, the studied tract densities showed non-significant differences between ET patients and HCS with p values > 0.05 (Table 1, Fig. 2).

Diffusion tensor tractography of an included essential tremor patient a corticospinal, b middle cerebellar peduncle, and c thalamo-cortical tractography. FA: fractional anisotropy
The VIS and VEST, CDP as well as examined tracts FA were lower in patients with positive family history of ET, propranolol response, and/or those with additional head, voice, or lower limb tremors. In contrast, MoCA scale, auditory MMN, and SST had no relations to such variables.
Correlation analysis data revealed that MoCA as well as VEST were negatively correlated with disease duration and TETRAS, but positively correlated with AADLs (Fig. 3). At the same time, MADRS as well as MMN latency showed positive correlation with disease duration and TETRAS, but negative correlation with AADLs. On the other hand, TDI showed non-significant correlation with each of disease duration, TETRAS, and AADLs.

Negative correlation between the essential tremor rating assessment scale and each of Montreal cognitive assessment scale (left) as well as vestibular computerized dynamic posturography ratio (right)
The correlation analysis of DTT results showed significant negative correlation between tremor severity (TETRAS) and each of MCP and TCC, FA with p values 0.001 and 0.004, respectively. On the other hand, TCC, FA showed no correlation with each of MADRS, TDI, and MMN (amplitude and latency as well as CDP (VIS and VEST) with p values > 0.05. The only NMM parameter, which was positively correlated with TCC, FA was the MoCA scale (p value 0.008) (Table 2).
Discussion
The present study showed that ET patients exhibit a variety of cognitive, mood, olfactory, and balance impairments exceeding their age- and sex-matched counterparts pointing to the multi-systemic neurological nature of the disorder which affects a wide range of brain areas. This result is passing with the works of Louis, 2019 [13] as well as Soto and Fasano, 2020 [14] who stated that ET is no longer considered as a benign monosymptomatic illness with isolated postural tremor but a slowly progressive neurodegenerative disorder with a variety of motor and non-motor manifestations due to enhanced brain biological aging.
The results revealed that the most common non-motor symptoms of ET patients were subjective cognitive decline and mild depressive symptoms while most patients were not aware of their olfactory or balance problems except after objective assessment. Lack of awareness to the existence of non-tremorgenic dysfunctions is most probably related to their very slow rate of progression as well as cultural believes that these manifestations were attributed to the effect of physiological brain aging. These results are in harmony with the study of Azar and colleagues, 2017 [15] who stated that, despite the great negative impacts of ET non-motor manifestations on the quality of life, many patients are unaware of their existence.
The study showed higher incidence of mild cognitive impairment among ET patients than their age- and sex-matched peers. At the same time, the abnormal auditory MMN-evoked response reflects impaired working memory, attentional switch as well as automatic pre-attentive discrimination of acoustic changes. These results are passing with the work of Meyers and colleagues, 2019 [16] as well as Novellino and colleagues, 2020 [17] who demonstrated greater cognitive decline not only among ET patients but also their 1st degree relatives. They also identified hippocampal microstructural damage correlated with the ET-associated cognitive impairment and make it as a risk for dementia. On the other hand, Medeiros and colleagues, 2016 [18] found non-significant diminution of the global cognitive functions in ET patients compared to healthy control possibly due to the wide age range of their included patients beside recruitment of young ET patients with short disease duration.
The present work revealed that a great proportion of ET patients experienced depressive symptoms with feeling of sadness, helplessness, and hopelessness. These mood disturbances had very mild positive correlation with the tremor severity but greatly impair patients’ ADLs. These data are in accordance with the study of Cersonsky and colleagues, 2019 [19] who demonstrated high demoralization feelings and psychological distress in ET patients even in those with mild tremor disability scores.
Regarding olfactory performance, the results showed mild hyposmia in some ET patients greater than expected for age which was not correlated with the disease duration and/or severity. This finding is passing with the work of Giorelli and colleague, 2014 [20] who identified mild olfactory dysfunction in their included ET patients higher than control. On the other hand, Wu and colleague, 2016 [21] revealed non-significant difference regarding olfactory performance in ET patients compared to healthy control. This discrepancy is possibly related to their inclusion of older age group subjects, use different methods of olfactory assessment, and the racial difference in smelling performance.
The results of the present work showed impaired static and dynamic balance control in ET patients evidenced by decreased VIS and VEST, CDP ratio. On the other hand, the SOM ratio was not significantly impaired. Moreover, VEST ratio was negatively correlated with the disease duration and severity while VIS ratio had no such association. All these data point to the increased risk of falls in ET patients and the different pathogenic effect induced by ET on the three sensory components of balance. These results are in accordance with that of Prasad and colleagues, 2018 [22] who concluded that CDP reveals significant balance impairment in ET patients which adds to the growing body evidence of cerebellar involvement in ET.
The study revealed reduces FA in each of CST, MCP, and TCC, DTT of ET patients while tracts density was non-significantly affected pointing to the microstructural connectivity changes induced by ET. These changes include increased heterogenicity of axon FA (myelination) with preserved tract density (fiber number) which results in decreased synchrony of impulses transduction. These results are passing with that of Chung and colleagues, 2013 [23] who identified that ET induces heterogeneous cortical thinning and white matter alteration with a resultant alteration in the rate of disease progression as well as clinical response to propranolol.
The results also showed positive correlation between brain network changes (DTT, mean FA) and each of tremor severity (TETRAS) as well as cognitive impairment (MoCA) while such association was absent with other examined parameters including olfactory, mood, and balance dysfunctions. This information suggests that ET-associated kinetic tremor and cognitive decline may share the same neuroanatomical basis. At the same time, neuropeptides and neuro-circuits involved in olfactory, mood, and balance changes are different. The net result hypothesizes that ET is a multisystem, multi-peptide, and multi-networks brain disorder with each manifestation; either motor or non-motor has its own route of progression. These data may open a small window in solving the mystery of ET heterogenicity which could improve the treatment results. These data are in harmony with that of Tian and colleagues, 2018 [24] as well as Akram colleagues, 2018 [25] who demonstrated an association between brain microstructural and cognitive impairment in ET. They also stated that good assessment of such matrices changes allows for better selective targeting of disrupted networks during deep brain stimulation as well as MRI-guided focused thalamotomy. On the other hand, Sengul and colleagues, 2019 [26] revealed significant correlation between depression severity and DTT parameters including FA. This discrepancy is possibly due to different patients’ demography with enrollment of higher number of female genders, the use of a different depression scale, and DTT measurements in other regions of interest (ROI) including the prefrontal cortex, paralimbic, and limbic structures.
Conclusion
Essential tremor patients exhibit a wide variety of non-tremorgenic manifestations including mood disturbances, cognitive impairment, olfactory dysfunctions, and increased liability to fall which have great negative impacts on the patients’ ADLs beyond that is caused by the postural tremor itself.
Recommendations
The managing physician of ET patients should be vigilant enough to avoid under-estimation of the ET non-motor manifestations and their negative impact on the patients ADLs. These non-motor dysfunctions need specific management protocol apart of tremor treatment for better patients’ quality of lives.
Limitations
Lack of standardized normative data for CDP is considered abnormal when reduction was more than 1.5 times the standard deviation of HCS. Longitudinal follow-up of patients is further needed to determine the value of such non-motor manifestations as prognostic biomarkers for ET progression which will be the objectives of the 2nd phase of this work.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ADLs:
-
Activity of daily livings
- AADLs:
-
Advanced activities of daily living scale
- CDP:
-
Computerized dynamic posturography
- DTI:
-
Diffusion tensor imaging
- DTT:
-
Diffusion tensor tractography
- ET:
-
Essential tremor
- HCS:
-
Healthy control subjects
- MADRS:
-
Montgomery–Åsberg Depression Rating Scale
- MDS:
-
Movement Disorder Society
- MMN:
-
Mismatch negativity
- MoCA:
-
Montreal Cognitive Assessment Scale
- SOM:
-
Somatosensory
- SST:
-
Sniffin’ Sticks Test
- TCC:
-
Thalamo-cortical connectivity
- TDI:
-
Sum of threshold, discrimination and identification
- TETRAS:
-
The Essential Tremor Rating Assessment Scale
- VEST:
-
Vestibular
- VIS:
-
Visual
References
Reich SG. Essential tremor. Med Clin N Am. 2019;103:351–6. https://doi.org/10.1016/j.mcna.2018.10.016.
Lee SM, Kim M, Lee HM, Kwon KY, Koh SB. Non-motor symptoms in essential tremor: comparison with Parkinson's disease and normal control. J Neurol Sci. 2015. https://doi.org/10.1016/j.jns.2015.01.012.
Louis ED, Collins K, Rohl B, Morgan S, Robakis D, Huey ED, et al. Self-reported physical activity in essential tremor: relationship with tremor, balance, and cognitive function. J Neurol Sci. 2016. https://doi.org/10.1016/j.jns.2016.05.034.
Bahnasy WS, Badr MY, Almalt AM, Amer RA, Elshafey RA, Kotait MA. Cognitive functions in essential tremor. Int J Pharm Res Allied Sci. 2017;6(1):227–35.
Cristal AD, Chen KP, Hernandez NC, Factor-Litvak P, Clark LN, Ottman R, et al. Knowledge about essential tremor: a study of essential tremor families. Front Neurol. 2018. https://doi.org/10.3389/fneur.2018.00027.
Bhatia KP, Bain P, Bajaj N, Elble RJ, Hallett M, Louis ED, et al. Consensus statement on the classification of tremors. From the task force on tremor of the International Parkinson and Movement Disorder Society. Mov Disord. 2018. https://doi.org/10.1002/mds.27121.
Elble R, Comella C, Zesiewicz T. Reliability of a new scale for essential tremor. Mov Disord. 2012;27(12):1567–9. https://doi.org/10.1002/mds.25162.
Dias EN, da Silva JV, Pais-Ribeiro JL, Martins T. Validation of the advanced activities of daily living scale. Geriatr Nurs. 2019;40:7–12. https://doi.org/10.1016/j.gerinurse.2018.05.008.
Williams JBW, Kobak KA. Development and reliability of a structured interview guide for the Montgomery-Asberg depression rating scale (SIGMA). Br J Psychiatry. 2008;192(1):52–8. https://doi.org/10.1192/bjp.bp.106.032532.
Massukawa Oda DT, Ganança CF. Computerized dynamic posturography in the assessment of body balance in individuals with vestibular dysfunction. Audiol Commun Res. 2015;20(2):89–95. https://doi.org/10.1590/S2317-64312015000200001469.
Rumeau C, Nguyen DT, Jankowski R. How to assess olfactory performance with the Sniffin’ sticks test. Eur Ann Otorhinolaryngol Head Neck Dis. 2016;133:203–6. https://doi.org/10.1016/j.anorl.2015.08.004.
Chung HW, Chou MC, Chen CY. Principles and limitations of computational algorithms in clinical diffusion tensor MR tractography. Am J Neuroradiol. 2011;32(1):3–13. https://doi.org/10.3174/ajnr.A2041.
Louis ED. The roles of age and aging in essential tremor: an epidemiological perspective. Neuroepidemiology. 2019;52:111–8. https://doi.org/10.1159/000492831.
Soto MCS, Fasano A. Essential tremor: new advances. Clinical Parkinsonism and Related Disorders. 2020;3:100031. https://doi.org/10.1016/j.prdoa.2019.100031.
Azar M, Bertrand E, Louis ED, Huey E, Collins K, Rohl B, et al. Awareness of cognitive impairment in individuals with essential tremor. J Neurol Sci. 2017;377:155–60. https://doi.org/10.1016/j.jns.2017.04.009.
Meyers JH, Hickman R, Cristal AD, Factor-Litvak P, Cosentino S, Louis ED. More unaffected first-degree relatives of essential tremor cases have mild cognitive deficits than age-matched controls. Parkinsonism and Related Disorders. 2019;61:144–50. https://doi.org/10.1016/j.parkreldis.2018.10.030.
Fabiana Novellino F, Roberta Vasta R, Valeria Saccà V, Rita Nisticò R, Maurizio Morelli M, Gennarina Arabia G, et al. Hippocampal impairment in patients with essential tremor. Parkinsonism and Related Disorders. 2020;72:56–61. https://doi.org/10.1016/j.parkreldis.2020.02.006.
Medeiros LMI, de Castro PCF, Felício AC, Queiros BB, Silva SMCA, Ferraz HB, et al. Patients with essential tremor can have manual dexterity and attention deficits with no impairments in other cognitive functions. Arq Neuropsiquiatr. 2016;74(2):122–7. https://doi.org/10.1590/0004-282X20160006.
Cersonsky TEK, Kellner S, Morgan S, Cosentino S, Koo BB, de Figueiredo JM, et al. Demoralization in essential tremor: prevalence, clinical correlates, and dissociation from tremor severity. CNS Spectrums. 2019:1–8. https://doi.org/10.1017/S1092852918001633.
Giorelli M, Bagnoli J, Consiglio L, Lopane M, Zimatore GB, Zizza D, et al. Do non-motor symptoms in Parkinson’s disease differ from essential tremor before initial diagnosis? A clinical and scintigraphic study. Parkinsonism and Related Disorders. 2014;20:17–21. https://doi.org/10.1016/j.parkreldis.2013.09.004.
Wu Y, Wang X, Wang C, Sun Q, Song N, Zhou Y, et al. Prevalence and clinical features of non-motor symptoms of essential tremor in Shanghai rural area. Parkinsonism and Related Disorders. 2016;22:15–20. https://doi.org/10.1016/j.parkreldis.2015.10.617.
Prasad S, Velayutham SG, Reddam VR, Stezin A, Jhunjhunwala K, Pal PK. Shaky and unsteady: dynamic posturography in essential tremor. J Neurol Sci. 2018;385:12–6. https://doi.org/10.1016/j.jns.2017.12.003.
Chung SJ, Kwon H, Lee DK, Hong JY, Sunwoo MK, Sohn YH, et al. Neuroanatomical heterogeneity of essential tremor according to propranolol response. PLoS One. 2013;8(12):e84054. https://doi.org/10.1371/journal.pone.0084054.
Tian Q, Wintermark M, Elias WJ, Ghanouni P, Halpern CH, Henderson JM, et al. Diffusion MRI tractography for improved transcranial MRI-guided focused ultrasound thalamotomy targeting for essential tremor. Neuroimage Clin. 2018;19:572–80. https://doi.org/10.1016/j.nicl.2018.05.010.
Akram H, Dayal V, Mahlknecht P, Georgiev D, Hyam J, Foltynie T, et al. Connectivity derived thalamic segmentation in deep brain stimulation for tremor. Neuroimage Clin. 2018;18:130–42. https://doi.org/10.1016/j.nicl.2018.01.008.
Sengul Y, Otcu H, Ustun I, Sengul HS, Cersonsky T, Alkan A, et al. Neuroimaging depression and anxiety in essential tremor: a diffusion tensor imaging study. Clin Imaging. 2019;58:96–104. https://doi.org/10.1016/j.clinimag.2019.06.016.
Acknowledgements
We would like to thank the neurology, audiology, diagnostic radiology and otolaryngology medical and para-medical staff, Tanta University Hospitals, for their great help in patients’ selection and evaluation.
Consent of publication
Not applicable.
Funding
No funding had been received.
Author information
Authors and Affiliations
Contributions
MEME participated in the study’s design, patients’ selection, statistical analysis, data analysis, references collection, manuscript writing, and revision and final approval. KHR participated in the study’s idea, design, patients’ selection, neurological examination, posturography assessment, statistical analysis, data analysis, references collection, manuscript writing, revision, and final approval. WSB participated in the study’s idea, design, patients’ selection, neurological examination, posturography assessment, statistical analysis, data analysis, references collection, manuscript writing, revision, and final approval. YAE participated in study’s idea and design, patients’ assessment and inclusion, data analysis, statistical analysis, references collection, manuscript writing, revision, and final approval. EASE participated in the study’s idea, design, patients’ selection and evaluation, data analysis, references collection, manuscript revision, and final approval. MOT participated in study’s idea and design, patients’ assessment and inclusion, Sniffin’ Sticks test performance, data analysis, references collection, manuscript writing, revision, and final approval. KMR participated in study’s design, patients’ assessment, DTT performance, manuscript revision, and final approval. MAK participated in study’s idea and design, patients’ assessment and inclusion, mismatch negativity and posturography interpretation, data analysis, statistical analysis, manuscript writing, revision, and final approval. RAA participated in study’s design, patients’ evaluation, inclusion and neuropsychological assessment, statistical analysis, revision, and final approval. SAE participated in the study’s design, patients’ selection, statistical analysis, data analysis, references collection, manuscript writing and revision, and final approval. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
-The manuscript was approved from The Research Ethics Committee and Quality Assurance Unit, Faculty of Medicine, Tanta University.
-The URL: http://tqac.tanta.edu.eg/new-tqac/QualityAssuranceUnit@hotmail.com
-Approval Code: 31129/09/16
-Name of the PI: Wafik Said Bahnasy
-Name of the department: Neuropsychiatry
-Type of the research: Promotion research
-Date of approval: September 2016
-The study’s protocol had permitted by The Research Ethics Committee and Quality Assurance Unit, Faculty of Medicine, Tanta University.
-Participations were voluntary, informed consents were approved by all participants’ guardian, and any possible risks were clarified.
Competing interests
All authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Mismatch negativity
Additional file 2.
Sniffin’ Sticks test
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elhassanien, M.E.M., Rashed, K.H., Bahnasy, W.S. et al. Essential tremor: what is beyond the oscillatory monosymptomatic illness?. Egypt J Neurol Psychiatry Neurosurg 56, 67 (2020). https://doi.org/10.1186/s41983-020-00200-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-020-00200-4