
Abstract
Background
The applicability of dental age estimation has been expanded to meet a variety of medico-legal needs, law enforcement, and disaster victim identification. The objective of this study is to examine the applicability of the Willems method for Indonesian children.
Material and method
A total of 110 panoramic radiographs of the patients (6–14 years old) who met the inclusion criteria were obtained from the Department of Forensic Odontology and Department of Radiology, Universitas Airlangga, Indonesia. Estimated dental age (EDA) was assessed using the Willems method by two blinded examiners. The statistical analysis was carried out using IBM® SPSS® Statistics version 23.0 (IBM, Armonk, NY, USA).
Results and discussion
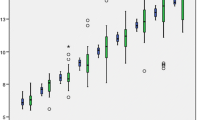
The mean of the chronological age (CA) in this study is 11.30 ± 1.43 years (boys) and 11.65 ± 1.55 years (girls). The overall mean difference between CA and EDA for boys and girls is − 0.08 ± 0.76 and − 0.31 ± 0.97, respectively. This study showed that the mean age difference in girls was more significant than in boys. The growth spurt timing between boys and girls might cause a difference in dental maturation, whereas the onset of the pubertal growth spurt in girls is about 2 years earlier than in boys. In general, girls start and finish their dental development earlier than boys end.
Conclusion
The present study suggests that the dental age estimation methods proposed by Willems can be considered as an applicable method for the children population in Surabaya, both boys and girls. However, a detailed study may be required while applying this approach to the 11–14-year-old girl population in Surabaya, as a substantial underestimation was observed in this community.
Similar content being viewed by others


Introduction
Indonesia is a huge archipelagic country located in the Ring of Fire, which is vulnerable to catastrophes such as volcanic eruption, earthquakes, floods, and tsunamis (Geographic 2019). The National Disaster Management Agency (Badan Nasional Penanggulangan Bencana) has announced that 709 disasters occurred in Indonesia between January and February 2019, with over 396,000 refugees and 130 deaths (Badan Nasional Penanggulangan Bencana (BNPB) 2019).
For over 250 million of the population with a diversity of culture and religions, a suitable identification method is urgently needed to be adopted at an event of a mass disaster in Indonesia (Sahelangi and Novita 2012). Age estimation is one of the ways to identify an individual by classifying the victim according to their estimated ages. Age estimation is also required in the fields of law enforcement, immigrant cases (Pradella et al. 2017), sports competition (Timme et al. 2017), and marriage (Islam 1984).
The value of teeth in assessing individual age is widely accepted in forensic sciences and numerous areas of human life, such as socioeconomic, legal aspects, and dental treatment planning (Koshy and Tandon 1998; Franco et al. 2013). Several studies have been performed on the estimation of human biological age (Cameriere et al. 2004); most of those are focused on skeletal markers (Priya 2017) such as epiphyseal and cranial suture fusions (Ebeye et al. 2016), hand-wrist bones (Benjavongkulchai and Pittayapat 2018), sternoclavicular bones (Ufuk et al. 2016), and dental maturation (Manjunatha and Soni 2014).
The previous studies have demonstrated that the radiograph of hand-wrist and dental development is the most reliable method of assessing the biological age for children and adolescents (Greulich 1959). This study was proposed to analyze the applicability of the Willems dental age estimation method applied in Indonesian children, which is categorized as Mongoloid race.
Material and methods
The present study was conducted under the approval from the Ethics Committee of the Faculty of Dental Medicine, Universitas Airlangga, Indonesia (permit number: 48/KKEPK.FKG/IV/2016). Panoramic radiographs were collected from 110 patients (46 boys and 64 girls; 6–14 years old) who met the following inclusion criteria:
Clear panoramic radiographs
Date of birth and date of the radiographic recording were available
Chronological age between 6 and 14 years old
Indonesian descendants (parents are of the same ethnicity)
The exclusion criteria of this study were as follows:
Patient with orthodontics appliances
Bilateral tooth extraction
Developmental abnormalities or disorders
The subjects were then divided into two groups of age (6–10 and 11–14 years old) in both sexes.
The developmental stage of all seven left mandibular teeth was determined according to the Demirjian classification. If a mandibular tooth on the left side is missing, the corresponding tooth on the right side is used as a substitute. The stage of each tooth was then converted to scores using the Willems score chart and summed up to calculate an estimated dental age (EDA) of the subject (Koshy and Tandon 1998; Willems et al. 2001; Franco et al. 2013). Two observers assessed the tooth developmental stages on panoramic radiographs during two different periods.
All data, both CA and EDA, were then tabulated and analyzed using IBM® SPSS® Statistics version 23.0 (IBM, Armonk, NY, USA). Analysis of the discrepancy between CA and EDA of each group was investigated using paired sample t test, with a confidence interval of 95%.
Results
Out of the 110 subjects, 64 were girls and 46 were boys, 6–14 years old. The inter-examiner agreement test was calculated to attain the reliability of the data, with Cohen’s kappa coefficient < 0.05. The Shapiro-Wilk test was also performed to explain that the data is normally distributed and is adequate for further statistical analysis, p > 0.05.
The independent sample t test was used to calculate the mean age difference between boys and girls, with p = 0.198. The overall mean difference between CA and EDA for boys and girls revealed an underestimation of − 0.08 ± 0.81 and − 0.20 ± 1.00, respectively. Subsequently, the difference between CA and EDA in boys’ and girls’ group was analyzed using the paired sample t test, p = 0.513 for boys and p = 0.121 for girls (Table 1). This result suggests that in general, the underestimation of age was not significant in boys and girls (Table 2).
Further analysis was done by classifying the age groups to 6–10 and 11–14 years old. Overestimation of age was observed in 6–10 years, both boys and girls, without a significant statistical difference, p > 0.05. Underestimation of age was described in 11–14 years, in both sexes. The age difference between CA and EDA in boys was not significant in all ranges of age, whereas in girls, a significant underestimation of age was observed in the range 11–14 years, p = 0.002.
Discussion
Estimating a person’s age is one of the most important aspects of human identification (Ubelaker and Khosrowshahi 2019). Dental age estimation significantly narrows the search possibilities of the suspected victim into the estimated ages and gender (Krishan et al. 2015). This study took place in Surabaya, East Java, Indonesia. We evaluated the applicability of the Willems method for Indonesian children, which are classified as the Mongoloid race, whereas the population of the established method was Caucasian.
In the scope of dental age estimation, the previous study by Olze et al. had reviewed various methods of dental development staging and found that the Demirjian method can define the chronological age accurately (Olze et al. 2005). In spite of that statement, another study suggested that the modification of the Demirjian method proposed by Willems showed higher accuracy in estimating age and has been tested in various populations (Willems et al. 2001, 2012; Grover et al. 2012; Ambarkova et al. 2014; Ye et al. 2014). The Willems method was considered to be applied in the Indonesian children population because of its accuracy, and there was no established dental age estimation method for Indonesian children.
The previous study in Malay children (Mongoloid race) found that the Willems method showed overestimation in age groups of 5 and 15 years, and underestimation in age groups of 10 years in both sexes, without a significant statistical difference (Ismail et al. 2018). Unlike the results of the previous study in Malay children, there was an underestimation of age observed in the present study, both boys and girls. Further statistical analysis suggested that there was no significant difference between CA and EDA in the boys’ group. However, a significant difference was observed in the girls’ group.
The differences in dental maturation between boys and girls that might cause significant mean age difference are more visible in the girls’ group, whereas girls experience earlier growth spurt phase than boys. The growth spurt phase in girls occurs in early birth periods, 6 until 7 years, and 12 to 14 years old. Some literature has discussed that the mean difference of the onset of a pubertal growth spurt in boys and girls is about 2 years earlier for girls (Burstone 1963; de Souza Araujo et al. 2011). A study by Nola (1960) stated that there are remarkable differences in the distribution of tooth calcification and mineralization between sexes. In general, girls begin and end their dental development earlier than boys (Nolla 1960; Chertkow 1980).
A study by Willems in 2001 confirmed the substantial overestimation of the dental age in Belgian Caucasians using the original methods by Demirjian. It claimed that significant overestimation is due in theory to the different rates of dental development in different populations (Willems et al. 2001). Evaluation of dental development was considered as a reliable method for predicting age, as maturation events associated with tooth formation are less variable, and the mineralization of teeth is not affected by the external factors, such as crowding, retention, or early extraction of deciduous teeth (Chertkow and Fatti 1979; Maia et al. 2010; Latić-Dautović et al. 2017). As a developing country with a huge population, socioeconomic and nutritional status may affect the skeletal and dental growth of children in Indonesia (Cameriere et al. 2007).
Routine radiographs for dental treatment such as panoramic and periapical may be used as evidence in the forensic fields. Estimating the dental age in children can be done by defining the calcification and mineralization of teeth. Some combined methods, such as hand-wrist radiograph, might be necessary for further consideration and investigation of the dental age estimation.
Conclusion
The results of this study suggest that the dental age estimation method proposed by Willems can be applied accurately to the boy population in Surabaya, as there was no significant statistical difference. However, a thorough analysis might be necessary while applying this method to the girl population in Surabaya. A small number of subjects have been thought as one limitation in this study; hence, further studies with more samples will improve the reliability of the Willems method in Indonesia.
Availability of data and materials
Not applicable.
Abbreviations
- CA:
-
Chronological age
- EDA:
-
Estimated dental age
References
Ambarkova V, Galić I, Vodanović M et al (2014) Dental age estimation using Demirjian and Willems methods: cross sectional study on children from the Former Yugoslav Republic of Macedonia. Forensic Sci Int. https://doi.org/10.1016/j.forsciint.2013.10.024
Badan Nasional Penanggulangan Bencana (BNPB) (2019) Infografis Kejadian Bencana. https://bnpb.go.id/publikasi/info-bencana/info-bencana-februari-2019.html. Accessed 14 Nov 2019
Benjavongkulchai S, Pittayapat P (2018) Age estimation methods using hand and wrist radiographs in a group of contemporary Thais. Forensic Sci Int. https://doi.org/10.1016/j.forsciint.2018.03.045
Burstone CJ (1963) Process of maturation and growth prediction. Am J Orthod. https://doi.org/10.1016/0002-9416(63)90220-3
Cameriere R, Ferrante L, Cingolani M (2004) Precision and reliability of pulp/tooth area ratio (RA) of second molar as indicator of adult age. J Forensic Sci 49:1–5. https://doi.org/10.1520/JFS2004125
Cameriere R, Flores-Mir C, Mauricio F, Ferrante L (2007) Effects of nutrition on timing of mineralization in teeth in a Peruvian sample by the Cameriere and Demirjian methods. Ann Hum Biol 34:547–556. https://doi.org/10.1080/03014460701556296
Chertkow S (1980) Tooth mineralization as an indicator of the pubertal growth spurt. Am J Orthod. https://doi.org/10.1016/0002-9416(80)90226-2
Chertkow S, Fatti P (1979) The relationship between tooth mineralization and early radiographic evidence of the ulnar sesamoid. Angle Orthod 49:282–288. https://doi.org/10.1043/0003-3219(1979)049<0282:TRBTMA>2.0.CO;2
de Souza Araujo MT, A De A C-S, AFJ d M (2011) Clinical and radiographic guidelines to predict pubertal growth spurt. Dental Press J Orthod. https://doi.org/10.1590/S2176-94512011000500015
Ebeye OA, Eboh DE, Onyia NS (2016) Radiological assessment of age from epiphyseal fusion at the knee joint. Anatomy. https://doi.org/10.2399/ana.15.020
Franco A, Thevissen P, Fieuws S et al (2013) Applicability of Willems model for dental age estimations in Brazilian children. Forensic Sci Int 231:401.e1–401.e4. https://doi.org/10.1016/j.forsciint.2013.05.030
Geographic N (2019) Ring of Fire. https://www.nationalgeographic.org/encyclopedia/ring-fire/. Accessed 14 Nov 2019
Greulich WWPS (1959) Radiographic atlas of skeletal development of the hand and wrist, 2nd edn. Stanford Univ. Press, Stanford
Grover S, Marya CM, Avinash J, Pruthi N (2012) Estimation of dental age and its comparison with chronological age: accuracy of two radiographic methods. Med Sci Law. https://doi.org/10.1258/msl.2011.011021
Islam MN (1984) Estimation of mean age at first marriage: use of a simple mathematical model. Rural Demogr 27:39–59
Ismail AF, Othman A, Mustafa NS et al (2018) Accuracy of different dental age assessment methods to determine chronological age among Malay children. J Phys Conf Ser 1028:012102. https://doi.org/10.1088/1742-6596/1028/1/012102
Koshy S, Tandon S (1998) Dental age assessment: the applicability of Demirjian’s method in South Indian children. Forensic Sci Int. https://doi.org/10.1016/S0379-0738(98)00034-6
Krishan K, Kanchan T, Garg AK (2015) Dental evidence in forensic identification - an overview, methodology and present status. Open Dent J 9:250–256. https://doi.org/10.2174/1874210601509010250
Latić-Dautović M, Nakaš E, Jelešković A et al (2017) Cameriere’s European formula for age estimation: a study on the children in Bosnia and Herzegovina. South Eur J Orthod Dentofac Res. https://doi.org/10.5937/sejodr4-15528
Maia MCG, Martins M d GA, Germano FA et al (2010) Demirjian’s system for estimating the dental age of northeastern Brazilian children. Forensic Sci Int 200:177.e1–177.e4. https://doi.org/10.1016/j.forsciint.2010.03.030
Manjunatha BS, Soni N (2014) Estimation of age from development and eruption of teeth. J Forensic Dent Sci. https://doi.org/10.4103/0975-1475.132526
Nolla CA (1960) The development of the permanent teeth. J Dent Child 27:254–66
Olze A, Bilang D, Schmidt S et al (2005) Validation of common classification systems for assessing the mineralization of third molars. Int J Legal Med. https://doi.org/10.1007/s00414-004-0489-5
Pradella F, Pinchi V, Focardi M et al (2017) The age estimation practice related to illegal unaccompanied minors immigration in Italy. J Forensic Odontostomatol 35:141–148
Priya E (2017) Methods of skeletal age estimation used by forensic anthropologists in adults: a review. Foresic Res Criminol Int J. https://doi.org/10.15406/frcij.2017.04.00104
Sahelangi P, Novita M (2012) Role of Dentists in Indonesian Disaster Victim Identification Operations: Religious & Cultural Aspects. J Forensic Odontostomatol 30:11
Timme M, Steinacker JM, Schmeling A (2017) Age estimation in competitive sports. Int J Legal Med 131:225–233
Ubelaker DH, Khosrowshahi H (2019) Estimation of age in forensic anthropology: historical perspective and recent methodological advances. Forensic Sci Res 4:1–9. https://doi.org/10.1080/20961790.2018.1549711
Ufuk F, Agladioglu K, Karabulut N (2016) CT evaluation of medial clavicular epiphysis as a method of bone age determination in adolescents and young adults. Diagnostic Interv Radiol. https://doi.org/10.5152/dir.2016.15355
Willems G, Ramanan N, Thevissen P, Fieuws S (2012) Dental age estimation in Japanese individuals combining permanent teeth and third molars. J Forensic Odontostomatol 30 (2):34–39
Willems G, Van Olmen A, Spiessens B, Carels C (2001) Dental age estimation in Belgian children: Demirjian’s technique revisited. J Forensic Sci 46:15064J. https://doi.org/10.1520/JFS15064J
Ye X, Jiang F, Sheng X et al (2014) Dental age assessment in 7-14-year-old Chinese children: comparison of Demirjian and Willems methods. Forensic Sci Int. https://doi.org/10.1016/j.forsciint.2014.07.027
Acknowledgements
Not applicable
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
AK, SRA, and MIM contributed to the data collection and dental age assessment of the subjects. MSM, HU, AC, and AS are the supervisor of the present study. AK, MIM, and BNR contributed to the drafting of the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval has been obtained from the Ethics Committee of the Faculty of Dental Medicine, Universitas Airlangga (KKEPK), Indonesia (permit number: 48/KKEPK.FKG/IV/2016), in accordance with the International Ethical Guidelines for Biomedical Research Involving Human Subjects by The Council for International Organizations of Medical Sciences (CIOMS).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Kurniawan, A., Agitha, S.R.A., Margaretha, M.S. et al. The applicability of Willems dental age estimation method for Indonesian children population in Surabaya. Egypt J Forensic Sci 10, 5 (2020). https://doi.org/10.1186/s41935-020-0179-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41935-020-0179-6