
Abstract
Background
Colorectal cancer (CRC) is a neoplasia with high incidence and mortality rates. It had been suggested that the inflammatory response is an important CRC prognostic factor. The disordered and accelerated proliferation of neoplastic cells decreases the oxygen and nutrient supply, generating a microenvironment characterized by hypoxia, necrosis and inflammation. This study aimed to evaluate the impact of factors associated with hypoxia, such as HIF1A (hypoxia-inducible factor 1-alpha) and VEGF (vascular endothelial growth factor), and with lipid metabolism, including PPARG (peroxisome proliferator-activated receptor-gamma), LXRA (liver X receptor-alpha) and LXRB (liver X receptor-beta), on the overall survival (OS) of CRC patients.
Methods
This was a cohort study of 101 patients with high-risk stage II-III (TNM) CRC located above the peritoneal reflection. They were treated between 1990 and 2004 at the AC Camargo Cancer Center. Immunohistochemical analyses of HIF1A, VEGF, PPARG, LXRA and LXRB protein expression were performed using tissue microarrays (TMAs).
Results
There was an association between the presence of vascular invasion and the lack of VEGF expression (p = 0.028) as well as with positive HIF1A expression and lymphatic invasion (p = 0.045). The 5-year and 10-year OS rates were 76.6% and 60.2%, respectively. Patients with PPARG-positive tumors had a higher OS (p = 0.018). There were no correlations between the positive expression of VEGF, HIF1A, LXRA or LXRB and OS. The Cox regression model demonstrated that the risk of death was 2.72-fold higher in patients with PPARG-negative tumors (95% CI = 1.08–6.85).
Conclusion
The PPARG expression was an independent prognostic factor for CRC tumors and might be used for risk stratification to stage II and stage III CRC patients.
Similar content being viewed by others
Background
Colorectal cancer (CRC) is a neoplasia with high incidence and mortality rates [1, 2], and the elucidation of the mechanisms of carcinogenesis and tumor progression has contributed to the development of novel treatment strategies. The disordered and accelerated proliferation of neoplastic cells during tumorigenesis and tumor progression reduces oxygen and nutrient supply, thereby generating a microenvironment characterized by hypoxia, necrosis and inflammation. Hypoxia promotes inflammation, and the inflamed tissues become even more hypoxic. Under normal oxygen concentrations, HIF (hypoxia-inducible factor) is inactive; however, HIF1A (hypoxia-inducible factor 1-alpha) is activated in response to hypoxia in the tumor microenvironment [1,2,3].
In addition to hypoxia, low local glucose levels, low pH, high levels of oxygen free radicals, and the influx of neutrophils and macrophages are features of inflamed tissues. Interdependence between innate immunity and hypoxic responses has been demonstrated, where by HIF regulates innate immunity by promoting the bactericidal activity of phagocytic cells and stimulating the immune response in dendritic cells, mast cells and macrophages [4].
Low cellular oxygen levels are a key stimulatory signal for angiogenesis. VEGF (vascular endothelial growth factor) is one of the major hypoxia-regulated angiogenic factors [1]. HIF1A activates VEGF expression, and together they regulate angiogenesis [5].
PPARs (peroxisome proliferator-activated receptors) and LXRs (liver X receptors) are also involved in inflammation and immunity [6, 7]. PPARs are nuclear receptors that regulate the transcriptional activity of factors involved in inflammatory and immune responses. PPARG (peroxisome proliferator-activated receptor gamma) is expressed in monocytes, macrophages, T cells, dendritic cells, skeletal muscle cells, adipocytes and gastrointestinal epithelial cells. It is involved in several biological processes, including lipid and glucose homeostasis, adipocyte differentiation and inflammation [6, 7].
LXRs are nuclear hormone receptors that regulate the metabolism of cholesterol and fatty acids as well as the innate immune response, wherein they modulate the release of IL (interleukin) and TNF (tumor necrosis factor) by macrophages [8]. Synthetic LXR agonists that promote tumor cell apoptosis were shown to inhibit tumor growth in breast and prostate cancer studies [9]. Furthermore, it has been demonstrated that LXRA (liver X receptor alpha) activation inhibits dendritic cell maturation and then compromises the antitumor immune response [10]. Interestingly, both LXRA and PPARG increase VEGF expression in a HIF1A-independent manner [11, 12].
Although the expression of HIF1A and VEGF and the role of PPARs and LXRs have been assessed in some tumor types, there have been few studies demonstrating their clinical value in solid tumors [5]. In the present study, immunohistochemical analyses were performed to evaluate the expression of factors associated with hypoxia (HIF1A and VEGF) and lipid metabolism (PPARG, LXRA, and LXRB) and to ascertain their association with prognosis in CRC patients.
Methods
Retrospective analysis was performed on a cohort of patients with high-risk stage II and stage III CRC located above the peritoneal reflection who were treated from 1990 to 2004. Patients with inflammatory bowel disease or hereditary CRC were excluded. The study cohort consisted of 101 consecutive patients who had available samples; from this total, 49 patients presented with high-risk stage II CRC (pT4, CEA > 10 ng/ml, G2/G3, presence of lymphatic and vascular invasion and/or the presence of perineural invasion), and 52 patients presented with stage III CRC.
To construct the Tissue Microarray (TMA), sections were stained with hematoxylin-eosin (HE) and histologically examined by light microscopy to identify and mark the representative tumor areas. Then, the chosen area was marked on the corresponding paraffin block (donor block). Using the tissue microarrayer, tissue cylinders with a diameter of 1.0 mm were punched from these marked areas and transferred into a new paraffin block (recipient block). Each case was analyzed in duplicate: two cylinders were obtained in two distinct and representative tumor areas for each case. Histological sections of these blocks were obtained for immunohistochemistry. A coordinate system from Excel tables was used to determine and precisely identify the cases within the TMA, and a liver tissue cylinder served as the reference.
The following specific antibodies were used in this study: anti-LXR alpha (clone PPZ0412, Abcam, Cambridge, MA, USA; 1:1000; nuclear staining pattern; control = normal colon), anti-LXR beta (clone K8917, Perseus Proteomics, Cambridge, MA, USA; 1:1600; nuclear staining pattern; control = normal colon), anti-PPAR gamma (clone H1a67, Neomarkers, Fremont, CA, USA; 1:100; nuclear staining pattern; control = normal lung), anti-HIF1 alpha (polyclonal, Abcam, Cambridge, MA, USA; 1:50; cytoplasmic and nuclear staining patterns; control = breast cancer), and anti-VEGF (clone VGI, Dako, Tokyo, Japan; 1:100; cytoplasmic staining pattern; control = tonsil).
The staining was evaluated by means of light microscopic examination and interpreted by pathologist who was blinded to the clinical information. The results were determined using Rajkumar score, resulting from the product of the score for the fraction of positive cells (range, 0 to 4 [0, < 10% of positively stained cells; 1, 10% to 25%; 2, 26% to 50%; 3, 51% to 75%; and 4, > 75%]) and the score for staining intensity (range, 0 to 3). Tumor cases with scores of 8 or higher were classified as positive and the ones with scores lower than 8 as negative [13].
Descriptive statistics were used to characterize the cohort. Chi-square and Fisher’s exact tests were used to analyze the associations, Student’s t-test and the Mann-Whitney test were used to compare the continuous variables, and ANOVA and the Kruskal-Wallis test were used to compare the continuous variables across multiple groups. The Kaplan-Meier method was used to estimate the probabilities of overall survival (OS) and disease-free survival (DFS). The log-rank test was used to analyze the differences between the survival curves. Multivariate analysis was used to predict the combined effect of independent variables using a Cox proportional hazards model. The significance level was set at 5% for all the statistical analyses.
This study was approved by the ethics committee of the institution (number 1459/10).
Results
The distribution of the clinical and histopathological variables and the frequency of HIF1A, VEGF, PPARG, LXRA and LXRB expression are shown in Table 1 and Fig. 1.

Photomicrograph of colon adenocarcinoma showing invasive atypical gland (HE) and positive tumor cells for HIF1A, LXRA, LXRB, PPARG and VEGF (original magnification of 400× for all pictures)
There was an inverse correlation between the absence of VEGF expression and the presence of vascular invasion (p = 0.028), and HIF1A expression was correlated with the presence of lymphatic invasion (p = 0.045). No correlations were observed between VEGF or HIF1A expression and clinical stage, histological grade or perineural invasion (Table 2).
The median follow-up was 78 months (range, 0.3 to 237 months), with a median OS of 34.6 months and a median DFS of 21 months (range, 7.4 to 62.8 months). The 5-year and 10-year OS rates were 76.6% and 60.2%, respectively, and the 5-year and 10-year DFS rates were 79.3% and 66.4%, respectively.
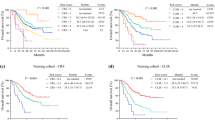
Patients with PPARG-positive tumors had increased 5-year and 10-year OS rates compared with patients with PPARG-negative tumors (83.5% vs. 70.4% and 75.9% vs. 52.6%, respectively; p = 0.018, Fig. 2). There were no correlations between VEGF, HIF1A, LXRA, or LXRB expression and OS (Table 3).

Kaplan − Meier estimate and cumulative incidence curve of the overall survival of colorectal cancer patients with regard to the expression of PPARG
The multivariate Cox regression analysis revealed that the following independent prognostic variables were associated with the risk of death: age > 65 years (relative risk (RR) 2.05; 95% confidence interval (CI) 0.93–4.50); positive lymph nodes (pN+) (RR 2.51; 95% CI 1.10–5.72), lymphatic invasion (RR 2.62; 95% CI 1.23–5.61), and perineural invasion (RR 2.51; 95% CI 1.13–5.57). The risk of death was 2.72-fold higher in patients with PPARG-negative tumors (RR 2.72; 95% CI 1.08–6.85) (Table 4, Fig. 3).

Kaplan − Meier estimate and cumulative incidence curve of the disease-free survival of colorectal cancer patients with regard to the expression of PPARG
Discussion
There is evidence that the inflammatory response is associated with prognosis in CRC patients; this prompted an analysis of the expression of signaling molecules and/or transcription factors that modulate the inflammatory response as well as hypoxia (HIF1A and VEGF) or lipid metabolism (PPARG, LXRA and LXRB) [4, 6, 7, 9].
HIF1 is an important transcriptional regulator involved in regulating energy metabolism and the adaptation to cellular stress caused by oxygen deficiency. HIF1 is composed by two units, HIF1 alpha (HIF1A) and HIF1 beta (HIF1B). Under normal oxygen conditions, HIF1A expression is undetectable. [1] In our study, HIF1A expression was observed in the majority of the CRCs and was associated with lymphatic invasion. However, the association between HIF1A expression and high risk of death or reduced survival was not found. HIF1A has been showed to be over-expressed in various human malignant tumors as a result of intratumoral hypoxia associating with treatment failure and higher mortality of the patients [1, 5]. Considering the fact that higher HIF1A levels promote tumor progression its inhibition may represent an intriguing therapeutic target for these patients.
Angiogenesis is a complex process, which involves the formation of new vessels from the preexisting blood vessels. These new vessels supply nutrients to the tumor, promoting cancer survival, growth, and dissemination. This process involves numerous factors; VEGF and its signaling are considered as one of the most important [14].
VEGF has been the most widely studied biomarker in predicting response to antiangiogenic treatment. Associations between the efficacy of antiangiogenic treatments and circulating VEGF levels have been reported in several phase II studies. These have shown that the elevated levels of VEGF have been associated with a poor prognosis but do not predict response to antiangiogenic treatments, such as bevacizumab [15,16,17]. In our study we found VEGF expression in more than 80% of the CRC samples, and there was no association between VEGF expression and survival.
PPARs comprise a family of nuclear receptors with several functions, including regulating the immune response and trigger antiproliferative and pro-apoptotic signaling in epithelial cells [6, 7]. Fujisawa et al. demonstrated that inhibiting PPARG expression with a selective antagonist promoted the formation of intestinal colonic polyps in rats [18].
In our study, patients with PPARG-negative tumors had a decreased OS and DFS. The multivariate analysis revealed that the risk of death was 2.72-fold higher in patients with PPARG-negative tumors, suggesting that the absence of PPARG expression is a poor prognostic factor for CCR patients. Consistent with our results, Ogino et al. [19] and Pancione et al. [20] also detected a correlation between the lack of PPARG expression and poor prognosis in patients with CRC. Furthermore, a study performed by Pancione et al. [21] demonstrated that lower PPARG levels were associated with increased macrophage infiltration and increased expression of cyclooxygenase-2 and NK-κB, reinforcing the role of PPARG in the antitumor immune response.
Protective functions have consistently been reported for LXRs in a variety of diverse cancers. Specific LXR activation leads to anti-proliferative effects in CRC cells [22]. Several mechanisms have been proposed for these LXR- mediated effects. For instance, cell cycle inhibiton [23, 24], induction of apoptosis [25], and ligand deprivation have all been described [26]. Our results showed expression of LXRA in less than 50% of the cases. In the other hand, LXRB expression was observed in almost all cases. These results are intriguing and further studies are needed to identify the related molecular mechanisms and their relationship to colorectal carcinogenesis.
Conclusion
The role of the inflammatory response markers as a prognostic factor in patients with CRC is of great interest due to the high incidence of this disease and the large number of affected patients. Among the studied biomarkers (HIF1A, VEGF, PPARG, LXRA and LXRB), the PPARG expression was an independent prognostic factor in patients with stage II and high-risk stage III colorectal cancer.
References
Benizri E, Ginouvès A, Berra E. The magic of the hypoxia-signaling Cascade. Cell Mol Life Sci. 2008;65:1133–49.
Eltzschig HK, Carmeliet P. Hypoxia and inflammation. N Engl J Med. 2011;364(7):656–65.
Kaelin WG Jr, Ratcliffe PJ. Oxygen sensing by metazoans: the central role of the HIF Hydroxylase pathway. Mol Cell. 2008;30:393–402.
Nizet V, Johnson RS. Interdependence of hypoxic and innate immune responses. Nat Rev Immunol. 2009;9:609–17.
Cao D, Hou M, Guan YS, Jiang M, Yang Y, Gou HF. Expression of HIF-1alpha and VEGF in colorectal cancer: association with clinical outcomes and prognostic implications. BMC Cancer. 2009;9:432.
Fijisawa T, Sugiyama M, Tomimoto A, et al. Inhibition of peroxisome proliferator-activated receptor gamma promotes tumorigenesis through activation of the betacatenin / T cell factor (TCF) pathway in the mouse intestine. J Pharmacol Sci. 2008;108:535–44.
McAlpine CA, Barak Y, Matise I, Cormier RT. Intestinal-specific PPARgamma deficiency enhances tumorigenesis in ApcMin/+ mice. Int J Cancer. 2006;119:2339–46.
Bensinger SJ, Tontonoz P. Integration of metabolism and inflammation by lipid-activated nuclear receptors. Nature. 2008;454:470–7.
Chuu CP, Kokontis JM, Hiipakka RA, Liao S. Modulation of liver X receptor signaling as novel therapy for prostate cancer. J Biomed Sci. 2007;14:543–53.
Villablanca EJ, Raccosta L, Zhou D, et al. Tumor-mediated liver X receptor-alpha activation inhibits CC Chemokine Receptor-7 expression on Dendritic cells and dampens antitumor responses. Nat Med. 2010;16(1):98–105.
Walczak R, Joseph SB, Laffitte BA, et al. Transcription of the vascular endothelial growth factor gene in macrophages is regulated by liver X receptors. J Biol Chem. 2004;279(11):9905–11.
Röhrl C, Kaindl U, Koneczny I, et al. Peroxisome-Proliferator-activated receptors γ and β/δ mediate vascular endothelial growth factor production in colorectal tumor cells. J Cancer Res Clin Oncol. 2011;137(1):29–39.
Rajkumar T, Stamp GW, Pandha HS, et al. Expression of the type 1 tyrosine kinase growth factor receptors EGF receptor, c-erbB2 and c-erbB3 in bladder cancer. J Pathol. 1996;179:381–5.
Al-Husein B, Abdalla M, Trepte M, Deremer DL, Somanath PR. Anti-angiogenic therapy for cancer: an update. Pharmacotherapy. 2012;32(12):1095–111.
Mass RD, Sarkar S, Holden SN, Hurwitz H. Clinical benefit from bevacizumab (BV) in responding (R) and nonresponding (NR) patients (pts) with metastatic colorectal cancer (mCRC). J Clin Oncol. 2005;23:S249–249.
Poon RT, Fan ST, Wong J. Clinical implications of circulating angiogenic factors in cancer patients. J Clin Oncol. 2001;19:1207–25. [PubMed]
Jubb AM, Hurwitz HI, Bai W, et al. Impact of vascular endothelial growth factor-a expression, thrombospondin-2 expression, and microvessel density on the treatment effect of bevacizumab in metastatic colorectal cancer. J Clin Oncol. 2006;24:217–27.
Fujisawa T, Sugiyama M, Tomimoto A, et al. Inhibition of Peroxisome Proliferator-activated receptor gamma promotes tumorigenesis through activation of the Beta-catenin/T cell factor (TCF) pathway in the mouse intestine. J Pharmacol Sci. 2008;108:535–44.
Ogino S, Shima K, Baba Y, et al. Colorectal cancer expression of Peroxisome Proliferator-activated receptor gamma (PPARG, PPAR gamma) is associated with good prognosis. Gastroenterology. 2009;136(4):1242–50.
Pancione M, Sabatino L, Fucci A, et al. Epigenetic silencing of Peroxisome Proliferator-activated receptor γ is a biomarker for colorectal cancer progression and adverse Patients’ outcome. PLoS One. 2010;5(12):e14229.
Pancione M, Forte N, Sabatino L, et al. Reduced Beta-catenin and Peroxisome Proliferator-activated receptor-gamma expression levels are associated with colorectal cancer metastatic progression: correlation with tumor-associated macrophages, Cyclooxygenase 2, and patient outcome. Hum Pathol. 2009;40(5):714–25.
Savic D, Ramaker RC, Roberts BS, Dean EC, Burwell TC, Meadows SK, Cooper SJ, Garabedian MJ, Gertz J, Myers RM. Distinct gene regulatory programs define the inhibitory effects of liver X receptors and PPARG on cancer cell proliferation. Genome Med. 2016;8(1):74.
Vedin LL, Gustafsson JA, Steffensen KR. The oxysterol receptors LXRalpha and LXRbeta suppress proliferation in the colon. Mol Carcinog. 2013;52(11):835–44.
Fukuchi J, Kokontis JM, Hiipakka RA, Chuu CP, Liao S. Antiproliferative effect of liver X receptor agonists on LNCaP human prostate cancer cells. Cancer Res. 2004;64(21):7686–9.
Pommier AJ, Alves G, Viennois E, Bernard S, Communal Y, Sion B, Marceau G, Damon C, Mouzat K, Caira F, et al. Liver X receptor activation downregulates AKT survival signaling in lipid rafts and induces apoptosis of prostate cancer cells. Oncogene. 2010;29(18):2712–23.
Lee JH, Gong H, Khadem S, Lu Y, Gao X, Li S, Zhang J, Xie W. Androgen deprivation by activating the liver X receptor. Endocrinology. 2008;149(8):3778–88.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Council for Scientific and Technological Development (CNPq; Process Number 301603/2012–0) and by the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP; Process Number 2010/18843–6).
Availability of data and materials
Please contact author for data requests.
Research support
This study was partially supported by the National Council for Scientific and Technological Development - CNPq (301,603/2012–0). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. No additional external funding was received for this study.
Author information
Authors and Affiliations
Contributions
AC conceptualization, data collection, formal analysis, investigation, methodology, writing the original draft and the final version of the manuscript, review and editing. PRSF and SAJ: conceptualization, data curation, clinical data, writing the original draft and final version of the manuscript, revised and edited. MDB: conceptualization, data curation, histopathological analysis, tissue macrodissection, review and editing the final version of the manuscript. VL, FSCO, FOF, WTN, RMS: data collection, review and editing the final version of the manuscript. AL: Conceptualization, funding acquisition, investigation, project administration, resources, supervision, writing the original draft, revised and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of the institution - A.C. Camargo Cancer Center (number 1459/10).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
da Costa, A.C., Filho, P.R.S., Júnior, S.A. et al. Prognostic value of factors associated with hypoxia and lipid metabolism in patients with colorectal cancer. Appl Cancer Res 37, 44 (2017). https://doi.org/10.1186/s41241-017-0050-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41241-017-0050-8