
Abstract
Background
Diabetes mellitus is the leading cause of end-stage renal disease. Monitoring and controlling normal blood sugar levels play a critical role in slowing the progression of micro- and macrovascular complications of diabetes. This study was conducted to measure glycaemic control and diabetes-related knowledge in diabetic patients on maintenance haemodialysis and to assess any relationship between these two variables.
Methods
This cross-sectional study was conducted at six dialysis centres in the north of the West Bank. Blood samples were collected to measure glycated haemoglobin (HbA1c) levels, while the Michigan Diabetic Knowledge Test (MDKT) was employed as a measure tool of diabetes-related knowledge. Patients were also asked to fill in a questionnaire in order to determine their sociodemographic characteristics. Finally, univariate analyses were used to measure the associations between the clinical and sociodemographic data, and diabetes knowledge and glycaemic control.
Results
A total of 147 haemodialysis patients with diabetes were included in this study. The mean age of the cohort was 60.12 (SD = 10.28). Males accounted for 51.7% of the cohort. The HbA1c levels (%) and MDKT scores were 6.89 ± 1.72 and 9.19 ± 1.7 (mean ± SD), respectively. 36.1% of the patients had poor glycemic control. The study showed that residency and household income were associated with diabetes knowledge (P < 0.05). However, the study did not show a significant association between diabetes-related knowledge and glycaemic control overall, nor did it show a significant association between the clinical and sociodemographic factors and glycaemic control (P > 0.05).
Conclusions
This study showed that patients living in refugee camps as well as those with low income had low diabetes-related knowledge and needed extra care. This study also revealed that a relatively high proportion of diabetic patients on maintenance haemodialysis suffered from poor glycemic control. Here, we recommend to put greater emphasis on better diabetes-related knowledge as a means to achieve better diabetes care with improved glycemic control for all haemodialysis patients
Similar content being viewed by others

Background
Type 2 diabetes mellitus is a serious long-term illness that can affect the health system of communities in general and the personal health of patients in particular [1, 2]. It causes many complications that can affect several organs in the human body, such as the brain, heart, eyes and kidneys [3]. End-stage renal disease (ESRD) has many causes; however, the most common one (30–50%) is type 2 diabetes mellitus [4]. Of other causes, hypertension should receive special attention as well because it can accelerate the progression of chronic renal disease when it coexists with diabetes mellitus [5, 6]. This holds true in diabetic patients as hypertension affects ~ 70% of them [7].
The progression of diabetes complications cannot be stopped; however, one of the most important methods for delaying disease progression is the maintenance of normal blood glucose levels [8]. In addition, controlling blood pressure also leads to reduction in diabetes mellitus complications and diabetes-related deaths [6]. The risk of cardiovascular complications, deaths from cardiovascular events and life expectancy may be improved by enhanced glycaemic control [9]. The Kidney Disease Outcomes Quality Initiative and the Kidney Disease Improving Global Outcomes guidelines recommended that patients with chronic kidney disease or ESRD should maintain their glycated haemoglobin (HbA1c) readings below 7% [10]; however, maintaining optimum blood glucose levels is troublesome for haemodialysis patients with diabetes as they may also suffer from other diseases and comorbidities that can contribute to impaired glycaemic control [11].
Fully understanding the sociodemographic and clinical factors that modulate glycaemic control in haemodialysis patients with diabetes would be of great benefit. These valuable results would guide future studies and interventions and help clinicians and healthcare decision makers to improve patient outcomes and their access to quality care. A total of 382 million people had diabetes in 2013, and this number is expected to increase to 592 million in 2035 [12]. The Middle East had the highest prevalence (10.9%) and the second highest proportional increase after Africa [12]. In Palestine, the prevalence was 9.8% in rural areas and 12% in urban areas [13, 14].
The Palestinian Ministry of Health’s annual 2015 mid-year health analysis reported that 5761 new diabetic cases were discovered in the West Bank, with an incidence rate of 201.3 per 100,000 of population. The total population of Palestinians was 4.6 million with 2.8 million living in the West Bank. The rate of reported diabetes deaths was 6.8% of all deaths. Moreover, 1014 patients were receiving regular haemodialysis [15].
Glycaemic control and its associated factors are not new concepts, and many studies have shown the relationship between glycaemic control and clinical and sociodemographic factors; however, these studies were conducted in different countries [16,17,18,19]. A considerable amount of literature has been published regarding haemodialysis patients in Palestine [20,21,22,23,24,25,26,27,28,29]; however, no single study of that population has investigated the relationship between glycaemic control and diabetes-related knowledge in haemodialysis patients with diabetes. Therefore, the present study was carried out to determine the relationship between glycaemic control and diabetes-related knowledge in haemodialysis patients with diabetes, and to assess the clinical and sociodemographic factors that affect both of these variables.
Methods
Study design
The research approach employed a multicentre, cross-sectional design for diabetic patients on maintenance haemodialysis > 6 months (duration of dialysis), in the West Bank, Palestine.
Study setting
This study was conducted at six dialysis centres in the north of the West Bank, in Nablus, Tulkarem, Jenin, Qalqilya, Tubas and Salfeet. All centres are located in governmental hospitals, except in Nablus, where the location is a teaching hospital [30]. Patients were requested to complete a questionnaire and to provide a blood sample to check HbA1c levels during their routine visits to the centre.
Study population
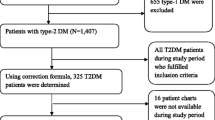
According to the 2015 mid-year annual health analysis from the Palestinian MOH, 507 patients were receiving haemodialysis in the six dialysis centres [15]. A recent study suggested that approximately 45% of haemodialysis patients in these centres were also diabetic; therefore, our available population was approximately 230 individuals [24]. Patients were included in the study if (1) they were older than 18 years; (2) they were confirmed to have ESRD (by a clinician); (3) they had previously been diagnosed with type 2 diabetes mellitus; (4) they had been regularly receiving haemodialysis for at least 6 months; and (5) they had diabetes for ≥ 1 year. Patients with cognitive or mental restrictions to fill out the questionnaire were excluded from the study. From the six dialysis centres, 147 haemodialysis patients were selected.
Data collection instrument
The instrument was composed of three sections. The first section contained sociodemographic data about each participant, including their age, gender, weight and height (to calculate body mass index (BMI)), residency (city, village or refugee camp), living status (with family or alone), education level, marital status, occupation (employed or unemployed), household income and smoking status (smoker or nonsmoker). The second section contained clinical data, including duration of dialysis per year, duration of diabetes per year, number of dialysis sessions per week, total treatment hours per session, kidney transplant (yes or no), total number of chronic medications including anti-diabetic and haemodialysis medication (e.g. insulin, heparin, diuretics and anti-hypertensive drugs); total number of chronic diseases, which included any disease that lasted for a long time or at least 3 months, other than diabetes (e.g. osteoarthritis, hypertension, heart failure and COPD); and drug administration (alone or by other people). Blood samples were also taken by experienced nurses at the dialysis centres, to measure HbA1c levels; the results were subsequently classified as controlled (≤ 7%) or uncontrolled (> 7%) according to a previous study [18]. This classification is also used by health workers to give different management plans according to the patient’s classification.
The third section contained the Arabic-translated version of the Michigan Diabetic Knowledge Test (MDKT). This test was previously assessed for its validity and reliability [31], and that Arabic translation was also used in another study [32]. Permission to use MDKT was obtained from the developer. The first 14 items in the English version’s online questionnaire (http://diabetesresearch.med.umich.edu/peripherals/profs/documents/svi/DKT2_with_answers.pdf) are appropriate to assess knowledge of diabetes. The modified MDKT contained 14 multiple choice questions with only one correct answer for each. Every question in this test evaluated the patient’s knowledge about a particular aspect concerning diabetes. With one point given for a correct answer, none for an incorrect answer, and a total score of 14; thus, more correct answers corresponded to greater knowledge.
Data collection procedure
Permission to interview the patients at the MOH and An-Najah National University Hospital (ANNUH) was obtained before the onset of data collection. The computerised data systems at each dialysis centre were then used to identify the patients who met the study criteria. Those who did were informed of the study and verbal informed consent was obtained. Face-to-face interviews were conducted by medical students to complete the study questionnaire. Qualified nurses working in the dialysis centres then took blood samples, which were refrigerated and sent to the ANNUH laboratory department for measurement of HbA1c levels. The data collection instrument(s) were initially tested on a pilot sample, of just 10 haemodialysis patients with diabetes, to evaluate the response burden as well as comprehension. This pilot sample was not part of the final study sample.
Ethical approval
The Institutional Review Board (IRB) at An-Najah National University approved this study and both the MOH and ANNUH gave permission to perform interviews and withdraw blood samples at their haemodialysis centres. Before any interview or withdrawing blood, every patient’s verbally informed constant insured that their identity would not be revealed and that their information would be protected and coded, so that only the authors would have access to them. The purpose of the study, the authors’ titles/qualifications and the funding agency itself were all explained to the patients, too.
Statistical analysis
Each questionnaire was coded from 1 to 147 and inserted into SPSS version 21 for analysis. Data were expressed as frequency (percentage), mean ± SD or median (interquartile range Q1–Q3) depending on whether it was categorical or continuous. Fisher’s exact test and the chi-square test were used, where appropriate, to test the significance of HbA1c (≤ 7 and > 7), sociodemographic, clinical and MDKT categorical variables. Furthermore, the MDKT was set as the dependent variable, whereas sociodemographic and clinical variables were set as the independent ones. Non-normally distributed variables were represented using the median and interquartile range (IQR). Additionally, the non-normally distributed data were compared, using either the Kruskal–Wallis test or the Mann–Whitney U test, where appropriate, to measure the association between MDKT score and sociodemographic and clinical variables. The significance level (P value) was set to be less than 0.05.
Results
Clinical and sociodemographic characteristics
Of the 147 patients, 76 (51.7%) were male and 71 (48.3%) were female. The average age was 60.12 years (SD = 10.28), with 78 (53.1%) individuals ≤ 60 years and 69 individuals (46.9%) > 60 years of age. Only 38 (25.9%) of the subjects were within the normal BMI range (18.5–24.9), whereas 65 (44.2%) were obese. The cohort contained patients from different regions, but most (57.8%) came from villages. In general, the cohort was poorly educated, with only 28 (19.0%) patients who completed college or had a higher degree. With regards to their socioeconomic status, 118 (80.3%) patients were married and 141 (95.9%) lived with their families; however, 132 (89.8%) were unemployed and 77 (52.4%) had a low household income. Only 32 (21.8%) patients were smokers and only 43 (29.3%) had three or more chronic diseases. Most patients (92.5%) suffered from diabetes for > 5 years, and 56 (38.1%) patients had been receiving haemodialysis for ≥ 4 years (dialysis vintage); further, 128 (87.1%) had three or more sessions per week. Only 3 (2.0 %) patients had undergone kidney transplantation in the past. Ninety (64.6%) patients took their drugs alone and, coincidentally, 95 (64.6%) took less than eight chronic medications. Further information about the clinical and sociodemographic features of the cohort are provided in Table 1.
MDKT values
The average MDKT score in this cohort was 9.19 (SD = 1.7). Patients with low household income and those living in Palestinian refugee camps had significantly lower MDKT scores (P value for both variables was < 0.05). Other sociodemographic and clinical factors were not associated with diabetes knowledge (all P values were > 0.05). These factors were age, gender, BMI, living status, education level, marital status, occupation, smoking, duration of dialysis per year, duration of diabetes per year, frequency of dialysis per session/week, treatment hours per session, kidney transplant status, total chronic diseases, total chronic medications, drug taking and HbA1c levels (all P values were > 0.05). Table 1 shows the associations between MDKT scores and sociodemographic and clinical variables.
HbA1c level as a measure of glycaemic control
Analysis of HbA1c levels in this cohort showed that 94 (63.9%) patients showed good glycaemic control (≤ 7%) while 53 (36.1%) patients showed poor control (> 7%). The mean HbA1c was 6.9 ± 1.7. None of the sociodemographic and clinical factors included in our study were found to be significantly associated with glycaemic control. These factors were similar to those noted above: age, gender, BMI, residency, living status, household income, marital status, occupation, smoking, treatment hours per session, duration of diabetes per year, frequency of dialysis per session/week, duration of dialysis, kidney transplant status, total chronic medications, education level, total chronic diseases, drug taking (alone or by others) and diabetes knowledge. Table 2 shows all the associations between HbA1c and sociodemographic, and clinical factors.
Discussion
This study used the MDKT scores and HbA1c levels to assess the diabetes-related knowledge and to measure glycaemic control, among haemodialysis patients with diabetes, respectively. We also aimed in this study to make correlations between these two variables. This study was the first of its kind in Palestine to use both the MDKT and HbA1c levels in haemodialysis patients with diabetes. Previously, similar studies used only the MDKT in patients with diabetes in Palestine [32], Malaysia [17], Kuwait [16], Turkey [33], South Africa [34] and Nigeria [35].
The median MDKT score was 9 (SD = 1.7), and most patients (70.1%) achieved an acceptable score (e.g. 7–10). These scores are considered higher than those seen in other studies [12, 16, 17, 32, 36], which were performed on diabetic patients who were not dependent on haemodialysis. This could be because diabetes is less problematic in its early stages, which makes it less likely for diabetic patients to perceive their condition as thoughtfully as those with more advanced or complicated illness, such as those with diabetes and on haemodialysis, as in our study [37]. Different variables affected knowledge among haemodialysis patients; for example, refugee camp residents exhibited lower knowledge than those who lived in villages or cities. This could be due to poor health services in refugee camps [38] or because refugees have a lower education level [39]. This study also showed that low income was associated with poor knowledge, which is similar to findings in other studies that were carried on diabetic patients who were not dependent on haemodialysis [16]. Moreover, a study in a low-income population showed that there was a positive association between health literacy and diabetes knowledge [40]. This could explain how poor knowledge may correlate with low income levels in our study.
In our study, gender had no significant association with diabetes knowledge, which is consistent with the results of other studies [16, 35]. These studies showed higher, but not statistically significant, scores in males, as it is the case in our study. However, one investigation showed that South African females had higher knowledge pass rates, when compared with South African males [34]. Moreover, a study in Pakistan showed a significant association between gender and diabetes knowledge, with men scoring significantly higher than women [36]. In our project, there was an increase in diabetes-related knowledge with longer duration of the disease, but it was statistically not significant enough to assume an association, and this was similar to other studies [16, 41]. A plausible explanation could be that the longer patients suffer from diabetes, the more experience they will gain from their disease and the more educational programmes they will attend. Although decreasing age and increasing education levels significantly increased diabetes knowledge in some studies [16, 36], we found no significant associations in our study. Other studies carried out in communities similar to ours attributed this to the cultural environment, which could affect diabetes knowledge by providing wrong information, regardless of the age and level of education [42, 43].
Although many studies suggested using glycated albumin as a more accurate measure than HbA1c to measure blood glucose levels in haemodialysis patients [44,45,46], other studies recommended to depend HbA1c levels as a reliable measurement to assess glycemic control in haemodialysis patients, especially those with values of 6–7% [47, 48]. Moreover, glycated albumin represents blood glucose levels during the previous 7–14 days, which is a much shorter interval than what is provided by HbA1c (60 to 120 days). In addition, there are no long-term studies that investigate the relationship between glycated albumin and the risk of diabetes chronic complications [49,50,51]. Therefore, our project employed HbA1c as a more meaningful measure of glycaemic control. That said, we discovered that there was no significant correlation between glycaemic control and diabetes knowledge, which is in contrast to multiple studies [17, 33, 52] that have documented a significant correlation between these variables. In Nashville, Tennessee (USA), 83 patients were allocated to either a control group or a study group, and participants were followed for 1 year. The authors found that the provision of an educational programme to the study group led to a decline in HbA1c levels, from 6.9 to 6.3%, while the control group showed no change in HbA1c levels [53]. This indicated that prior acquired knowledge had no effect on glycaemic control, whereas an effective and intensive diabetes educational programme at the dialysis unit would be of great benefit. However, this discrepancy could also be due to the difference between what the patients were taught and what they were actually doing (the knowledge-action gap), as reported in a Chinese study which, similar to the Nashville undertaking, did not show an association between HbA1c and diabetes knowledge [54].
Factors that did not affect glycaemic control in this study include education level, diabetes duration and BMI. However, a significant association between these factors and glycaemic control were present in a Jordanian undertaking, carried out on patients with type 2 diabetes mellitus [11]. In our study, there was no association between glycemic control and marital or living status, which was in contrast to a Japanese study, that showed a significant association between glycaemic control and social support [55]. This may indicate that haemodialysis patients with diabetes have additional factors that contribute to this discrepancy, which warrants further investigation. This could also be due to the poor diabetic health programmes in the West Bank.
Strengths and limitations
One strength of our effort here is that it is the first to investigate the association between diabetes knowledge, glycaemic control and clinical parameters in ESRD patients with diabetes who are undergoing haemodialysis. Another advantage of this study is its multicentre design. In addition, it employed the MDKT, which was previously tested and validated [31], and the questionnaire was answered using a face-to-face interview. Of course, it may have had some limitations, such as the fact that the questions were asked by medical students, a process that could have introduced author bias. This study is also a cross-sectional study and, as a result, a cause–effect relationship could not be established. We used the HbA1c to measure the glycaemic level, which would not be 100% reliable in haemodialysis patients. One final limitation is that this project’s focus on patients from dialysis centres in the north of the West Bank in Palestine.
Conclusions
In conclusion, our project and analysis showed that prior diabetes-related knowledge in haemodialysis patients with diabetes significantly depended on their residency and household income, but not on their educational level. The results of this study indicated that a relatively high proportion of diabetic patients on maintenance haemodialysis suffered from poor glycemic control. Moreover, this study also demonstrated that glycaemic control was not significantly related to prior diabetes-related knowledge or any of the sociodemographic and clinical factors used. Therefore, it is recommended that clinicians and healthcare workers provide additional attention to haemodialysis’ patients who live in refugee camps or receive a low income. They should find new ways to approach these patients, to make sure that the best level of health care is delivered and to prevent any diabetes-related complications. In addition, they should follow them up, to diminish patients’ knowledge-action gap. We also recommend that researchers conduct further investigations on differing diabetes education programmes; they would surely benefit from them, through raising knowledge and addressing misconceptions among patients in the early stage of diabetes. The goal would be to prevent diabetes-related complications.
Availability of data and materials
The datasets used for the current study are available from the corresponding author upon request.
Abbreviations
- BMI:
-
Body mass index
- ESRD:
-
End-stage renal disease
- HbA1c:
-
Glycated haemoglobin
- IRB:
-
Institutional Review Board
- MKDT:
-
Michigan Diabetic Knowledge Test
- MOH:
-
Ministry of Health
- ANNUH:
-
An-Najah National University Hospital
- SD:
-
Standard deviation
References
Javanbakht M, Abolhasani F, Mashayekhi A, Baradaran HR, Jahangiri noudeh Y. Health related quality of life in patients with type 2 diabetes mellitus in Iran: a national survey. PLoS One. 2012;7(8):e44526.
Saffari M, Ghanizadeh G, Koenig HG. Health education via mobile text messaging for glycemic control in adults with type 2 diabetes: a systematic review and meta-analysis. Prim Care Diabetes. 2014;8(4):275–85.
Hajos TR, Pouwer F, de Grooth R, Holleman F, Twisk JW, Diamant M, Snoek FJ. The longitudinal association between glycaemic control and health-related quality of life following insulin therapy optimisation in type 2 diabetes patients. A prospective observational study in secondary care. Qual Life Res. 2012;21(8):1359–65.
Mehdi U, Toto RD. Anemia, diabetes, and chronic kidney disease. Diabetes Care. 2009;32(7):1320–6.
Lago RM, Singh PP, Nesto RW. Diabetes and hypertension. Nat Clin Pract Endocrinol Metab. 2007;3(10):667.
Adler AI, Stratton IM, Neil HAW, Yudkin JS, Matthews DR, Cull CA, Wright AD, Turner RC, Holman RR. Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): prospective observational study. BMJ. 2000;321(7258):412.
Klein R, Klein BE, Lee KE, Cruickshanks KJ, Moss SE. The incidence of hypertension in insulin-dependent diabetes. Arch Intern Med. 1996;156(6):622–7.
Calisti L, Tognetti S. Measure of glycosylated hemoglobin. Acta Biomed. 2005;76(Suppl 3):59–62.
American Diabetes Association. Standards of medical care in diabetes. Diabetes Care. 2004;27(Suppl 1):S15–35.
K/DOQI Workgroup: K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis 2005, 45(4 Suppl 3):S1-153.
Khattab M, Khader YS, Al-Khawaldeh A, Ajlouni K. Factors associated with poor glycemic control among patients with type 2 diabetes. J Diabetes Complicat. 2010;24(2):84–9.
Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U, Shaw JE. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res Clin Pract. 2014;103(2):137–49.
Husseini A, Abdul-Rahim H, Awartani F, Jervell J, Bjertness E. Prevalence of diabetes mellitus and impaired glucose tolerance in a rural Palestinian population. East Mediterr Health J. 2000;6(5-6):1039–45.
Abdul-Rahim HF, Husseini A, Giacaman R, Jervell J, Bjertness E. Diabetes mellitus in an urban Palestinian population: prevalence and associated factors. East Mediterr Health J. 2001;7(1-2):67–78.
Ministry of Health, Palestinian Health Information Center. Health status, Palestine, mid year 2015 2016. http://www.moh.ps/Content/Books/kD3bquHr7jbwK9f6VQJAsLDCuckgEDlCZUFa9ssb62m9Eim2le562D_ECDSNEboZRJwc6HyiggSMzKUPMeDJa2vkBNlAdZOGlvNuS9CHKJjGO.pdf. Accessed 23 Sept 2016.
Al-Adsani AM, Moussa MA, Al-Jasem LI, Abdella NA, Al-Hamad NM. The level and determinants of diabetes knowledge in Kuwaiti adults with type 2 diabetes. Diabetes Metab. 2009;35(2):121–8.
Al-Qazaz H, Sulaiman SA, Hassali MA, Shafie AA, Sundram S, Al-Nuri R, Saleem F. Diabetes knowledge, medication adherence and glycemic control among patients with type 2 diabetes. Int J Clin Pharm. 2011;33(6):1028–35.
Rhee JJ, Ding VY, Rehkopf DH, Arce CM, Winkelmayer WC. Correlates of poor glycemic control among patients with diabetes initiating hemodialysis for end-stage renal disease. BMC Nephrol. 2015;16(1):204.
Ghannadi S, Amouzegar A, Amiri P, Karbalaeifar R, Tahmasebinejad Z, Kazempour-Ardebili S. Evaluating the effect of knowledge, attitude, and practice on self-management in type 2 diabetic patients on dialysis. J Diabetes Res. 2016;2016:3730875.
Zyoud SH, Al-Jabi SW, Sweileh WM, Tabeeb GH, Ayaseh NA, Sawafta MN, Khdeir RL, Mezyed DO, Daraghmeh DN, Awang R. Use of complementary and alternative medicines in haemodialysis patients: a cross-sectional study from Palestine. BMC Complement Altern Med. 2016;16:204.
Al Zabadi H, Rahal H, Fuqaha R. Hepatitis B and C prevalence among hemodialysis patients in the West Bank hospitals. Palestine BMC Infect Dis. 2016;16:41.
Al-Ramahi R, Raddad AR, Rashed AO, Bsharat A, Abu-Ghazaleh D, Yasin E, Shehab O. Evaluation of potential drug-drug interactions among Palestinian hemodialysis patients. BMC Nephrol. 2016;17:96.
Naalweh KS, Barakat MA, Sweileh MW, Al-Jabi SW, Sweileh WM, Zyoud SH. Treatment adherence and perception in patients on maintenance hemodialysis: a cross-sectional study from Palestine. BMC Nephrol. 2017;18(1):178.
Zyoud SH, Daraghmeh DN, Mezyed DO, Khdeir RL, Sawafta MN, Ayaseh NA, Tabeeb GH, Sweileh WM, Awang R, Al-Jabi SW. Factors affecting quality of life in patients on haemodialysis: a cross-sectional study from Palestine. BMC Nephrol. 2016;17(1):44.
Dumaidi K, Al-Jawabreh A. Prevalence of occult HBV among hemodialysis patients in two districts in the northern part of the West Bank. Palestine J Med Virol. 2014;86(10):1694–9.
Adas H, Al-Ramahi R, Jaradat N, Badran R. Assessment of adequacy of hemodialysis dose at a Palestinian hospital. Saudi J Kidney Dis Transpl. 2014;25(2):438–42.
Samara AM, Sweileh MW, Omari AM, Omari LS, Dagash HH, Sweileh WM, Natour N, Zyoud SH. An assessment of sleep quality and daytime sleepiness in hemodialysis patients: a cross-sectional study from Palestine. Sleep Sci Pract. 2019;3. https://doi.org/10.1186/s41606-41019-40036-41604.
Omari AM, Omari LS, Dagash HH, Sweileh WM, Natour N, Zyoud SH. Assessment of nutritional status in the maintenance of haemodialysis patients: a cross-sectional study from Palestine. BMC Nephrol. 2019;20(1):92.
Al-Jabi SW, Sous A, Jorf F, Taqatqa M, Allan M, Sawalha L, Lubadeh E, Zyoud SH, Sweileh WM: Depression in patients treated with haemodialysis: a cross-sectional study. Lancet 2018, 391 Suppl 2:S41.
Khatib ST, Hemadneh MK, Hasan SA, Khazneh E, Zyoud SH. Quality of life in hemodialysis diabetic patients: a multicenter cross-sectional study from Palestine. BMC Nephrol. 2018;19(1):49.
Fitzgerald JT, Funnell MM, Hess GE, Barr PA, Anderson RM, Hiss RG, Davis WK. The reliability and validity of a brief diabetes knowledge test. Diabetes Care. 1998;21(5):706–10.
Sweileh WM, Zyoud SH, Abu Nab’a RJ, Deleq MI, Enaia MI, Nassar SM, Al-Jabi SW. Influence of patients’ disease knowledge and beliefs about medicines on medication adherence: findings from a cross-sectional survey among patients with type 2 diabetes mellitus in Palestine. BMC Public Health. 2014;14(1):94.
Ozcelik F, Yiginer O, Arslan E, Serdar MA, Uz O, Kardesoglu E, Kurt I. Association between glycemic control and the level of knowledge and disease awareness in type 2 diabetic patients. Pol Arch Med Wewn. 2010;120(10):399–406.
Moodley LM, Rambiritch V: An assessment of the level of knowledge about diabetes mellitus among diabetic patients in a primary healthcare setting. S Afr Fam Pract 2014, 49(10):16-16d.
Odili VU, Isiboge PD, Eregie A. Patients’ knowledge of diabetes mellitus in a Nigerian city. Trop J Pharm Res. 2011;10(5):637–42.
Rafique G, Azam SI, White F. Diabetes knowledge, beliefs and practices among people with diabetes attending a university hospital in Karachi, Pakistan. East Mediterr Health J. 2006;12(5):590–8.
Brown JB, Harris SB, Webster-Bogaert S, Wetmore S, Faulds C, Stewart M. The role of patient, physician and systemic factors in the management of type 2 diabetes mellitus. Fam Pract. 2002;19(4):344–9.
Giacaman R, Khatib R, Shabaneh L, Ramlawi A, Sabri B, Sabatinelli G, Khawaja M, Laurance T. Health status and health services in the occupied Palestinian territory. Lancet. 2009;373(9666):837–49.
Eljedi A, Mikolajczyk RT, Kraemer A, Laaser U. Health-related quality of life in diabetic patients and controls without diabetes in refugee camps in the Gaza strip: a cross-sectional study. BMC Public Health. 2006;6(1):268.
Speeckaert M, Van Biesen W, Delanghe J, Slingerland R, Wiecek A, Heaf J, Drechsler C, Lacatus R, Vanholder R, Nistor I, et al. Are there better alternatives than haemoglobin A1c to estimate glycaemic control in the chronic kidney disease population? Nephrol Dial Transplant. 2014;29(12):2167–77.
Murata GH, Shah JH, Adam KD, Wendel CS, Bokhari SU, Solvas PA, Hoffman RM, Duckworth WC. Factors affecting diabetes knowledge in Type 2 diabetic veterans. Diabetologia. 2003;46(8):1170–8.
Mull DS, Nguyen N, Mull JD. Vietnamese diabetic patients and their physicians: what ethnography can teach us. West J Med. 2001;175(5):307–11.
Anderson RM, Herman WH, Davis JM, Freedman RP, Funnell MM, Neighbors HW. Barriers to improving diabetes care for blacks. Diabetes Care. 1991;14(7):605–9.
Peacock TP, Shihabi ZK, Bleyer AJ, Dolbare EL, Byers JR, Knovich MA, Calles-Escandon J, Russell GB, Freedman BI. Comparison of glycated albumin and hemoglobin A(1c) levels in diabetic subjects on hemodialysis. Kidney Int. 2008;73(9):1062–8.
Freedman BI, Andries L, Shihabi ZK, Rocco MV, Byers JR, Cardona CY, Pickard MA, Henderson DL, Sadler MV, Courchene LM, et al. Glycated albumin and risk of death and hospitalizations in diabetic dialysis patients. Clin J Am Soc Nephrol. 2011;6(7):1635–43.
Freedman BI, Shihabi ZK, Andries L, Cardona CY, Peacock TP, Byers JR, Russell GB, Stratta RJ, Bleyer AJ. Relationship between assays of glycemia in diabetic subjects with advanced chronic kidney disease. Am J Nephrol. 2010;31(5):375–9.
Joy MS, Cefalu WT, Hogan SL, Nachman PH. Long-term glycemic control measurements in diabetic patients receiving hemodialysis. Am J Kidney Dis. 2002;39(2):297–307.
Konya J, Ng JM, Cox H, Cooke M, Lewis N, Bhandari S, Atkin SL, Kilpatrick ES. Use of complementary markers in assessing glycaemic control in people with diabetic kidney disease undergoing iron or erythropoietin treatment. Diabet Med. 2013;30(10):1250–4.
Abe M, Matsumoto K. Glycated hemoglobin or glycated albumin for assessment of glycemic control in hemodialysis patients with diabetes? Nat Clin Pract Nephrol. 2008;4(9):482–3.
Chen CW, Drechsler C, Suntharalingam P, Karumanchi SA, Wanner C, Berg AH. High glycated albumin and mortality in persons with diabetes mellitus on hemodialysis. Clin Chem. 2017;63(2):477–85.
Sacks DB, Arnold M, Bakris GL, Bruns DE, Horvath AR, Kirkman MS, Lernmark A, Metzger BE, Nathan DM. Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus. Clin Chem. 2011;57(6):e1.
Bains SS, Egede LE. Associations between health literacy, diabetes knowledge, self-care behaviors, and glycemic control in a low income population with type 2 diabetes. Diabetes Technol Ther. 2011;13(3):335–41.
McMurray SD, Johnson G, Davis S, McDougall K. Diabetes education and care management significantly improve patient outcomes in the dialysis unit. Am J Kidney Dis. 2002;40(3):566–75.
Chan Y, Molassiotis A. The relationship between diabetes knowledge and compliance among Chinese with non-insulin dependent diabetes mellitus in Hong Kong. J Adv Nurs. 1999;30(2):431–8.
Nakahara R, Yoshiuchi K, Kumano H, Hara Y, Suematsu H, Kuboki T. Prospective study on influence of psychosocial factors on glycemic control in Japanese patients with type 2 diabetes. Psychosomatics. 2006;47(3):240–6.
Acknowledgments
The authors would like to thank An-Najah National University for providing the opportunity to conduct this study. The project described was supported by Grant Number P30DK020572, awarded by the Michigan Diabetes Research Center (MDRC) from the National Institute of Diabetes and Digestive and Kidney Diseases. As well, we would like to thank the MDRC for permission to use their tool. Also, the authors thank retired British Library curator Andy Simons for English editing of the manuscript.
Funding
Not available.
Author information
Authors and Affiliations
Contributions
MH collected data, performed the analyses, conducted the literature search and drafted the manuscript. SK also collected data, performed the analyses and conducted the literature search. SH, EK and IT participated in the data collection and literature search. SZ conceptualised and designed the study; coordinated, supervised and analysed the data; critically reviewed the manuscript; interpreted the results and assisted in writing the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The IRB at An-Najah National University approved this study. Verbal informed consent was taken from each patient before the interviews were started. Permission from the MOH and ANNUH was also obtained to perform interviews and withdraw blood samples in their institutions. The study protocol was approved (including the verbal consent process) by the IRB and did not require written consent. Patients were asked to provide blood samples and were informed that their information would be coded and anonymised.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Hemadneh, M.K., Khatib, S.T., Hasan, S.A. et al. Diabetes-related knowledge in diabetic haemodialysis patients: a cross-sectional study from Palestine. Ren Replace Ther 5, 45 (2019). https://doi.org/10.1186/s41100-019-0241-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41100-019-0241-8