
Abstract
Accumulation of uremic toxins induces various uremia-related complications in patients with chronic kidney disease, particularly those undergoing dialysis treatment. Direct interactions of uremic toxins with organ tissues are thought to be a major pathophysiological mechanism for disease; for example, indoxyl sulfate reacts directly with macrophages and accelerates atherosclerosis. The removal of sufficient volume of uremic toxins will prevent uremia-related complications in dialysis patients. Hemodialysis with the use of a high-flux dialysis membrane, long or frequent treatment, and increased blood/dialysate flow has improved removal of water-soluble small molecular weight uremic toxins. Middle molecular weight molecules are removed more effectively with hemodialysis using a high-flux membrane, hemodiafiltration and hemofiltration, and a direct hemoperfusion method using β2-microglobulin adsorption column, which is useful in reducing serum β2-microglobulin levels as well as improving dialysis-related amyloidosis-induced clinical symptoms. With improvements in dialysis therapies, removal of low and middle molecular weight water-soluble molecules has improved; however, conventional dialysis treatment is limited in its ability to remove protein-bound uremic toxins (PBUTs). Recent findings suggest that adsorption treatments using oral charcoal adsorbent, mixed matrix membrane hollow fiber, and additive charcoal in the dialysate, in addition to conventional dialysis treatment, may effectively remove a substantial amount of PBUTs. Further improvement of renal replacement therapy, including dialysis and additional therapeutic strategies, is needed for better clearance of small and middle molecular weight molecules and PBUTs, which will lead to improved survival and quality of life for dialysis-dependent chronic kidney disease patients.
Similar content being viewed by others

Background
Patients with chronic kidney disease (CKD), particularly those undergoing dialysis treatment, develop various systemic complications, such as cardiovascular disease, mineral and bone disorders, and infectious disease. One of the reasons underlying the development of these complications is direct or indirect interactions between various uremic toxins and organ tissues [1–3]. Thus, renal replacement therapies must effectively remove a sufficient amount of uremic toxins in order to improve survival and prevent CKD-related complications. With progress in dialysis therapies, removal of low and middle molecular weight water-soluble molecules has improved; however, conventional dialysis treatment is limited in its ability to remove protein-bound uremic toxins (PBUTs) owing to their binding to large molecular proteins [4]. In this article, we review characteristics of uremic toxins, particularly PBUTs, as well as recent progress and future perspective on therapeutic strategies for removal of uremic toxins.
Uremic toxins
Progressive kidney disease induces uremic syndrome, with the retention of various solutes that are normally excreted by the kidney. Solutes with biological toxicity, direct or indirect, are called “uremic toxins” (Table 1) [5]. A literature search identified 88 uremic toxins from 621 articles, and these were classified into three groups according to molecular weight and binding properties, such as water-soluble low molecular weight, middle molecular weight, and protein-bound solutes [6].
There are 40 kinds of free water-soluble low molecular weight molecules (<0.5 kDa) that are considered uremic toxins. For example, recent findings showed that serum level of trimethylamine-N-oxide (TMAO), molecular weight 75, is increased in hemodialysis patients [7], and clinical research demonstrated an association between serum level of TMAO and cardiovascular disease [8]. Dietary intake of phosphatidylcholine serves as fuel for intestinal microbiota, resulting in the production of trimethylamine, which is oxidized to TMAO in the liver. TMAO accelerates atherosclerosis; a direct reaction with macrophages was demonstrated in a mouse model [9]. Thus, elevated TMAO level in dialysis patients accelerates atherosclerosis by inducing functional abnormalities of macrophages. Uremic toxins with a small molecular weight are easily removed with conventional dialysis treatment. Kt/V urea is widely used to assess the efficiency of small uremic toxin removal in dialysis patients. Previous clinical studies showed that single-pool Kt/V urea up to 1.8 correlated with improved survival in Japanese hemodialysis patients [10] while high dose hemodialysis with Kt/V urea 1.71 did not show significant benefit for mortality as compared to standard dose of dialysis with Kt/V urea 1.32 [11]. According to those clinical studies, Japanese Society of Dialysis Therapy (JSDT) recommends to keep Kt/V urea more than 1.2 for hemodialysis patients for the better survival [12]. However, evaluation of Kt/V urea alone is not adequate to determine dialysis adequacy, because (1) there are limited reports concerning toxicity of urea, (2) distribution volume of urea is different from that of other water-soluble small molecules, and (3) Kt/V urea dose did not evaluate the adequacy of removal of middle molecular weight and protein-bound molecules [13]. Thus, clinicians should consider Kt/V as a minimum requirement parameter, and consider total dialysis adequacy to include not only Kt/V but also other middle molecular weight- and PBUT-related markers.
There are 25 types of middle molecular weight molecules, those molecular weight from 0.5 to 60 kDa, such as β2-microglobulin (β2-m) and α1-macroglobulin. Clearance of middle molecular weight molecules by a hemodialyzer is not as great as that of small molecules owing to their larger molecular weight; however, the use of high-flux dialyzer or hemodiafiltration results in better clearance of middle molecular weight molecules than hemodialysis with low-flux dialyzer. β2-m, a representative middle molecular weight molecule (11.8 kDa), correlates with survival in dialysis patients. In the randomized hemodialysis (HEMO) study, the relationship between serum β2-m levels or dialyzer β2-m clearance and mortality over a period of 2.84 years was analyzed [14]. In time-dependent Cox regression models, pre-dialysis serum β2-m levels were associated with all-cause mortality in maintenance hemodialysis patients [14]. In Japan, Okuno et al. reported that all-cause and non-cardiovascular mortality in hemodialysis patients with a serum β2-m level greater than 32.2 mg/L were higher than that in those with a level lower than 32.2 mg/L [15]. Although HEMO study did not demonstrate an association between serum β2-m level and cardiovascular mortality [14], several studies reported the possibilities of a relationship between β2-m and cardiovascular disease. A report showed that serum level of β2-m in CKD patients, including those undergoing chronic dialysis, was associated with vascular calcification as well as cardiovascular events/mortality during a mean follow-up of 969 days [16]. A cross-sectional study revealed that serum β2-m level correlated with heart valve calcification, which is associated with carotid intima media thickness in dialysis patients [17]. Another clinical study showed that serum β2-m levels positively correlated with several cardiovascular risk factors, such as highly sensitive C-reactive protein, troponin-T, myeloperoxidase, and N-terminal pro-B-type natriuretic peptide, and inversely correlated with prealbumin and ankle-brachial index [18]. In addition to all-cause and cardiovascular mortality, mortality due to infections was also increased in dialysis patients with high serum β2-m levels [19]. These reports indicate that a high serum level of β2-m is associated with mortality, partially due to cardiovascular disease and infection in patients undergoing maintenance hemodialysis treatment. There is no data to show that increase of β2-m removal by renal replacement therapy induces better survival in dialysis patients, and further studies are needed to understand it. With present evidences, JSDT recommends the maintenance of serum β2-m at a pre-dialysis level of less than 30 mg/L [12]. In peritoneal dialysis patients, serum β2-m level is conversely related with residual kidney function [20], and patients should switch their renal replacement therapy from peritoneal dialysis to hemodialysis when the serum level of β2-m increases above 30 mg/L [21]. From another point of view, β2-m is a precursor protein for dialysis-related amyloidosis (DRA). β2-m-related amyloid fibrils are formed and deposited primarily in osteoarticular joint tissues, resulting in various osteoarticular disorders, such as carpal tunnel syndrome, destructive spondyloarthropathy, and bone cysts in dialysis patients [22]. Duration of dialysis treatment is one of the risk factors for osteoarticular disorders, and the accumulation of β2-m during long-term dialysis treatment may be related to this development [23]. Conformational change of the β2-m molecule is needed for amyloid fibril formation in the in vitro setting [24], and intermediate states of β2-m molecules are found in hemodialysis patients [25]. Thus, the accumulation and conformational change of β2-m molecules are required for the development of DRA during prolonged dialysis treatment.
PBUTs are strongly protein-bound and are difficult to remove with conventional hemodialysis treatment. For example, indoxyl sulfate (IS) and p-cresyl sulfate (PCS) are 97.7 and 95.1 % protein-bound, respectively, and reduction rates of IS and PCS by standard hemodialysis are only 31.8 and 29.1 %, respectively [26] (Table 2).
Recently, the relationships between several PBUTs and mortality in CKD patients were reported. Serum level of IS increased with the progression of CKD, particularly in patients undergoing dialysis treatment. IS was associated with increased cardiovascular mortality in CKD patients as well as aortic calcification and pulse wave velocity [2]. Indoleacetic acid (IAA) showed trends similar to IS, and multivariate analysis showed that IAA, but not IS and PCS, remained a significant predictor of mortality and cardiovascular events [27]. Direct interactions of uremic toxins with blood vessel cells are thought to be a major pathophysiological mechanism for the development of cardiovascular disease in CKD patients [1]. When various types of PBUTs at the concentration found in dialysis patients, with or without albumin, were exposed to human umbilical vein endothelial cells (HUVEC), production of reactive oxygen species (ROS) from cells increased most intensely with IS, followed by indole glucuronide, hippuric acid, and PCS, in the absence of albumin. Even in the presence of albumin, IS and 3-carboxy-4-methyl-5-propyl-2-furanpropionic increased ROS production form HUVEC in vitro [26]. When macrophages differentiated from THP-1 cells were exposed to IS in vitro, IS decreased cell viability but promoted macrophage inflammatory cytokine production as well as ROS production. IS also reduced macrophage cholesterol efflux and decreased ATP-binding cassette transporters G1 expression [28]. These results indicate that direct interactions of IS with macrophages may be a major cause of atherosclerosis acceleration in patients with CKD (Fig. 1). In an animal study, atherosclerotic lesions in apolipoprotein E deficient mice were significantly accelerated by uninephrectomy or subtotal nephrectomy as compared to those with normal kidney function [29–31]. When the mice were treated with an oral charcoal adsorbent AST-120 after renal ablation, AST-120 treatment dramatically ameliorated the kidney damage-induced atherosclerosis [29]. These mice had less aortic deposition of IS, as well as reduced aortic expression of inflammatory cytokines. These results suggest that PBUTs, particularly IS, accelerate atherosclerosis as a result of direct interaction with macrophages and endothelial cells in the aorta. AST-120 also modulated CKD-induced cardiac damage, with decreased serum/urine levels of IS and oxidative stress markers, such as 8-hydroxy-2’-deoxyguanosine and aclorein, in a rat model [32]. Concerning bone disease, thyroparathyroidectomy and progressive partial nephrectomy in rats induced an increase of the mineral/matrix ratio and carbonate substitution as well as decreased storage modulus and crystallinity as compared to thyroparathyroidectomy alone. AST-120 abolished kidney damage-induced bone abnormalities and decreased serum IS concentration [33]. These findings suggest that uremic toxins react with various organs, directly or indirectly, and removal of these toxins with AST-120 will result in improved organ function. Clinical studies have not shown clearly that AST-120 had beneficial effect on CKD-related complications as compared to rodent studies, probably owing to the dose of AST-120. Many basic and clinical research studies suggest the importance of PBUTs in various CKD-related complications; however, there is still no recommendation concerning adequate concentration or removal of PBUTs for improved survival, and commercial measurements of these toxins are not clinically available.

Indoxyl sulfate (IS) induces macrophage foam cell formation in an atherosclerotic lesion. IS, a protein-bound uremic toxin, reacts directly with macrophages and induces production of inflammatory cytokines as well as impairment of cholesterol efflux to high-density lipoprotein, leading to macrophage foam cell formation
Removal of uremic toxins by renal replacement therapies
Current progress in renal replacement therapies has improved the removal of various uremic toxins in dialysis patients, but current methods are insufficient to prevent CKD-related systemic complications.
-
1)
Hemodialysis
Removal of uremic toxins, particularly middle molecular weight molecules, has been improved with hemodialysis using the high-flux dialyzer membrane [34]. A large randomized, controlled trial showed that high dose hemodialysis increased Kt/V urea, but not clearance of β2-m, and use of a high-flux dialyzer increased clearance of β2-m, but not Kt/V urea [11]. The removal of small and middle molecular weight molecules by hemodialysis is dependent on treatment time, even with slow flow of both blood and dialysate [35]. Compared with hemodialysis for 4 h with 350 ml/min blood and dialysate flow rate, 8-h dialysis sessions with 190 ml/min blood and dialysate flow rate increased the removal of urea and β2-m by 22.6 and 39.2 %, respectively. Reduction rate of IS and PCS are 31.8 and 29.1 %, respectively, with regular hemodialysis treatment [26], and there was a trend towards the increased removal of these molecules with 8-h hemodialysis as compared to routine 4-h treatment [35]. Another clinical study showed that daily hemodialysis maintained lower serum levels of IS and IAA as well as lower levels of non-protein-bound solutes [36]. Recent finding showed that the time extension for hemodialysis resulted in improved removal of not only small and middle molecular weight molecules but also some PBUTs as to standard hemodialysis when patients used the same high-flux dialyzer, dialysis flow, and blood flow [37]. Dialyzers also affect the efficiency of PBUT extraction. Large pore super-flux cellulose triacetate membranes (SF) showed much removal of IS, IAA, and hippuric acid than low-flux cellulose triacetate membranes (LF) (removal rate of IS; SF 32.5 ± 8.5 % vs LF 24.8 ± 6.5 %) [38]. These studies suggest that prescriptions for hemodialysis, such as the type of dialysis membrane, treatment time, and blood/dialysate flow rates, affect the clearance of not only small and middle molecular weight molecules but also some PBUTs; however, these changes remain insufficient to prevent CKD-related complications.
-
2)
Hemodiafiltration and hemofiltration
Hemodiafiltration (HDF) and hemofiltration (HF) are more effective to remove water-soluble middle molecules than hemodialysis due to the increase of convection, but the effect is small for PBUTs. A crossover trial clinical to examine the removal of uremic toxins by hemodialysis or post-dilution HDF was conducted [39]. Post-dilution HDF increased the instantaneous plasma clearance of urea and β2-m as compared to hemodialysis; however, clearance of both total and free IS and PCS did not increase with the change from hemodialysis to HDF [39]. In the comparison of different convective strategies, removal of small molecules, such as urea and creatinine, was more effective with post-dilution HDF than pre-dilution HDF and HF [40]. In the case of middle molecular weight molecules, post-dilution HDF is superior to pre-dilution HDF for the removal of β2-m. For some PBUTs, including hippuric acid, IS, and PCS, both pre- and post-dilution HDF are superior to post-dilution HF [40]. It is difficult to compare the properties to remove uremic toxins between HDF and HD using SF; however, these findings suggest that physicians should choose the types of convection based upon the type of uremic toxins to be removed most efficaciously for each dialysis patient.
-
3)
β2-microglobulin adsorption column
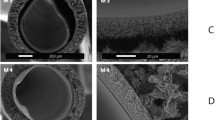
The Lixelle® column was developed for direct β2-m adsorption from circulating blood and is used primarily for hemodialysis patients with progressive DRA. Lixelle contains a porous cellulose bead filling with a sodium citrate buffer. The porous cellulose beads were designed to selectively adsorb β2-m, having the appropriate pore size and hydrophobic interaction. This adsorption column system is designed for direct hemoperfusion and is used in combination with a dialyzer that is the downstream of the Lixelle column (Fig. 2). There are several clinical trials demonstrating the effect of Lixelle on the reduction of β2-m in patients undergoing hemodialysis [41–46]. The Lixelle column induces a 60.0–78.9 % reduction in serum β2-m with 157–300 mg removal; the serum level of β2-m decreased from 27.1–29.0 to 6.8–13.5 mg/L [41, 42, 46]. According to a prospective multicenter study, a Lixelle column (S-35) placed in series with a polysulfone dialyzer increased serum β2-m reduction in patients undergoing hemodialysis as compared to hemodialysis treatment without Lixelle (reduction rate: 74.1 ± 6.1 vs 60.1 ± 6.3 %) [46]. These clinical studies also showed improvements in DRA-related symptoms, such as joint pain and activities of daily living [41, 43–48]. Gejyo et al. surveyed the clinical effect of Lixelle in hemodialysis patients with DRA. Of 345 patients with DRA, 56.2 % patients treated with Lixelle for 3.5 ± 2.7 years reported improvement in their DRA-related symptoms [47]. Some clinical study showed shrinkage in the size of bone cysts owing to amyloidosis when evaluated by X-ray [41, 49]; thus, this direct hemoperfusion treatment may decrease the deposition of β2-m-related amyloid. In addition, the Lixelle column adsorbs not only β2-m but also other molecules, including inflammatory cytokines, with molecular sizes ranging from 4000 to 20,000 Da [50]. This may be another explanation for the improvement in DRA-related clinical symptoms.
Fig. 2 
Schematic representation of blood flow through the dialyzer and β2-microglobulin (β2-m) adsorption column. The column system is designed for direct hemoperfusion and is used in combination with a hemodialyzer downstream of the β2-m adsorption column
-
4)
Other treatments
The removal of water-soluble small and middle molecular weight uremic toxins has been improved with hemodialysis, HDF/HF, or direct hemoperfusion; however, the efficacy of these dialysis treatments in the removal of PBUTs is small. Even in the case of CKD patients undergoing peritoneal dialysis, residual kidney function is more important to decrease PBUTs than peritoneal clearance [51, 52]. Thus, alternative or additional therapeutic strategies will be needed for future blood purification therapies to prevent PBUT-induced dialysis-related complications, including cardiovascular disease.

The oral charcoal adsorbent AST-120 is known to reduce serum levels of IS through the adsorption of indole, which is converted from dietary tryptophan in the gastrointestinal tract in non-dialysis CKD patients [53]. Although randomized, controlled trials did not clearly demonstrate inhibited progression of renal disease in non-dialysis CKD patients with the use of AST-120 [54, 55], a clinical study showed that the treatment in pre-dialysis may affect the prognosis after initiation of dialysis treatment [56]. Thus, AST-120, the adsorption treatment, may show more benefit for prognosis in dialysis patients because this population has much higher levels of circulating PBUTs [2, 26]. When anuric patients undergoing maintenance hemodialysis treatment used AST-120 6 g/day for 2 weeks, total and free IS levels in the predialysis session decreased significantly with AST-120 treatment from 3.06 to 1.63 mg/dL and from 0.098 to 0.023 mg/dL, respectively [57]. The use of AST-120 also reduced the PCS (total and free) and phenyl sulfate (free). We also evaluated changes in the oxidative stress markers with AST-120 treatment in dialysis patients and found that the use of AST-120 induced significant reduction in oxidized albumin content as well as 8-isoprostane [57]. Another study investigated the effect of a mixed matrix membrane (MMM) for the removal of protein-bound uremic toxins [58]. The MMM hollow fiber consists of a porous macrovoid free polymeric inner membrane layer strongly attached to the activated carbon-containing outer MMM layer; it absorbed 2.27 mg PCS/g membrane and 3.58 mg PCS/g membrane in diffusion as well as convection for 4 h from human plasma [58]. The addition of charcoal to the dialysate increased the clearance of indican (12 vs 5 ml/min without sorbent), PCS (9 vs 4 ml/min without sorbent), and p-cresol (35 vs 14 ml/min without sorbent) in artificial plasma [59]. Taken together, these adsorption treatments have the potential to remove significantly more PBUTs when added to conventional dialysis treatment, and removal with adsorption may be a key strategy in next generation renal replacement therapy.
Conclusions
Recent progress in dialysis treatment has increased the removal of uremic toxins, but these improvements are insufficient to prevent CKD-related complications and improve mortality, particularly concerning levels of PBUTs. Further improvements in renal replacement therapy including hemodialysis or additional therapeutic strategies will be needed for better clearance of small and middle molecular weight molecules as well as PBUTs.
Abbreviations
CKD, chronic kidney disease; DRA, dialysis-related amyloidosis; HDF, hemodiafiltration; HF, hemofiltration; HUVEC, human umbilical vein endothelial cells; IAA, indoleacetic acid; IS, indoxyl sulfate; JSDT, Japanese Society of Dialysis Therapy; MMM, mixed matrix membrane; PBUTs, protein-bound uremic toxins; PCS, p-cresyl sulfate; ROS, reactive oxygen species; TMAO, trimethylamine-N-oxide; β2-m, β2-microglobulin.
References
Lekawanvijit S, Kompa AR, Wang BH, Kelly DJ, Krum H. Cardiorenal syndrome: the emerging role of protein-bound uremic toxins. Circ Res. 2012;111:1470–83.
Barreto FC, Barreto DV, Liabeuf S, Meert N, Glorieux G, Temmar M, Choukroun G, Vanholder R, Massy ZA. Serum indoxyl sulfate is associated with vascular disease and mortality in chronic kidney disease patients. Clin J Am Soc Nephrol. 2009;4:1551–8.
Bammens B, Evenepoel P, Keuleers H, Verbeke K, Vanrenterghem Y. Free serum concentrations of the protein-bound retention solute p-cresol predict mortality in hemodialysis patients. Kidney Int. 2006;69:1081–7.
Susantitaphong P, Siribamrungwong M, Jaber BL. Convective therapies versus low-flux hemodialysis for chronic kidney failure: a meta-analysis of randomized controlled trials. Nephrol Dial Transplant. 2013;28:2859–74.
Niwa T. Uremic toxicity of indoxyl sulfate. Nagoya J Med Sci. 2010;72:1–11.
Duranton F, Cohen G, De Smet R, Rodriguez M, Jankowski J, Vanholder R, Argiles A, European Uremic Toxin Work, G. Normal and pathologic concentrations of uremic toxins. J Am Soc Nephrol. 2012;23:1258–70.
Bain MA, Faull R, Fornasini G, Milne RW, Evans AM. Accumulation of trimethylamine and trimethylamine-N-oxide in end-stage renal disease patients undergoing haemodialysis. Nephrol Dial Transplant. 2006;21:1300–4.
Tang WH, Wang Z, Levison BS, Koeth RA, Britt EB, Fu X, Wu Y, Hazen SL. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. N Engl J Med. 2013;368:1575–84.
Wang Z, Klipfell E, Bennett BJ, Koeth R, Levison BS, Dugar B, Feldstein AE, Britt EB, Fu X, Chung YM, Wu Y, Schauer P, Smith JD, Allayee H, Tang WH, DiDonato JA, Lusis AJ, Hazen SL. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature. 2011;472:57–63.
Shinzato T, Nakai S, Akiba T, Yamazaki C, Sasaki R, Kitaoka T, Kubo K, Shinoda T, Kurokawa K, Marumo F, Sato T, Maeda K. Survival in long-term haemodialysis patients: results from the annual survey of the Japanese Society for Dialysis Therapy. Nephrol Dial Transplant. 1997;12:884–8.
Eknoyan G, Beck GJ, Cheung AK, Daugirdas JT, Greene T, Kusek JW, Allon M, Bailey J, Delmez JA, Depner TA, Dwyer JT, Levey AS, Levin NW, Milford E, Ornt DB, Rocco MV, Schulman G, Schwab SJ, Teehan BP, Toto R. Effect of dialysis dose and membrane flux in maintenance hemodialysis. N Engl J Med. 2002;347:2010–9.
Watanabe Y, Kawanishi H, Suzuki K, Nakai S, Tsuchida K, Tabei K, Akiba T, Masakane I, Takemoto Y, Tomo T, Itami N, Komatsu Y, Hattori M, Mineshima M, Yamashita A, Saito A, Naito H, Hirakata H, Minakuchi J. “Maintenance hemodialysis: hemodialysis prescriptions” guideline working group, JSfDT: Japanese society for dialysis therapy clinical guideline for “maintenance hemodialysis: hemodialysis prescriptions”. Ther Apher Dial. 2015;19 Suppl 1:67–92.
Vanholder R, Glorieux G, Eloot S. Once upon a time in dialysis: the last days of Kt/V? Kidney Int. 2015;88:460–5.
Cheung AK, Rocco MV, Yan G, Leypoldt JK, Levin NW, Greene T, Agodoa L, Bailey J, Beck GJ, Clark W, Levey AS, Ornt DB, Schulman G, Schwab S, Teehan B, Eknoyan G. Serum beta-2 microglobulin levels predict mortality in dialysis patients: results of the HEMO study. J Am Soc Nephrol. 2006;17:546–55.
Okuno S, Ishimura E, Kohno K, Fujino-Katoh Y, Maeno Y, Yamakawa T, Inaba M, Nishizawa Y. Serum beta2-microglobulin level is a significant predictor of mortality in maintenance haemodialysis patients. Nephrol Dial Transplant. 2009;24:571–7.
Liabeuf S, Lenglet A, Desjardins L, Neirynck N, Glorieux G, Lemke HD, Vanholder R, Diouf M, Choukroun G, Massy ZA, European Uremic Toxin Work, G. Plasma beta-2 microglobulin is associated with cardiovascular disease in uremic patients. Kidney Int. 2012;82:1297–303.
Ikee R, Honda K, Oka M, Maesato K, Mano T, Moriya H, Ohtake T, Kobayashi S. Association of heart valve calcification with malnutrition-inflammation complex syndrome, beta-microglobulin, and carotid intima media thickness in patients on hemodialysis. Ther Apher Dial. 2008;12:464–8.
Kuragano, T, Kida, A, Furuta, M, Nanami, M, Otaki, Y, Hasuike, Y, Nonoguchi, H, Nakanishi, T: The impact of beta2-microglobulin clearance on the risk factors of cardiovascular disease in hemodialysis patients. ASAIO J. 2010;56:326–332.
Cheung AK, Greene T, Leypoldt JK, Yan G, Allon M, Delmez J, Levey AS, Levin NW, Rocco MV, Schulman G, Eknoyan G, Group, HS. Association between serum 2-microglobulin level and infectious mortality in hemodialysis patients. Clin J Am Soc Nephrol. 2008;3:69–77.
Yamamoto S, Kasai A, Shimada H. High peritoneal clearance of small molecules did not provide low serum beta2-microglobulin concentrations in peritoneal dialysis patients. Perit Dial Int. 2003;23 Suppl 2:S34–6.
Working Group Committee for Preparation of Guidelines for Peritoneal Dialysis, JSfDT, Japanese Society for Dialysis, T. 2009 Japanese Society for Dialysis Therapy guidelines for peritoneal dialysis. Ther Apher Dial. 2010;14:489–504.
Yamamoto S, Kazama JJ, Narita I, Naiki H, Gejyo F. Recent progress in understanding dialysis-related amyloidosis. Bone. 2009;45 Suppl 1:S39–42.
Dember LM, Jaber BL. Dialysis-related amyloidosis: late finding or hidden epidemic? Semin Dial. 2006;19:105–9.
Naiki, H, Okoshi, T, Ozawa, D, Yamaguchi, I, Hasegawa, K: Molecular pathogenesis of human amyloidosis: lessons from beta-microglobulin-related amyloidosis. Pathol Int. 2016;66:193–201.
Uji Y, Motomiya Y, Ando Y. A circulating beta 2-microglobulin intermediate in hemodialysis patients. Nephron Clin Pract. 2009;111:c173–81.
Itoh Y, Ezawa A, Kikuchi K, Tsuruta Y, Niwa T. Protein-bound uremic toxins in hemodialysis patients measured by liquid chromatography/tandem mass spectrometry and their effects on endothelial ROS production. Anal Bioanal Chem. 2012;403:1841–50.
Dou L, Sallee M, Cerini C, Poitevin S, Gondouin B, Jourde-Chiche N, Fallague K, Brunet P, Calaf R, Dussol B, Mallet B, Dignat-George F, Burtey S. The cardiovascular effect of the uremic solute indole-3 acetic acid. J Am Soc Nephrol. 2015;26:876–87.
Matsuo K, Yamamoto S, Wakamatsu T, Takahashi Y, Kawamura K, Kaneko Y, Goto S, Kazama JJ, Narita I. Increased proinflammatory cytokine production and decreased cholesterol efflux due to downregulation of ABCG1 in macrophages exposed to indoxyl sulfate. Toxins (Basel). 2015;7:3155–66.
Yamamoto S, Zuo Y, Ma J, Yancey PG, Hunley TE, Motojima M, Fogo AB, Linton MF, Fazio S, Ichikawa I, Kon V. Oral activated charcoal adsorbent (AST-120) ameliorates extent and instability of atherosclerosis accelerated by kidney disease in apolipoprotein E-deficient mice. Nephrol Dial Transplant. 2011;26:2491–7.
Suganuma E, Zuo Y, Ayabe N, Ma J, Babaev VR, Linton MF, Fazio S, Ichikawa I, Fogo AB, Kon V. Antiatherogenic effects of angiotensin receptor antagonism in mild renal dysfunction. J Am Soc Nephrol. 2006;17:433–41.
Bro S, Bentzon JF, Falk E, Andersen CB, Olgaard K, Nielsen LB. Chronic renal failure accelerates atherogenesis in apolipoprotein E-deficient mice. J Am Soc Nephrol. 2003;14:2466–74.
Fujii H, Nishijima F, Goto S, Sugano M, Yamato H, Kitazawa R, Kitazawa S, Fukagawa M. Oral charcoal adsorbent (AST-120) prevents progression of cardiac damage in chronic kidney disease through suppression of oxidative stress. Nephrol Dial Transplant. 2009;24:2089–95.
Iwasaki Y, Kazama JJ, Yamato H, Shimoda H, Fukagawa M. Accumulated uremic toxins attenuate bone mechanical properties in rats with chronic kidney disease. Bone. 2013;57:477–83.
Palmer SC, Rabindranath KS, Craig JC, Roderick PJ, Locatelli F, Strippoli GF. High-flux versus low-flux membranes for end-stage kidney disease. Cochrane Database Syst Rev. 2012;9:CD005016.
Basile C, Libutti P, Di Turo AL, Casino FG, Vernaglione L, Tundo S, Maselli P, De Nicolo EV, Ceci E, Teutonico A, Lomonte C. Removal of uraemic retention solutes in standard bicarbonate haemodialysis and long-hour slow-flow bicarbonate haemodialysis. Nephrol Dial Transplant. 2011;26:1296–303.
Fagugli RM, De Smet R, Buoncristiani U, Lameire N, Vanholder R. Behavior of non-protein-bound and protein-bound uremic solutes during daily hemodialysis. Am J Kidney Dis. 2002;40:339–47.
Cornelis T, Eloot S, Vanholder R, Glorieux G, van der Sande FM, Scheijen JL, Leunissen KM, Kooman JP, Schalkwijk CG. Protein-bound uraemic toxins, dicarbonyl stress and advanced glycation end products in conventional and extended haemodialysis and haemodiafiltration. Nephrol Dial Transplant. 2015;30:1395–402.
De Smet R, Dhondt A, Eloot S, Galli F, Waterloos MA, Vanholder R. Effect of the super-flux cellulose triacetate dialyser membrane on the removal of non-protein-bound and protein-bound uraemic solutes. Nephrol Dial Transplant. 2007;22:2006–12.
Krieter DH, Hackl A, Rodriguez A, Chenine L, Moragues HL, Lemke HD, Wanner C, Canaud B. Protein-bound uraemic toxin removal in haemodialysis and post-dilution haemodiafiltration. Nephrol Dial Transplant. 2010;25:212–8.
Meert N, Eloot S, Waterloos MA, Van Landschoot M, Dhondt A, Glorieux G, Ledebo I, Vanholder R. Effective removal of protein-bound uraemic solutes by different convective strategies: a prospective trial. Nephrol Dial Transplant. 2009;24:562–70.
Homma N, Gejyo F, Hasegawa S, Teramura T, Ei I, Maruyama H, Arakawa M. Effects of a new adsorbent column for removing beta-2-microglobulin from circulating blood of dialysis patients. Contrib Nephrol. 1995;112:164–71.
Gejyo F, Homma N, Hasegawa S, Arakawa M. A new therapeutic approach to dialysis amyloidosis: intensive removal of beta 2-microglobulin with adsorbent column. Artif Organs. 1993;17:240–3.
Nakazawa R, Azuma N, Suzuki M, Nakatani M, Nankou T, Furuyoshi S, Yasuda A, Takata S, Tani N, Kobayashi F. A new treatment for dialysis-related amyloidosis with beta 2-microglobulin adsorbent column. Int J Artif Organs. 1993;16:823–9.
Gejyo F, Teramura T, Ei I, Arakawa M, Nakazawa R, Azuma N, Suzuki M, Furuyoshi S, Nankou T, Takata S, et al. Long-term clinical evaluation of an adsorbent column (BM-01) of direct hemoperfusion type for beta 2-microglobulin on the treatment of dialysis-related amyloidosis. Artif Organs. 1995;19:1222–6.
Abe T, Uchita K, Orita H, Kamimura M, Oda M, Hasegawa H, Kobata H, Fukunishi M, Shimazaki M, Akizawa T, Ahmad S. Effect of beta(2)-microglobulin adsorption column on dialysis-related amyloidosis. Kidney Int. 2003;64:1522–8.
Gejyo F, Kawaguchi Y, Hara S, Nakazawa R, Azuma N, Ogawa H, Koda Y, Suzuki M, Kaneda H, Kishimoto H, Oda M, Ei K, Miyazaki R, Maruyama H, Arakawa M, Hara M. Arresting dialysis-related amyloidosis: a prospective multicenter controlled trial of direct hemoperfusion with a beta2-microglobulin adsorption column. Artif Organs. 2004;28:371–80.
Gejyo F, Amano I, Ando T, Ishida M, Obayashi S, Ogawa H, Ono T, Kanno Y, Kitaoka T, Kukita K, Kurihara S, Sato M, Shin J, Suzuki M, Takahashi S, Taguma Y, Takemoto Y, Nakazawa R, Nakanishi T, Nakamura H, Hara S, Hiramatsu M, Furuya R, Masakane I, Tsuchida K, Motomiya Y, Morita H, Yamagata K, Yoshiya K, Yamakawa T. Survey of the effects of a column for adsorption of beta2-microglobulin in patients with dialysis-related amyloidosis in Japan. Ther Apher Dial. 2013;17:40–7.
Yamamoto Y, Hirawa N, Yamaguchi S, Ogawa N, Takeda H, Shibuya K, Kawahara K, Kojima H, Dobashi Y, Fujita M, Azusima K, Miyazaki N, Kobayashi M, Kobayashi C, Fujiwara A, Yuto J, Saka S, Yatsu K, Toya Y, Yasuda G, Ohnishi T, Umemura S. Long-term efficacy and safety of the small-sized beta2-microglobulin adsorption column for dialysis-related amyloidosis. Ther Apher Dial. 2011;15:466–74.
Kuragano T, Inoue T, Yoh K, Shin J, Fujita Y, Yoshiya K, Kim JI, Sakai R, Sekita K, Goto T, Fukagawa M, Nakanishi T. Effectiveness of beta(2)-microglobulin adsorption column in treating dialysis-related amyloidosis: a multicenter study. Blood Purif. 2011;32:317–22.
Kutsuki H. beta(2)-Microglobulin-selective direct hemoperfusion column for the treatment of dialysis-related amyloidosis. Biochim Biophys Acta. 2005;1753:141–5.
Pham NM, Recht NS, Hostetter TH, Meyer TW. Removal of the protein-bound solutes indican and p-cresol sulfate by peritoneal dialysis. Clin J Am Soc Nephrol. 2008;3:85–90.
Lee CT, Kuo CC, Chen YM, Hsu CY, Lee WC, Tsai YC, Ng HY, Kuo LC, Chiou TT, Yang YK, Cheng BC, Chen JB. Factors associated with blood concentrations of indoxyl sulfate and p-cresol in patients undergoing peritoneal dialysis. Perit Dial Int. 2010;30:456–63.
Schulman G, Agarwal R, Acharya M, Berl T, Blumenthal S, Kopyt N. A multicenter, randomized, double-blind, placebo-controlled, dose-ranging study of AST-120 (Kremezin) in patients with moderate to severe CKD. Am J Kidney Dis. 2006;47:565–77.
Schulman, G, Berl, T, Beck, GJ, Remuzzi, G, Ritz, E, Arita, K, Kato, A, Shimizu, M: Randomized placebo-controlled EPPIC trials of AST-120 in CKD. J Am Soc Nephrol. 2014.
Akizawa T, Asano Y, Morita S, Wakita T, Onishi Y, Fukuhara S, Gejyo F, Matsuo S, Yorioka N, Kurokawa K, Group C-KS. Effect of a carbonaceous oral adsorbent on the progression of CKD: a multicenter, randomized, controlled trial. Am J Kidney Dis. 2009;54:459–67.
Ueda H, Shibahara N, Takagi S, Inoue T, Katsuoka Y. AST-120 treatment in pre-dialysis period affects the prognosis in patients on hemodialysis. Ren Fail. 2008;30:856–60.
Yamamoto S, Kazama JJ, Omori K, Matsuo K, Takahashi Y, Kawamura K, Matsuto T, Watanabe H, Maruyama T, Narita I. Continuous reduction of protein-bound uraemic toxins with improved oxidative stress by using the oral charcoal adsorbent AST-120 in haemodialysis patients. Sci Rep. 2015;5:14381.
Tijink MS, Wester M, Glorieux G, Gerritsen KG, Sun J, Swart PC, Borneman Z, Wessling M, Vanholder R, Joles JA, Stamatialis D. Mixed matrix hollow fiber membranes for removal of protein-bound toxins from human plasma. Biomaterials. 2013;34:7819–28.
Meyer TW, Peattie JW, Miller JD, Dinh DC, Recht NS, Walther JL, Hostetter TH. Increasing the clearance of protein-bound solutes by addition of a sorbent to the dialysate. J Am Soc Nephrol. 2007;18:868–74.
Authors’ contributions
SY, JK, and IN made substantial contributions to the conception and design for this review article. SY involved in drafting the manuscript. TW, YT, YK, and SG revised the manuscript critically for important intellectual content. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Yamamoto, S., Kazama, J.J., Wakamatsu, T. et al. Removal of uremic toxins by renal replacement therapies: a review of current progress and future perspectives. Ren Replace Ther 2, 43 (2016). https://doi.org/10.1186/s41100-016-0056-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41100-016-0056-9