
Abstract
Background
We aimed to systematically review the efficacy of mannitol (MTL) on patients with acute severe traumatic brain injury (TBI).
Methods
Databases such as PubMed (US National Library of Medicine), CENTRAL (The Cochrane Library 2014, Issue 3), ISI (Web of Science: Science Citation Index Expanded), Chinese Biomedicine Database (CBM), and China Knowledge Resource Integrated Database (CNKI) have been searched for relevant studies published between 1 January 2003 and 1 October 2014. We have established inclusion and exclusion criteria to identify RCTs, which were suitable to be enrolled in the systematic review. The comparison group could be hypertonic saline (HS), hydroxyethyl starch, or others. The quality assessment was based on the Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 and modified Jadad score scale. The major outcome was mortality, followed by the secondary outcomes such as neurological outcome, days on intensive care unit (ICU), and ventilator day. In addition, intracranial pressure (ICP), cerebral perfusion pressure (CPP), and mean arterial pressure (MAP) were used as the surrogate endpoints. Data synthesis and meta-analysis was conducted by using R (version 3.7-0.).
Results
When 176 potential relevant literatures and abstracts have been screened, four RCTs met all the inclusion criteria and were enrolled for the meta-analysis. Amongst all the enrolled studies, two trials have provided the primary outcome data. There was no heterogeneity between two studies (I 2 = 0 %) and a fixed model was used for meta-analysis (n = 53), pooled result indicated that the mortality was similar in mannitol intervention and control treatment, OR = 0.80, 95 % CI [0.27, 2.37], P = 0.38. We found that both mannitol and HS were efficient in decreasing the ICP. Furthermore, the effect of the HS on the ICP appeared to be more effective in the patients with diffuse brain injuries than mannitol did.
Conclusions
As a conclusion, the mannitol therapy cannot reduce the mortality risk of acute severe traumatic brain injury. Current evidence does not support the mannitol as an effective treatment of acute severe traumatic brain injury. The well-designed randomized controlled trials are in urgent need to demonstrate the adoption of mannitol to acute severe traumatic brain injury.
Similar content being viewed by others
Background
Dehydration treatment is one of the main interventions that are adopted to prevent herniation of intracranial hypertension. Mannitol is widely used in China as a dehydrating agent in traumatic brain injury (TBI) patients with intracranial hypertension. Earlier studies indicated that dehydration therapy might decrease the intracranial pressure (ICP) of patients with TBI by reducing cerebral edema [1]. However, the excessive dosage of mannitol will penetrate from the blood into the brain, where it might cause the increase of the intracranial pressure (rebound phenomenon) and introduce the secondary brain cells damage accordingly [2, 3]. Therefore, the effectiveness of the treatment of mannitol for the intracranial hypertension in TBI is controversial [4, 5]. After the 1990s, a few new dehydration products have been introduced as the ICP reduction mediums, such as the hypertonic saline (HS) and the colloidal solution. Some clinical trials have shown that the hypertonic saline is more effective than mannitol in reducing the intracranial pressure and increase the cerebral perfusion pressure [5, 6]. However, there are studies with various results and conclusions [7, 8]. Single clinical trial usually has disadvantages by its sample size, design, or conduction. Clinical practitioners are puzzled by the chaos of the conflicted evidences and opinions to this end. The widespread use of mannitol is in great need of clarity optimal administration. There is uncertainty over the effectiveness of mannitol when compared to other ICP-lowering agents and other treatment without dehydrating agents. As a result, a systematic review is in urgent need, and this is why we present this study.
Methods
Strategy of data retrieving
Published literatures on the use of mannitol in severe traumatic brain injury patients were retrieved in the following databases: PubMed (US National Library of Medicine), The Cochrane Library (2014, Issue 3), ISI (Web of Science: Science Citation Index Expanded), Chinese Biomedicine Database (CBM), and China Knowledge Resource Integrated Database (CNKI). Letters have been sent to the first authors of the reports, asking them to assist in identifying any further trials that may have been conducted by them but not been reported publicly. Eligibility was determined by reading the reports of possible trials. The terms and strategies of retrieving are listed in the Table 1.
Inclusion criteria
Studies evaluating adult trauma patients with severe traumatic brain injuries and which included mannitol as an intervention were evaluated. The following data were required for inclusion: (1) study design: only RCTs set up with parallel control groups were selected, excluding self-control or crossover trials;(2) type of patients: adult trauma patients (age ≥18 years); (3) severe brain injures (Glasgow coma score <8) with cerebral edema. When indexes of the two groups such as genders, ages, pre-treatment ICP, osmolality levels, and Glasgow scores were matched, then the two groups were comparable; (4) intervention: the treatment group received mannitol in any dose for any duration, while the comparison group could be placebo controlled, different dose, different agent, or no agent; (5) reported one or more outcomes as following: (a) primary outcome: the mortality and (b) secondary outcome: (i) days on ICU and (ii) ventilator day; and (6) surrogate endpoints: ICP, cerebral perfusion pressure (CPP), and mean arterial pressure (MAP). The mortality is related with secondary and surrogate outcomes, so we collect them in the study.
Exclusion criteria
The following data were required for exclusion: (1) non-RCTs; (2) age ≤17 years, diagnosis of stroke, brain tumors, and non-traumatic brain injuries; (3) crossover studies; (4) did not address any primary or secondary outcomes as mentioned above; and (5) for those studies that did not describe the randomization methods, we attempted to contact the original authors. If the original authors did not provide a response or the randomization method proved inadequate, the articles were excluded.
Methodological quality evaluation
The methodological quality assessment table was based on the Cochrane Reviewers’ Handbook [9] and the modified Jadad scale [10, 11]. Data synthesis was conducted by R (R package version 3.7-0.) [12]. We followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement to report the research protocol, outcome, and relevant items in this systematic review [13].
Limitations of the study
Though there are many published literatures regarding the use of mannitol in severe traumatic brain injury patients, few of them have met the high quality standards of evidence-based medicine. There is insufficient reliable evidence to make suggestions on the administration of mannitol and many unanswered questions on the optimal use of mannitol in severe traumatic brain injury patients.
Results and discussion
Study identification and selection
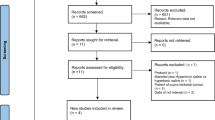
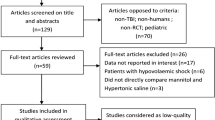
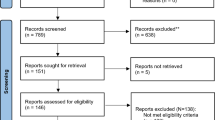
There were in total 176 potentially relevant titles, abstracts, and articles that have been screened. Initial screening resulted in 42 candidate studies [4, 5, 8, 14–52]. Figure 1 shows the details of the selection process and the reasons for exclusion. There were four trails that met all inclusion criteria and were included in the final meta-analysis. The characteristics of these included trials are listed in Tables 2 and 3.

Literature searching and selection
Major outcome: mortality
Amongst all the enrolled studies, Vialet et al. [49] and Harutjunyan et al. [50] have provided the primary outcome (mortality) (Table 4, Fig. 2). There is no heterogeneity between two studies (I 2 = 0 %), and a fixed model was used for the meta-analysis (n = 53), pooled result indicated that the mortality was similar in mannitol intervention and control treatment, OR = 0.80, 95 % CI [0, 27, 2.37], P = 0.38.

Comparison 1: mannitol versus hypertonic saline. Outcome 1 mortality
Secondary outcomes
In terms of the report of the secondary outcomes and surrogate endpoints, four RCTs were not uniformed and the data synthesis was not available. Hence, we have conducted a qualitative analysis afterward. There was no difference between two groups in neurological outcome (Glasgow outcome scale (GOS) 5/10 vs. 6/10; P >0.05) and days on ICU (23.3 ± 14.8 vs. 22.8 ± 15.5; P >0.05). No trial reported ventilator day.
Surrogated endpoints
ICP
Mannitol therapy may have a detrimental effect on decrease ICP when compared to hypertonic saline therapy. Vialet et al. [49] compared 20 % mannitol group with 7.5 % HS group. The result suggested that the mean number (13.3 ± 14.6 vs. 6.9 ± 5.6 episodes) of intracranial hypertension episodes (ICP >25 mmHg) per day and the daily duration (131 ± 123 vs. 67 ± 85 min) of intracranial hypertension episodes were significantly higher in the mannitol group (P <0.01) than those in the HS group [49]. The rate of clinical failure was also significantly higher in the mannitol group (7 of 10 vs. 1 of 10 patients; P <0.01) than that in the HS group [49]. Harutjunyan et al. [50] compared 15 % mannitol to 7.2 % hypertonic saline hydroxyethyl starch 200/0.5 (7.2 % NaCl/HES 200/0.5). NaCl/HES 200/0.5 (7.2 %) caused a greater decrease in the ICP than mannitol did (57 vs. 48 %; P <0.01) [50]. Both groups decreased the ICP to below 15 mmHg; but the mean time was significantly longer in the mannitol group (8.7 vs. 6 min; P <0.01) than that in the HS group. Francony et al. [51] and Cottenceau et al. [52] have shown that the spectrum of the ICP decrease was significantly larger in the HS group than in the mannitol group, and the spectrum was about 10 % over the entire stage. The changes of ICP across the four studies are summarized in Table 5.
CPP
Mannitol therapy may have a small detrimental effect in increasing CCP when compared to hypertonic saline therapy. Mannitol therapy may only have a beneficial effect in improving the blood supply of local brain tissue. Vialet et al. [49] has indicated that there was no significant difference in the mean number (3.1 ± 3.6 vs. 4.0 ± 4.6 episodes) of cerebral perfusion hypotension episodes (CPP <70 mmHg) per day and the daily duration (62 ± 107 vs. 52 ± 83 min) of cerebral perfusion hypotension episodes between the two groups (P >0.05) [49]. Harutjunyan et al. [50] has shown that the CPP had significantly sharp increase in both groups after the start of the infusion (P <0.0001), and the HS group was significantly higher than the mannitol group at 30 min after the beginning of the infusion (P <0.05) [50]. The maximum increase occurred at 30 min after the beginning of the infusion in both groups, and the HS group increased more than the mannitol group did (27 vs. 18 %; P <0.05) [50]. Francony et al. [51] suggested that mannitol could only effectively improve the CPP and the blood supply of the local brain tissue [51]. Cottenceau et al. [52] suggested that the maximum of CPP increase occurred at 30 min after the beginning of the infusion in both groups, but there was no significantly difference between the 20 % mannitol and the 7.5 % HS group [52]. The changes of CCP across the four studies are summarized in Table 6.
MAP
Mannitol therapy may have no beneficial effect in increasing MAP when compared to hypertonic saline therapy. Harutjunyan et al. [50] shown that MAP had a significantly sharp increase in 15 % mannitol and 7.2 % NaCl/HES 200/0.5 after the beginning of the infusion (P <0.05). There was no significant difference in the increase of MAP between two groups (5.8 vs. 7.6 %), but the maximum increase occurred significantly shorter in the mannitol group than in the HS group (10 vs. 30 min) [50]. Francony et al. [51] and Cottenceau et al. [52] have shown in their research that there was no significant difference in MAP between the 20 % mannitol and the 7.5 % HS. The changes of MAP across the four studies are summarized in Table 7.
Plasma osmolality, urine, and serum sodium
Mannitol therapy may have no difference in elevating the plasma osmolality and serum sodium when compared to hypertonic saline therapy. Mannitol therapy may have a small beneficial effect in increasing the urine output. But the single trial was too small for reliable conclusion. Vialet et al. [49] suggested that the plasma osmolality and serum sodium elevated significantly in both the 20 % mannitol group and the 7.5 % HS group after the beginning of the infusion (P <0.05), but there was no significant difference between the two groups. Harutjunyan et al. [50] showed the serum sodium increased in both the 15 % mannitol and the 7.2 % NaCl/HES 200/0.5 (P <0.05), although there was no significant difference between the two groups. Francony et al. suggested that mannitol caused a significantly greater increase in urine output (P 0.05) than HS [51]. Cottenceau et al. suggested that the HS caused a significantly greater increase of serum sodium (P = 0.0000), although mannitol caused a significantly decrease of it (P = 0.0000) [52]. The changes of plasma osmolality and sodium across the four studies are summarized in Table 8.
Conclusions
Published literatures regarding the use of mannitol in severe traumatic brain injury patients have rarely met the high quality standards of evidence-based medicine. This systematic review has revealed that the mannitol therapy cannot reduce death risk for TBI patients suffering from raised ICP.
Four RCTs retrieved by this study which have found reduced intracranial pressure (ICP): two RCTs suggested that hypertonic saline was superior to mannitol, and the time of maximized effect was earlier than that of mannitol; whilst the other two RCTs have proposed mannitol was equally on the impact of ICP comparing with hypertonic saline. In the elevation of CPP and MAP, one RCT found that hypertonic saline was superior to mannitol, whilst the other three RCTs considered no significant difference between the two agents. One RCT showed that mannitol might have a beneficial effect on cerebral hemodynamic when compare to hypertonic saline. However, some domestic studies have shown that the 23.4 % HS have faster and longer effect than the 20 % mannitol did in the treatment of raised ICP of severe brain injury [53–56]. Thus, the points of those researchers on this issue are varied and contradicted with each other.
Currently, mannitol is widely used as a part of conventional therapy of the TBI patients who suffer from intracranial pressure hypertension. Based on the most credible evidence from this study, mannitol therapy cannot reduce the mortality risk in this type of patients. Well-designed randomized controlled trials are urgently needed to demonstrate the efficacy of mannitol to acute severe traumatic brain injury.
Abbreviations
- CI:
-
confidence interval
- CPP:
-
cerebral perfusion pressure
- GCS:
-
Glasgow coma score
- HES:
-
hydroxyethyl starch
- HS:
-
hypertonic saline
- ICP:
-
intracranial pressure
- ICU:
-
intensive unit care
- MAP:
-
mean arterial pressure
- OR:
-
odds ratio
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RCT:
-
randomized controlled trial
- TBI:
-
traumatic brain injury
References
Archer DP, Freymond D, Ravussin P. Use of mannitol in neuro anesthesia and neuro intensive care. Ann Fr Anesth Reanim. 1995;14:77–82.
Oken DE. Renal extrarenal consideration in high-dose mannitol therapy. Ren Fail. 1994;16:147–59.
Kaufmann AM, Cardoso ER. Aggravation of vasogenic cerebral edema by multiple-dose mannitol. Neurosurg. 1992;77:584–9.
WakaiA MCA, Roberts I. Mannitol for acute traumatic brain injury. Cochrane Database SystRev. 2013;8:CD001049.
Jiang W-Q, Zeng H-K, Chen C-B. Comparison between HS with mannitol in the treatment of intracranial hypertension: a systematic review. J Evidence Based Med. 2008;10:279–83.
Sun M, Liu J, Jiang H, Peng J, Cai B, Hu W, et al. Hypertonic solution dose not decrease mortality from traumatic hemorrhagic shock: a systematic review and meta-analysis based on randomized control trials. Chin J Emerg Med. 2014;11:195–8.
Liang J-T, Peng Y-Q, Ke B-F. The clinical study of repeated use of mannitol to treat intracranial hypertension of the patients with severe craniocerebral injury. Int J Clin Exp Med. 2008;7:23–4.
Tan X, Zhang Z-P, Chen C-Y. Clinical analysis of alternate use of hypertonic saline and mannitol in treatment of postoperative intracranial hypertension in severe traumatic brain injury. Chin Modern Med. 2013;20:82–3.
Higgins JPT. Cochrane handbook for systematic reviews of interventions version 5.0.1. The Cochrane Collaboration. 2008. http://www.Cochrane-handbook.org. Accessed 19 May 2015.
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary. Control Clin Trials. 1996;17:1–12.
Min G, Liu F, Zhai S, Zhu JS, Zhang H, Wang T. Salbutamol in preventing preterm labour: a systematic review. Chin J Evid Based Med. 2007;7:591–600.
Guido Schwarzer. 2014. Meta: meta-analysis with R. R package version 3.7-0. http://CRAN.R-project.org/package=meta. Accessed 19 May 2015.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. doi:10.1371/journal.pmed1000097.
Liu H, Xu P, Gao R, et al. The effect of 3 % hypertonic saline in intracranial pressure decreasing of patients with severe traumatic brain injury. Jiangsu Med J. 2008;34:520–1.
Mao X, Feng D, Ye F. Comparison of mannitol with hypotonic saline in treatment of traumatic brain edema associated with intracranial hypertension. Jiangsu Med J. 2007;33:452–4.
Schwarz S, Schwab S, Bertram M, Aschoff A, Hacke W. Effects of hypertonic saline hydroxyethyl starch solution and mannitol in patients with increased intracranial pressure after stroke. Stroke. 1998;29:1550–5.
Ichai C, Armando G, Orban JC, Berthier F, Rami L, Samat-Long C, et al. Sodium lactate versus mannitol in the treatment of intracranial hypertensive episodes in severe traumatic brain-injured patients. Intensive Care Med. 2009;35:471–9.
Soustiel JF, Mahamid E, Chistyakov A, Shik V, Benenson R, Zaaroor M. Comparison of moderate hyperventilation and mannitol for control of intracranial pressure control in patients with severe traumatic brain injury—a study of cerebral blood flow and metabolism. Acta Neurochir (Wien). 2006;148:845–51.
Wakai A, Roberts IG, Schierhout G. Mannitol for acute traumatic brain injury. Cochrane Database Syst Rev. 2007;24(1):CD001049.
Marshall LF, SMith RW, Rauscher LA. Mannitol dose requirements in brain-injured patients. J Neurosurg. 1978;48:584–9.
Roberts IG, Schierhout G, Wakai A. Mannitol for acute traumatic brain injury. Cochrane Database Syst Rev. 2003;2:CD001049.
Li R, Wang J, Wang X. Effects of 7.5 % hypertonic saline on brain edema after severe traumatic brain injury. J Med Sci Central South China. 2012;40:487–9.
Shen X, Wang H. Systematic review of the safety and efficacy of hypertonic saline and mannitol treatment of intracranial hypertension. Chin Med Herald. 2011;8:11–3.
Bin X, Jian-guo LI, Zhang C-J, et al. Effects of hypertonic saline and treatment of acute intracranial hemorrhage: comparative study of 12 cases. Chin J Emergency Resuscitat Disaster Med. 2010;5:731–3.
Lei M, Guan Z-L, Yang G-S. Hypertonic saline treatment of traumatic intracranial hypertension. Chin J Med Guide. 2010;6:982–3.
Chai F, Luo X, Liang MA. Efficacy of using hypertonic saline and mannitol for cerebral edema. Chin J Mod Drug Appl. 2009;3:23–4.
Zhang B, Ke J. Comparative analysis of the treatment of using 3 % hypertonic saline, mannitol, glycerol and fructose for intracranial hypertension. Chin Manipul Rehabil Med. 2011;4:93.
Zeng H, Li H, Sun C, et al. Applied research of hypertonic saline in intracranial hypertension. Chin J Emerg Med. 2004;13:264–6.
Lin W. Study on efficiency of treatment of elevated intracranial pressure of severe head injury patients with 3 % hypertonic saline. West China Med J. 2009;24:1349–51.
Sayre MR, Daily SW, Stern SA, Storer DL, van Loveren HR, Hurst JM, et al. Out-of-hospital administration of mannitol to head-injured patients does not change systolic blood pressure. Acad Emerg Med. 1996;3:840–8.
BattisonC APJ, GrahamC PT. Randomized, controlled trial on the effect of a 20 % mannitol solution and 7.5 % saline/6 % dextran solution on increased intracranial pressure after brain injury. Crit Care Med. 2005;33:196–202.
Cruz J, Minoja G, Okuchi K, Facco E. Successful use of the new high-dose mannitol treatment in patients with Glasgow coma scale scores of 3 and bilateral abnormal pupillary widening: a randomized trial. J Neurosurg. 2004;100:376–83.
Chen T, Quan K, Cai J. Clinical study on application of 3 % hypertonic saline in treatment of severe traumatic brain injury with different administration methods. J J Traumatic. 2011;16:433–6.
Xiu J, Liu X, Chen G. Clinical studies in patients with traumatic brain injury intracranial pressure with 20 % piracetam. Chin J Clin Neur. 2011;16:553–4.
Chen Z. Observation of oxygen utilization of using dehydrating agent for severe traumatic brain injury. J Clin Emerg. 2008;9:111–3.
Jianling LI. Clinical observation of piracetam injection to reduce of 286 patients of raised intracranial pressure. Xinjiang Med. 2012;42:88–9.
Deng R, Fan H, Chen J. Effects of glycerol fructose or mannitol in treating intracranial hypertension induced by craniocerebral injury. J Med Res. 2010;39:98–100.
Jianke LI. Glycerin fructose and mannitol treatment after craniocerebral injury of intracranial pressure clinical curative effect analysis. Chin Foreign Treatment. 2013;8:108–10.
Yang Z-G, Gong Y, Zhou M-H. Clinical observation of hypertonic sodium chloride hydroxyethyl starch 40 injection in treating traumatic brain injury. Modern Med J. 2011;39:149–52.
Zhou Y-B, Jiang Y-G, Zhang L-Y. Curative effect of hypertonic saline on severe traumatic brain injury with shock. J Trauma Surg. 2007;9:211–4.
Yan Y-F, Yao H-B, Shen X. Hypertonic saline for the treatment of intracranial hypertension due to traumatic brain edema. J Trauma Surg. 2013;15:296–300.
Lian W, Wang R-Z, Ren Z-Y. Clinical study of Kangrong injection on high intracranial pressure in patients with intracranial diseases. Chin J Clin Neuro Surg. 2006;11:734–6.
Long R-F, Xiao-lin X, Chen Y-F. Clinical analysis of continuous infusion of 10 % hypertonic saline in the treatment of traumatic intracranial hypertension. Hainan Med J. 2011;22:9–11.
Deng Q. Clinical application of piracetam injection to reduce intracranial pressure. Guide Chin Med. 2010;8:124–5.
Yao Z-G, Sun XL, Xi Z-Q. Clinical observation of curative effect of 7.5 % hypertonic saline solution on patients with severe craniocerebral injury. Chin J Clin Neuro Surg. 2008;13:205–7.
Han B, Huo L, et al. Clinical analysis of using hypertonic saline to rescue 32 cases of patients with acute intracranial hypertension. Clin Med Chin. 2005;21:534–5.
Smith HP, Kelly JR, McWhorter JM. Comparison of mannitol regiments in patients with severe head injury undergoing intracranial monitoring. Jc Neurosurg. 1986;65:820–4.
Nordby HK, Nesbakken R. The effect of high dose barbiturate decompression after severe head injury. a controlled clinical trial. Acta Neurochir (Wien). 1984;72:157–66.
Vialet R, Albanèse J, Thomachot L. Isovolume hypertonic solutes (sodium chloride or mannitol) in the treatment of refractory posttraumatic intracranial hypertension: 2 mL/kg 7.5 % saline is more effective than 2 mL/kg 20 %. Crit Care Med. 2003;31:1683–7.
Harutjunyan L, Holz C, Rieger A, Menzel M, Grond S, Soukup J. Efficiency of 7.2 % hypertonic saline hydroxyethy/starch 200/0.5 versus mannitol 15 % in the treatment of increased intracranial pressure in neurosurgical patients - a randomized clinical trial. Crit Care. 2005;9:R530–40.
Francony G, Fauvage B, Falcon D, Canet C, Dilou H, Lavagne P, et al. Equimolar doses of mannitol and hypertonic saline in the treatment of increased intracranial pressure. Crit Care Med. 2008;36:795–800.
Cottenceau V, Masson F, Mahamid E, Petit L, Shik V, Sztark F, et al. Comparison of effects of equiosmolar doses of mannitol and hypertonic saline on cerebral blood flow and metabolism in traumatic brain injury. J Neurotrauma. 2011;28:2003–12.
Hongke Z, Hui LI. The use of 23.4 % hypertonic saline in the treatment of intracranial hypertension. Chin J Emerg Med. 2002;11:176–8.
Zeng H, Deng Y, Zhang Y. Clinical analysis of using 10 % hypertonic saline in treatment of acute cerebrovasvular diseases. Chin J Emerg Med. 2007;16:155–7.
Heng Y, Hongke Z, Hui L. Clinical studies of continuous use 23.4 % hypertonic saline treatment of intracranial hypertension. Guangdong Med J. 2005;26:483–4.
Zeng H, Ye H, Li H, et al. The infection different degree intracranial hypertension by 23.4 % hypertonic saline. Lingnan. J Emerg Med. 2004;9:83–5.
Acknowledgements
The authors appreciate Mr. Andrew He of University of Waikato for his generous help on the manuscript writing and proofreading.
Funding
This work was supported by grants from Sichuan Provincial Department of Science and Technology (No. 2012SZ0181, SZ20120209) and grants from Chengdu Municipality Department of Science and Technology (11PPYB099SF-289 AND 12PPYB181SF-002). Funders play no role on the study design, conduct, and manuscript writing.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
Study design and conception of this manuscript were performed by KW, M-WS, HJ, and JZ. Literature retrieving and study selection were performed by KW and M-WS. KW, HJ, and X-PC performed quality evaluation of the study. Mathematical modeling and meta-analysis are conducted by KW, JZ, and HJ. Results analysis and interpretation are done by M-WS, HJ, X-PC, and JZ. The manuscript was drafted by KW, M-WS, and HJ. KW, and M-WS contributed equally to this work. All authors read and approved the final manuscript.
Kai Wang and Mingwei Sun contributed equally to this work.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Wang, K., Sun, M., Jiang, H. et al. Mannitol cannot reduce the mortality on acute severe traumatic brain injury (TBI) patients: a meta–analyses and systematic review. Burn Trauma 3, 8 (2015). https://doi.org/10.1186/s41038-015-0006-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41038-015-0006-8