
Abstract
Background
The conventional transcervical resection for submandibular gland disease has some risks and an unsatisfactory cosmetic result. Recently, robot-assisted surgery has been developed as a plausible substitute for conventional surgery which provides an excellent cosmetic outcome.
Case presentation
The authors performed robot-assisted sialadenectomy via modified facelift incision using the da Vinci Xi surgical system (Intuitive Surgical Inc., CA, USA) with two endowrist arms (monopolar curved scissors and Maryland bipolar forceps) successfully in a 44-year-old female patient who suffered from sialolith and severe atrophic submandibular gland.
Conclusions
If similar studies are done in the future, this robot-assisted sialadenectomy may become established as an alternative to existing disadvantageous surgical methods.
Similar content being viewed by others


Background
The submandibular gland is vulnerable to non-neoplastic disorders (sialolithiasis and sialadenitis) due to its anatomic characteristics. The most common benign neoplasm is pleomorphic adenoma, and tumors of the submandibular gland are infrequently malignant [1]. The conventional treatment method of transcervical resection has some risks such as paresis of the marginal branch of the facial nerve, lingual nerve paresis, xerostomia, and an unsatisfactory cosmetic result [2]. Notwithstanding various techniques such as intraoral resection [3, 4] and endoscopic-assisted resection [5, 6] to reduce these complications, there are still postoperative discomforts, such as a temporary lack of function of lingual nerve and a temporary limitation of tongue movement [3]. Recently, robot-assisted surgery has been developed as a plausible substitute for conventional surgery which provides an excellent cosmetic outcome [7, 8]. Earlier robot-assisted surgeries were performed via a retroauricular approach [7], recent surgeries are being performed via modified facelift incision (MFI) approach [9,10,11], the postoperative scar being completely hidden by the auricle and hair. In this paper, the authors report a case of robot-assisted submandibular sialoadenectomy via MFI.
Case presentation
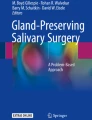
A 44-year-old female presented with a chief complaint of 3-year history of recurrent pain and intermittent swelling to the left mandibular region. The swelling was usually worsened by meals, extreme pain arising once a month. When the pain started, it lasted about 10 min, with an NRS (numeric rating scale) score of 10. She had recently begun to have pain every 4 h. On examination, there was a tense and sensitive submandibular salivary gland and visible swelling in the posterior part of the left side of submandibular area. No salivary flow was appreciated from the left submandibular duct. The radiograph showed an elongated radiopaque structure imposed on the left submandibular area (Fig. 1 top). Computerized tomographic (CT) scan of the mandibular region showed the presence of multiple high attenuated materials and elongated sialolith located within the left Wharton’s duct. Also, very severe atrophic submandibular gland was found (Fig. 1 bottom).

The panoramic radiograph showed an elongated radiopaque structure imposed on the left submandibular area (top). Computerized tomographic (CT) scan of the mandibular region showed the presence of multiple high attenuated materials and elongated sialolith located within the left Wharton’s duct. Very severe atrophic submandibular gland was also found (bottom).
Preoperative technetium-99m pertechnetate salivary gland scintigraphy revealed that other salivary glands were within normal limits, but with no definite radiotracer excretion in the Lt. submandibular gland (Fig. 2).

Preoperative technetium-99m pertechnetate salivary gland scintigraphy revealed that right salivary glands were within normal limits but with no definite radiotracer excretion in the Lt. submandibular gland
Surgical procedures
The patient was placed on the operating table in supine position and was induced with short-acting paralytics to allow for monitoring of the branches of the facial nerve during dissection. General anesthesia was obtained via oral endotracheal intubation. The neck was extended with the placement of a shoulder roll, and the head was turned to the opposite side of the involved parotid. The patient was prepared and draped in a sterile fashion. The ipsilateral commissure of the mouth was prepared as readily visible. The incision line was marked (standard modified facelift incision). 2% lidocaine with epinephrine was injected within the subcutaneous tissues of the proposed surgical incision, involving a standard preauricular curvilinear incision which begins at the tragus, going around the inferior border of the lobule and then continuing backwards in the auriculomastoid groove. The superior aspect of the postauricular incision reached to the level of the superior aspect of the mastoid and then was extended posteriorly into the hair line of the neck for cosmesis (Fig. 3 left).

Modified facelift incision (MFI) for robot-assisted submandibular gland excision (left) and obtaining a sufficient amount of working space (approximately 10-cm height) for securing a self-retaining retractor (right)
After skin incision, the subplatysmal skin flap is elevated just above the sternocleidomastoid (SCM) muscle using a monopolar electrocautery under direct vision. The greater auricular nerve and external jugular vein can be identified located superficial to the SCM muscle. The skin flap is elevated until the anterior extent reaches the midline of the anterior neck, the superior extent the inferior border of the mandible and the inferior extent the level of omohyoid muscle. Skin flap elevation below the mandible should be performed carefully to minimize injury to the nearby marginal branch of the facial nerve. Normally two assistant surgeons are required to comfortably lift up the skin flap with an Army-Navy retractor or a right-angle breast retractor. After obtaining a sufficient amount of working space (approximately 10-cm height), a self-retaining retractor is applied through the space and is secured [12, 13] (Fig. 3 right). Dissection began at the lower border of the SMG using the da Vinci Xi surgical system (Intuitive Surgical Inc., CA, USA) with two endowrist arms (monopolar curved scissors & Maryland bipolar forceps) (Fig. 4 left). The proximal facial artery was ligated with vascular clips, the lingual nerve was separated from the submandibular ganglion with monopolar cautery, and Wharton’s duct was ligated with a vascular clip. The lingual and hypoglossal nerves were well preserved. The specimen was well excised, the surgical bed irrigated with warm saline and bleeding control under both robot view and direct vision was performed (Fig. 4 right). A close suction drain was inserted posterior to the hairline incision, and the wound was closed with Dermabond skin adhesive (Ethicon, USA) after subcutaneous layer suture. The pathologic report was sialolith with ductal atrophy. There was no postoperative complication.

Dissection using the da Vinci Xi surgical system (Intuitive Surgical Inc., CA, USA) with two endowrist arms (monopolar curved scissors and Maryland bipolar forceps) (left) and excised specimen (right)
Conclusions
Since Terris et al. reported that modified facelift incision (MFI) is an alternative approach to parotidectomy for selected patients [14], there have been many reports on the versatility and esthetic advantages of MFI in various surgeries [15,16,17,18,19,20,21]. Various approaches have been proposed for the application of robotic surgery to the neck [22,23,24]. Since robotic cervical surgery using MFI was reported by Koh et al. [10], the usefulness of this approach has been affirmed, and even the cervical lymphadenectomy, is now being performed using a robot [25,26,27,28]. In this case, enough space was secured for robot operation during the approach using MFI, leaving a scar which was largely concealed by hair. Because the authors have already published a paper on endoscopic cervical lymphadenectomy [29], the advantages and disadvantages of using robots and endoscopes are clear to them. Compared with endoscopes, robots are more flexible, allowing for more free tissue detachment and the ability to perform uncomplicated operations with two arms. Three arms make operations much easier. In addition, it is possible to perform surgery in a more comfortable sitting position on the surgical console (Fig. 5) and since the visual field is three-dimensionally detailed and bright, it is possible to observe microscopic nerves and blood vessels rather than view them directly transcervically. Several types of robotic arms have been developed, but this operation is possible with only two types—monopolar curved scissors and Maryland bipolar forceps, ligation of blood vessels made possible with a robot arm or vascular clip. However, it cannot be felt when a structure like a mandible that restricts the movement of a robot arm is touched, so it is considered as a disadvantage that a surgical assistant should always observe it from the side. The cost is not likely to be an obstacle in choosing surgery, as patients have recently had a range of private insurance. The operation time was 3 h and 11 min, and it was not worse than open surgery for 2 h except for suture time. If one is familiar with endoscopic surgery, there should be no great difficulty. No specific postoperative complications were reported. In this case, the patient was discharged after the hemo-Vac discharge was reduced to 20 ml/day without any postoperative complications and showed great satisfaction with the operation results (Fig. 6). If similar studies are done in the future, this method may become established as an alternative to existing disadvantageous surgical methods.

The da Vinci Xi surgeon console

The patient shows stable nerve function and esthetic result at postoperative 3 months
References
Mizrachi A, Bachar G, Unger Y et al (2017) Submandibular salivary gland tumors: clinical course and outcome of a 20-year multicenter study. Ear Nose Throat J 96:E17–E20
Springborg LK, Moller MN (2013) Submandibular gland excision: long-term clinical outcome in 139 patients operated in a single institution. Eur Arch Otorhinolaryngol 270:1441–6
Hong KH, Kim YK (2000) Intraoral removal of the submandibular gland: a new surgical approach. Otolaryngol Head Neck Surg 122:798–802
Miloro M (1999) Intraoral submandibular gland excision. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 88:661–3
Guerrissi JO, Taborda G (2001) Endoscopic excision of the submandibular gland by an intraoral approach. J Craniofac Surg 12:299–303
Parente Arias PL, Fernandez Fernandez MM, Varela Vazquez P, de Diego MB (2016) Minimally invasive video-assisted submandibular sialadenectomy: surgical technique and results from two institutions. Surg Endosc 30:3314–20
Kim CH, Koh YW, Kim D, Chang JW, Choi EC, Shin YS (2013) Robotic-assisted neck dissection in submandibular gland cancer: preliminary report. J Oral Maxillofac Surg 71:1450–7
Lee HS, Park DY, Hwang CS et al (2013) Feasibility of robot-assisted submandibular gland resection via retroauricular approach: preliminary results. Laryngoscope 123:369–73
Koh YW, Choi EC (2014) Robotic approaches to the neck. Otolaryngol Clin North Am 47:433–54
Koh YW, Chung WY, Hong HJ et al (2012) Robot-assisted selective neck dissection via modified face-lift approach for early oral tongue cancer: a video demonstration. Ann Surg Oncol 19:1334–5
Kim JYKW, Choi EC, Nam W (2016) The role of virtual surgical planning in the era of robotic surgery. Yonsei Med J 57:265–8
Scott Magnuson EMG J, Kuppersmith RB (2016) Robotic Head and Neck Surgery. Thieme, New York
Eun Chang Choi YWK (2013) Atlas of head and neck surgery-endoscopic and robotic neck surgery. Panmun, Seoul
Terris DJTK, Fee WE Jr (1994) Modified facelift incision for parotidectomy. J Laryngol Otol 108:574–8
Lohuis PJTM, Bonte K, van den Brekel MW, Balm AJ, Vermeersch HB (2009) Superficial parotidectomy via facelift incision. Ann Otol Rhinol Laryngol 118:276–80
Wasson JKH, Yeo J, Panesar J (2010) Cervicomastoidfacial versus modified facelift incision for parotid surgery: a patient feedback comparison. Ann R Coll Surg Engl 92:40–3
Lee SYKY, Kim BG, Hong HJ, Jeong JH, Choi EC (2011) The extended indication of parotidectomy using the modified facelift incision in benign lesions: retrospective analysis of a single institution. World J Surg 35:2228–37
Lorenz KJBP, Höcherl D, Wilde F (2013) Improving the quality of life of parotid surgery patients through a modified facelift incision and great auricular nerve preservation. GMS Interdiscip Plast Reconstr Surg DGPW 16:1–7
Grover NDSA (2013) Facelift approach for parotidectomy: an evolving aesthetic technique. Otolaryngol Head Neck Surg 148:548–56
de Vicente JCG-GM, de Villalaín L, Fernández-Valle Á (2015) Modified facelift approach combined with a superficial musculoaponeurotic system flap in the treatment of benign parotid tumors. J Craniomaxillofac Surg 43:1655–61
Bulut OCPP, Federspil PA (2016) Modified facelift incision for partial parotidectomy versus bayonet-shaped incision: a comparison using visual analog scale. Eur Arch Otorhinolaryngol 273:3269–75
Kang SW, Jeong JJ, Yun JS et al (2009) Robot-assisted endoscopic surgery for thyroid cancer: experience with the first 100 patients. Surg Endosc 23:2399–406
Lee KE, Choi JY, Youn YK (2011) Bilateral axillo-breast approach robotic thyroidectomy. Surg Laparosc Endosc Percutan Tech 21:230–6
Richmon JD, Holsinger FC, Kandil E, Moore MW, Garcia JA, Tufano RP (2011) Transoral robotic-assisted thyroidectomy with central neck dissection: preclinical cadaver feasibility study and proposed surgical technique. J Robot Surg 5:279–82
Byrd JK, Duvvuri U (2013) Current trends in robotic surgery for otolaryngology. Curr Otorhinolaryngol Rep 1:153–7
Greer Albergotti W, Kenneth Byrd J, De Almeida JR, Kim S, Duvvuri U (2014) Robot-assisted level II-IV neck dissection through a modified facelift incision: initial North American experience. Int J Med Robot 10:391–6
Shin YS, Choi EC, Kim CH, Koh YW (2014) Robot-assisted selective neck dissection combined with facelift parotidectomy in parotid cancer. Head Neck 36:592–5
Albergotti WG, Byrd JK, Nance M et al (2016) Robot-assisted neck dissection through a modified facelift incision. Ann Otol Rhinol Laryngol 125:123–9
Kim JY, Cho H, Cha IH, Nam W (2014) Esthetic neck dissection using an endoscope via retroauricular incision: a report of two cases. J Korean Assoc Oral Maxillofac Surg 40:27–31
Funding
None.
Author information
Authors and Affiliations
Contributions
SWJ, YKK, and YHC participated in the operation and are responsible for the data collection, drafting of the article, and the critical revision of the article. WN is responsible for the conception and design of the study, the critical revision of the article, and the approval of the article. YWK gave us some advises about robot surgery. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the institutional review board of Yonsei Dental Hospital (IRB approval number 2-2017-0016).
Competing interests
The authors declare that they have no competing interests. The authors alone are responsible for the content and writing of the article.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Jung, S.W., Kim, Y.K., Cha, Y.H. et al. Robot-assisted submandibular gland excision via modified facelift incision. Maxillofac Plast Reconstr Surg 39, 25 (2017). https://doi.org/10.1186/s40902-017-0122-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40902-017-0122-4