
Abstract
Background
CrossFit is recognized as one of the fastest growing high-intensity functional training modes in the world. However, scientific data regarding the practice of CrossFit is sparse. Therefore, the objective of this study is to analyze the findings of scientific literature related to CrossFit via systematic review and meta-analysis.
Methods
Systematic searches of the PubMed, Web of Science, Scopus, Bireme/MedLine, and SciELO online databases were conducted for articles reporting the effects of CrossFit training. The systematic review followed the PRISMA guidelines. The Oxford Levels of Evidence was used for all included articles, and only studies that investigated the effects of CrossFit as a training program were included in the meta-analysis. For the meta-analysis, effect sizes (ESs) with 95% confidence interval (CI) were calculated and heterogeneity was assessed using a random-effects model.
Results
Thirty-one articles were included in the systematic review and four were included in the meta-analysis. However, only two studies had a high level of evidence at low risk of bias. Scientific literature related to CrossFit has reported on body composition, psycho-physiological parameters, musculoskeletal injury risk, life and health aspects, and psycho-social behavior. In the meta-analysis, significant results were not found for any variables.
Conclusions
The current scientific literature related to CrossFit has few studies with high level of evidence at low risk of bias. However, preliminary data has suggested that CrossFit practice is associated with higher levels of sense of community, satisfaction, and motivation.
Similar content being viewed by others


Key Points
-
For a large majority of studies, a low level of evidence and a high risk of bias were found. There is a need to improve the methodological approaches in further studies.
-
In the scientific literature, there is a gap to be filled in the area of controlling training load. Given the importance of managing training load in reducing injury risk and optimizing athletic performance, these approaches could be used to support CrossFit practice.
-
Initial reports of higher levels of sense of community, satisfaction, and motivation during CrossFit training were found in the scientific literature.
Background
CrossFit is recognized as one of the fastest growing modes of high-intensity functional training. According to the official CrossFit website (map.crossfit.com), CrossFit boxes are located in 142 countries across seven continents with more than 10,000 affiliates [1]. This strength and conditioning program is used to optimize physical competence in ten fitness domains: (1) cardiovascular/respiratory endurance, (2) stamina, (3) strength, (4) flexibility, (5) power, (6) speed, (7) coordination, (8) agility, (9) balance, and (10) accuracy [2]. CrossFit training is usually performed with high-intensity, functional movements called “workout of the day” (WOD) [3]. In these training sessions, high-intensity exercises are executed quickly, repetitively, and with little or no recovery time between sets [4]. With the focus on constantly varying functional movements, CrossFit training uses the main elements of gymnastics (e.g., handstand and ring exercises), weightlifting exercises (e.g., barbell squats and presses), and cardiovascular activities (e.g., running or rowing) as exercise tasks [5]. According to Glassman, who is the founder of CrossFit, the methodology that drives CrossFit training is entirely empirical. Furthermore, Glassman described that “meaningful statements about safety, efficacy, and efficiency, the three most important and interdependent facets of any fitness program, can be supported only by measurable, observable, repeatable facts, i.e., data” [3].
CrossFit is also considered an option for high-intensity interval training (HIIT). Consequently, HIIT has become one of the top 3 worldwide fitness trends since 2013 according to the American College Sports Medicine (ACSM) annual survey [6,7,8,9]. Notably, CrossFit was indicated as the primary reason HIIT workouts were ranked so high [6,7,8,9]. However, a consensus paper produced by the Consortium for Health and Military Performance (CHAMP) and ACSM associated a potential emergence of a high injury risk with programs such as CrossFit [10]. While positive influences on body composition and physical fitness were recognized, the consensus highlighted a “disproportionate musculoskeletal injury risk from these demanding programs, particularly for novice participants, resulting in lost duty time, medical treatment and extensive rehabilitation”. In addition, the consensus suggested the existence of a training paradigm requiring advanced level technique during maximal timed exercise repetitions without adequate rest intervals between sets, as well as an insufficient recovery time between high-volume loads and training sessions. This overload situation can lead to early fatigue, additional oxidative stress, less resistance to subsequent repetitive exercise strain, greater perception of effort, and unsafe movement execution [10]. Furthermore, this training context associated with inadequate training load progression increases the risk of overuse injury, overreaching, and overtraining. The consensus authors suggested, as a possible solution, individual monitoring of training load to minimize these risks [10]. Despite the proposed risks of CrossFit, others have suggested that high-intensity functional training programs, including CrossFit, have similar or lower potential for injury than many traditional physical training activities [11]. However, the authors also stated that controlling training volume must be done in order to reduce injury risk in military populations. For an effective training process and adaptation to occur, the monitoring [12], quantification [13], and regulation [14] of training load is necessary. However, managing training load poses a considerable challenge for sport scientists [15, 16]. Despite this challenge, managing training load is fundamental to achieving the objectives of reducing injury risk and optimizing sports performance [17,18,19,20,21,22].
Although there are a large number of CrossFit participants, empirical evidence demonstrating the improvements in physical fitness that arise from this form of training are far from substantive. Furthermore, an overview of CrossFit’s outcomes has not been verified. Therefore, the purpose of the present study was to analyze the findings of the scientific literature related to CrossFit through a systematic review and meta-analysis.
Methods
Literature Search
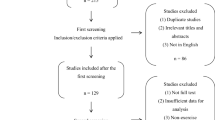
One author conducted the literature search, collated the abstracts, and applied the initial inclusion criteria. The keyword “CrossFit” was used during the electronic search. The following electronic databases were searched on the 25th of November 2016: PubMed, Web of Science, Scopus, Bireme/MedLine, and SciELO (Fig. 1). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines were adhered to in this manuscript. In the initial analysis, all CrossFit articles included in this manuscript were peer-reviewed and not limited to specific years or language. During the second phase of study selection, two authors reviewed and identified the titles and abstracts based on the inclusion criteria.

Study selection PRISMA flow diagram
Inclusion Criteria
To meet the inclusion criteria for the meta-analysis, studies investigating humans “in vivo” or “in obitus” and analyzed the effects of CrossFit as a training program were considered. The meta-analysis was only conducted on variables from short-term intervention studies (i.e., ≥ 3 weeks) with healthy male and/or female participants split into distinct gender groups (the procedures were consistent from those of another meta-analysis) [23]. Moreover, the variables analyzed were to be found in more than one study. If pertinent data were absent, authors were contacted and the necessary information requested via e-mail. If the original data were not provided by the authors, the mean and standard deviations were extracted from graphical representation using Ycasd [24] or estimated from the median, range, and sample size [25]. The remaining articles were included in the systematic review.
Study Quality
The Consolidated Standards of Reporting Trials (CONSORT) statement was adapted and used for checking the quality of reporting by two authors independently. Thus, the articles’ quality was evaluated based on the 25 items identified in the CONSORT criteria, providing a maximal possible score of 37. The CONSORT items are distributed in sections and topics such as “Title and abstract”; “Introduction” (Background and objectives); “Methods” (Trial design, Participants, Interventions, Outcomes, Sample size, Blinding, Statistical methods); “Results” (Participant flow, Recruitment, Baseline data, Numbers analyzed, Outcomes and estimation, Ancillary analyses, Harms); “Discussion” (Limitations, Generalizability, Interpretation); and “Other information” (Registration, Protocol, Funding) [26]. Additionally, the Oxford Levels of Evidence [27] were used to evaluate the level of evidence for all articles found in the literature on CrossFit. Where the five levels (i.e., Level 1 = systematic reviews; Level 2 = randomized controlled trials with low/moderate risk of bias or observational studies with dramatic effect; Level 3 = cohort study, non-randomized controlled trials with low/moderate risk of bias or randomized controlled trial at high risk of bias; Level 4 = case series, case report, case-control studies, cohort study, historically controlled studies or non-randomized controlled trials at high risk of bias; and Level 5 = mechanism-based reasoning/expert opinion) are determined based on the following questions: (i) “How common is the problem?”; (ii) “Is this diagnostic or monitoring test accurate? (diagnosis)”; (iii) “What will happen if we do not add a therapy? (prognosis)”; (iv) “Does this intervention help? (treatment benefits)”; (v) “What are the COMMON harms? (treatment harms)”; (vi) “What are the RARE harms? (treatment harms)”; and (vii) “Is this (early detection) test worthwhile? (screening)”.
Bias Analysis
For the systematic review, two authors independently assessed the quality of the included studies using the Cochrane risk of bias tool [28] with a priori formulated criteria adopted from the studies of Pas et al. [29] and Winters et al. [30]. Five domains of bias were appraised: selection bias (random allocation and allocation concealment), performance bias (blinding of personnel and participants), detection bias (blinding of outcome assessment), attrition bias (loss to follow-up), reporting bias (outcome reporting), and other biases. Each item was scored as low (+), high (−), or unclear (?) risk of bias. Studies were considered low risk of bias when all domains were scored as low risk of bias or if one item was scored as high risk or unable to determine. If two domains were scored as high or unable to determine risk of bias, the study received a moderate risk of bias. Finally, when more than two domains were scored as high risk of bias, the study was regarded to possess a high risk of bias. In case of disagreement between authors, consensus was sought during a consensus meeting. If no consensus was reached, a third author was asked to provide a final verdict. Publication bias was determined for the meta-analysis using an approach where differences in baseline assessments were checked for all intervention groups. Next, the interventions were divided into non-significant (p > 0.05) or significant (p < 0.05) results to determine the percentage of interventions with non-significant differences (these procedures were followed as per another meta-analysis) [23].
Statistical Analysis
For the meta-analysis, the heterogeneity of the included studies was evaluated by examining forest plots, confidence intervals (CI), and I2. I2 values of 25, 50, and 75 indicated low, moderate, and high heterogeneity, respectively [31]. Random effects were analyzed using the DerSimonian and Laird [32] approach. The meta-analysis was conducted based on the number of variables from short-term intervention studies. Statistical significance was set at p ≤ 0.05, and the magnitude of differences for each dependent variable was calculated using effect size (ES) with 95% CI [32]. The ES classification was large > 0.80; moderate = 0.20–0.80; small < 0.20 [33]. Inferential statistics were used for the descriptive analysis of the data. All data were analyzed using CMA v3 trial (Biostat, New Jersey, USA) and Excel 2010 worksheet (Microsoft, Washington, USA).
Results
The initial search found 204 articles (Fig. 1). When the inclusion criteria were applied, 32 articles were included in the systematic review. When the inclusion criteria were applied for the meta-analysis, five of these articles met the criteria and were included in the manuscript [4, 5, 34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63]. However, during this manuscript peer-reviewing process, one of 32 articles had a retraction published [64].
Quality assessment of the 31 included articles ranged from 22 to 84% with a mean CONSORT rating of 37% [26]. Only 9% (i.e., absolute number = 3) of the included articles [38, 53, 54] had ratings exceeding 50% (Additional file 1: Table S1). Ethical approval was obtained in all articles. The evidence level ranged between levels 2 and 4 for included articles. However, just 6% (i.e., absolute number = 2) of articles were considered level 2 (i.e., randomized controlled trials with low risk of bias) (Fig. 2) [53, 54].

Risk of bias and level of evidence
For the systematic review, only 6% of the assessed articles were at low risk of bias (Fig. 2) [53, 54]. These articles performed adequate randomization and allocation methods, blinding strategy, and clinical trial registry. In contrast, a majority of the non-controlled trials, cross-sectional studies based on an electronic questionnaire, and correlation studies or case report/case series did not explicitly describe if and how they controlled for detection bias. For the included articles in the meta-analysis, 78% of the intervention groups resulted in non-significant (p > 0.05) differences in baseline assessments (i.e., 83 interventions with non-significant differences ÷ 106 overall interventions = 78%).
The pooled sample size for this manuscript was 3597 with 81% of participants in the CrossFit group and the remaining 19% in the control group. Male participants (60%) were utilized more so than females (40%). CrossFit samples were composed of adolescents (male 4%, n = 112 and age = 15 ± 1 years; female 3%, n = 94 and age = 15 ± 1 years), adults (male 56%, n = 1638 and age = 30 ± 7 years; female 37%, n = 1065 and age = 30 ± 7 years), and elderly (male 0.2%, n = 5 and age > 60 years; female 0.1%, n = 2 and age > 60 years). The sample profile included 6% competitors (i.e., in the CrossFit Games), 63% trained individuals (i.e., in the CrossFit program more than 6 months), 22% physically active individuals, and 9% sedentary individuals. The average duration of each CrossFit intervention was 9 ± 3 weeks.
In summary, the following aspects of CrossFit were examined in the scientific literature: body composition (n = 4), psycho-physiological parameters (n = 12), musculoskeletal injury risk (n = 7), life and health aspects (n = 4), and psycho-social behavior (n = 11) (Table 1).
Among the included short-term intervention studies, five CrossFit fitness domains were found in the literature, i.e., cardiovascular/respiratory endurance [50, 53], stamina [50, 53], strength [53], flexibility [53], and power [50, 53]. Five domains were yet to be verified, i.e., speed, coordination, agility, balance, and accuracy.
Forty-three variables were found from short-term intervention studies in the meta-analysis. These variables represented cardiovascular/respiratory endurance and stamina (i.e., absolute and relative maximal oxygen consumption, VO2max), as well as body composition (i.e., body mass, body mass index, relative body fat, fat mass, lean body mass, and waist circumference). No significant results were found for any of the variables (Fig. 3).

Meta-analysis of short-term intervention studies
Discussion
Although CrossFit has a large number of participants, a high level of evidence demonstrating positive outcomes has yet to be established in the literature. Therefore, the present study aimed to verify the findings of scientific investigations related to CrossFit fitness domains as well as present outcome validity of CrossFit via systematic review and meta-analysis. Five of ten CrossFit fitness domains (cardiovascular/respiratory endurance, stamina, strength, flexibility, and power) were found in short-term intervention studies, with the remaining fitness domains (speed, coordination, agility, balance, and accuracy) lacking. Furthermore, CrossFit’s outcome evidence was provided for studies examining body composition, psycho-physiological parameters, musculoskeletal injury risk, life and health aspects, and psycho-social behavior. With respect to these studies, few achieved a high level of evidence at low risk of bias.
Meta-analyses were performed on body composition parameters including body mass index, relative body fat, fat mass, lean body mass, and waist circumference. All variables had non-significant results, reinforcing the need for more high-quality studies on CrossFit as well as long-term interventions.
Psycho-physiological Parameters
A study comparing CrossFit training with a training approach based on ACSM recommendations reported CrossFit training as more strenuous and considered a “very hard” activity by participants [52]. CrossFit participants also reported greater fatigue, greater muscle pain and swelling, and limb movement difficulties during or within 48 h after the workout [52]. Furthermore, the authors reported the five most frequently used and hardest WODs were “Fran,” “Murph,” “Fight Gone Bad,” “Helen,” and “Filthy Fifty.” Except for “Fran,” the psycho-physiological responses to these WODs were not reported. “Fran” and another popular WOD known as “Cindy” presented greater magnitudes for heart rate (95–97% of HRmax), %VO2max (57–66%), blood lactate (14–15 mmol/L), and rate of perceived exertion (RPE) [44]. Perciavalle et al. [59] also observed lactate concentrations around 14 mmol/L following a WOD called “15.5”. “Cindy” (98% HRmax and RPE = 9) also presented an acute blood oxidative stress response similar to a traditional bout of high-intensity treadmill running (running at a minimum intensity of 90% maximum heart rate over 20 min) [47].
Researchers have reported a decrease in anti-inflammatory cytokines without decrements in muscle power following two consecutive days of CrossFit training sessions [62]. The WODs employed included a rest interval between sets and exercises (i.e., 2–5 min, for more details see Table 1). Thus, IL-6 displayed an increase immediately after training WOD 1 and WOD 2 while IL-10 displayed an increase immediately after WOD 1 only and decreased 24 and 48 h following WOD 2 when compared to baseline values [62]. These findings should be considered with caution as while there are designated rest intervals in some CrossFit workouts (e.g., Fight Gone Bad, 5 × 500 m row), the inclusion of rest intervals is not common practice in CrossFit prescriptions.
In an acute study, the WOD “CrossFit triplet” (i.e., three burpees, four push-ups, and five squats; for details see Table 1) was associated with significant changes in physiological responses [51]. Participants achieved approximately 12,000 mmHg for rate pressure product, 6 mmol/L for blood lactate, and 54% of HRmax [51]. According to the authors, “CrossFit triplet” was of moderate to high intensity and thus considered a viable interval training option that provides sufficient intensity in a safe manner [51].
In the correlation studies, whole-body strength, power, endurance, and experience seemed to be important measures associated with performance in CrossFit [42, 43]. Butcher et al. [43] reported whole-body strength as a predictor of performance in some WODs such as “Grace,” “Fran,” and “Cindy”. The authors also found VO2max, Wingate power, and anaerobic thresholds were unsuccessful in predicting WOD performance. Conversely, Bellar et al. [42] found VO2max and anaerobic power to be significant predictors of performance after one CrossFit training session. The authors also divided 32 young healthy men into two groups and found CrossFit experience, or CrossFit training history, was also a predictor of performance during a WOD. Nonetheless, more research is required as the present literature is inconclusive regarding predictors of CrossFit performance.
Based on the systematic review, in general, WODs present highly varied psycho-physiological demands: heart rate between 54 and 98% of HRmax, blood lactate levels between 6 and 15 mmol/L, %VO2max between 57 and 66%, RPE between 8 and 9 (out of 10), and rate pressure product around 12,000 mmHg. Some WODs (e.g., “Fran,” “Cindy,” and “15.5”) can be identified as high-intensity level whereas others (e.g., “CrossFit triplet”) can be considered moderate.
Musculoskeletal Injury Risk
In one of the first publications on musculoskeletal injury risk, a descriptive epidemiological investigation used an electronic questionnaire to examine 132 CrossFit participants [34]. Results revealed 74% of CrossFit participants suffered at least one injury. The most common injury sites were shoulder and lower back followed by arm/elbow, with an injury rate of 3.1 events every 1000 h of training [34]. A total of 186 lesions were reported with some participants injured more than once in a period of 18 months. Nine of these cases required surgical intervention. In another study that examined the epidemiological profile of CrossFit participants, an injury prevalence of 31% was recorded [4]. In addition, when the participants were separated according to CrossFit experience, those who practiced CrossFit for more than 6 months (35%) showed significantly (p = 0.004) higher injury rates than those who practiced for less than 6 months (23%). This study also reported a 45% injury prevalence rate among athletes with more than 2 years of practice [4].
Another descriptive epidemiological study employed an electronic questionnaire to verify injury risk of the shoulder in CrossFit participants (n = 187). The authors found that 24% of participants reported at least one shoulder injury in the last 6 months of practice, with an injury rate of 1.9 per 1000 h. The most common attributed causes of injury were inadequate form of movement (33%) and exacerbation of previous injury (33%). Furthermore, 64% of those who suffered an injury reported a reduction in training for 1 month or less due to injury [61].
Similar electronic questionnaire and experimental approaches have also been used to examine injury risk in CrossFit (n = 381). Musculoskeletal injuries accounted for 19% of all injuries, with men injured more frequently than women (p = 0.03). The shoulder was injured most often during gymnastic movements whereas the lower back was injured most often during power lifting movements [41].
In addition, two case reports offered insight on injury risk. The first case study examined a traumatic tear of the latissimus dorsi myotendinous junction inflicted during the “muscle up” exercise [45]. This injury usually occurs in the acute configuration of forced abduction and external rotation during resisted contraction. Performing this exercise requires sound technique and high levels of strength, particularly at the transition point of the maneuver. The participant in this case report returned to complete pre-injury level of activity within 6 months after the inciting event, with mild residual functional deficit. The second case report was a retinal detachment due to CrossFit training [35]. A 25-year-old male presented an inferior scotoma in the right eye after engaging in a CrossFit workout which required “pull ups” with an elastic band tied around the waist and secured to the pull up bar, thus partially supporting body weight. The retina was successfully reattached, and vision was successfully recovered after 4 months.
The acute effects of high-intensity CrossFit training on tendon properties were evaluated via ultrasonography (n = 34). Thickness of the patellar and Achilles tendons increased significantly after the session. These findings suggest the high-intensity loads associated with concentric and eccentric muscle actions during CrossFit exercise may result in an increase in patellar and Achilles tendon thickness. However, long-term interventions are needed to investigate the effect of recovery between high-intensity sessions as a deterministic factor in altering the structure of biomaterials within tendons and the subsequent effects of changes in tendon morphology on risk of injury [5].
In summary, the number of injuries that affect CrossFit participants varies between 19 and 74% with 1.9–3.1 per 1000 training hours. In this sense, the percentage of injury is relatively high while the incidence of injuries per 1000 h is low. These results may reflect a sampling bias or inadequate management of training volume. Although higher training volume and perception of intensity have been found in CrossFit participants [49, 52], further studies directly comparing the injury rates of CrossFit with other ACSM-recommended training modalities are warranted.
The second aspect highlighted by the CHAMP and ACSM consensus was monitoring individual-specific training load and its potential to minimize injury risk [10]. Although the cause of injury is multifactorial, injury can result from the summation of load that imposes a force that exceeds the capacity of the biological tissue involved [65]. To attenuate this deleterious outcome, an integrated approach that incorporates individual-specific monitoring [12], quantification [13], and regulation [14] may aid in decreasing injury risk. Monitoring is defined as the verification of responses to the training loads performed that were previously planned by the coach [12]. Quantification is defined as the sum of the training load that was effectively executed by the athlete [13]. Regulation is defined as the adjustments in the training loads lifted in relation to the athlete responses [14]. However, no studies investigating training load management were found in the systematic review, which presents a gap in current knowledge. Presently, controlling training load is based on the coach’s anecdotal and scientific background which can be highly varied around the world. Due to the potentially positive impact an evidence-based integrated approach to training load management could have on reducing injury, risk while achieving training objectives (i.e., enhancing sports performance) [17,18,19,20,21,22] warrants greater research in this area.
Life and Health Aspects
Though sparse, case report and case series studies were found in the literature examining life and health aspects. Only two reported cases of rhabdomyolysis were found [39, 52]. However, this does not rule out the need to develop strategies of recovery between training sessions, respecting biological individuality of participants.
Other life and health aspects related to CrossFit training were found in the literature. Lu et al. [48] reported three cases of cervical carotid dissection that were associated with CrossFit workouts. Specifically, participant 1 suffered a distal cervical internal carotid artery dissection near the skull base and a small infarct in Wernicke’s area. The individual was placed on anticoagulation and on follow-up was near complete recovery. Participant 2 suffered a proximal cervical internal carotid artery dissection that led to arterial occlusion and recurrent middle cerebral artery territory infarcts, in addition to significant neurological sequelae. Participant 3 had a skull base internal carotid artery dissection that led to a partial Horner’s syndrome but no cerebral infarct. None of the three individuals died. While direct causality cannot be proven, the authors speculated the high-intensity CrossFit workouts likely led to the internal carotid artery dissections in these participants.
Similarly, Alexandrino et al. [37] examined 10 cases of stroke in participants aged between 27 and 65 years (80% being male). Among them, one man (32 years old) had an intracerebral hemorrhage stroke during a CrossFit session. The participant did not die, but he was left disabled ( no. 3 in the modified Rankin scale = moderate disability; requiring some help, but able to walk without assistance). The authors’ conclusion was that stroke during sport activity is rare, occurring mostly in healthy young males and that cervicocerebral arterial dissection is the primary mechanism of stroke, often without an explicit history of trauma.
Finally, researchers demonstrated neither beneficial nor deleterious effects on pelvic floor strength or support in nulliparous young women after CrossFit training [58]. The majority of these studies were evidence level 4 with high risk of bias and, as such, did not permit any recommendation.
To date, no studies have examined the effect of CrossFit training on resting blood pressure or heart rate. Further research examining the acute and chronic effects of CrossFit training on these health indicators is warranted.
Psycho-social Behavior
A greater sense of community in CrossFit sessions was verified when compared to traditional training whether in a group or analyzed on an individual basis. This social interaction level was assessed via questionnaire in physically active participants [60, 63]. However, sense of community was not related to participant retention/adherence for any of the modalities analyzed [63].
The retention/adherence of participants was assessed in a randomized intervention study involving obese individuals (BMI > 30). The same number of dropouts was also revealed after 8 weeks of traditional training when compared to CrossFit with aerobic and resistance training. Nonetheless, the intention for continuing physically vigorous activity was greater for the CrossFit group [38]. Furthermore, a European Organization for Research and Treatment of Cancer core 30-item questionnaire revealed 5 weeks of CrossFit training was well received by cancer survivors with an adherence rate of 75%. This intervention was also considered feasible and effective in improving emotional function [46].
Motivation for the practice of physical activity was also assessed by questionnaire in four groups: CrossFit, resistance exercise, alone, and in individuals who train with a personal trainer. Enjoyment, challenge, and affiliation were identified in the CrossFit group more than all other training groups. Such source of motivation is compatible with that presented in sports practice. Individuals who trained with a personal trainer had higher health-related motives. However, this group was older than the other groups, which may represent a confounding factor in the response [54].
In schoolchildren (i.e., 12 to 16 years) participating in CrossFit exercise, an older age has been associated with higher ratings of perceived intensity and less enjoyment. In the between-sex comparison, boys perceived greater intensity and enjoyment [49]. Among adults, no sex difference was identified for the perceived motivational climate of CrossFit sessions, although the achievement goals varied between males and females [40]. With respect to achievement goals, the mastery-based motivational climate is initially predominant, but when a domain of the tasks is reached, the performance approach becomes predominant. These variations are also present between sexes, with females emphasizing mastery avoidance (i.e., to do as well as I can) and males emphasizing the performance approach (i.e., to do better than others) [40].
Although the goals within CrossFit practice vary with practice time, the same does not appear to be true for psychological functioning as well-being, affection, body awareness, and self-esteem were not influenced by the time or frequency of CrossFit practice [56]. Similar results were found in an 8-week intervention study in adolescent students (i.e., 15 years), where no improvement in mental health was observed. However, a subgroup of individuals at risk of psychological distress presented significant improvements in mental health [53]. In another study of the same research group, high levels of retention (i.e., 82%), adherence (i.e., 94%), and satisfaction (4.2–4.6 where 5 is the highest level) were found in the students after 8 weeks of CrossFit Teens training [54].
Lastly, CrossFit’s motivational characteristics, which aim to lead the individual to achieve the best performance possible, generated a 5% prevalence of exercise addiction in CrossFit participants which is similar to other exercise programs. This observation has also been shown to be even greater in men and young individuals (i.e., < 30 years). Exercise addiction was associated with a tendency to exercise despite injury, feelings of guilt when unable to exercise, passion turning into obsession, and taking medication to be able to exercise. These negative attitudes toward exercise can facilitate damage, such as injuries and losses in social relations, within participants [57].
In summary, there is preliminary evidence of a higher sense of community, satisfaction, and motivation among CrossFit participants. However, it is still necessary for new studies to verify the positive relationship between these factors and retention/adherence of participants.
Brief Statement
Before finalizing, we wish to emphasize that this study did not seek to define CrossFit as “bad” or “good.” Rather, this investigation sought to present the possible benefits and risks associated with CrossFit according to current findings in the scientific literature. The low level of evidence at high risk of bias revealed by this study does not allow a stronger position on the advantages and disadvantages of CrossFit. The authors believe this disparity demonstrates the need to improve current methodological approaches in further studies, thus influencing current practice.
Conclusions
Until now, current CrossFit scientific literature has been based on studies that investigated the effects of CrossFit on body composition, psycho-physiological parameters, musculoskeletal injury risk, life and health aspects, and psycho-social behavior. Meta-analysis did not find a significant effect of CrossFit training changes in body mass index, relative body fat, fat mass, lean body mass, and waist circumference. Unfortunately, the number of studies investigating CrossFit with high level of evidence at low risk of bias is sparse. As a result, these findings neither firmly establish the benefits or risks of CrossFit, nor provide definitive practical recommendations concerning CrossFit training. Despite this disparity, there is the existence of initial evidence of higher levels of sense of community, satisfaction, and motivation among CrossFit participants.
References
Beers E. Virtuosity goes viral. CrossFit J. 2014;6:1–10.
Glassman G. What is fitness. CrossFit J. 2002;3:1–11.
Glassman G. Understanding CrossFit. CrossFit J. 2007;56:1–2.
Sprey JWC, Ferreira T, de Lima MV, Duarte A, Jorge PB, Santili C. An epidemiological profile of crossfit athletes in Brazil. Orthop J Sport Med. 2016;4:1–6.
Fisker FY, Kildegaard S, Thygesen M, Grosen K, Pfeiffer-Jensen M. Acute tendon changes in intense CrossFit workout: an observational cohort study. Scand J Med Sci Sports. 2016; https://doi.org/10.1111/sms.12781.
Thompson WR. Worldwide survey or ftiness trends for 2016: 10th Anniversary edition. ACSMs. Health Fit J 2015;19:9–18.
Thompson WR. World wide survey of fitness trends for 2017. ACSMs. Health Fit J 2016;20:8–17.
Thompson WR. Now trending: worldwide survey of fitness trends for 2014. ACSMs. Health Fit J 2013;17:10–20.
Thompson WR. World wide survey of fitness trends for 2015: what’s driving the market. ACSMs. Health Fit J. 2014;18:8–17.
Bergeron MF, Nindl BC, Deuster PA, Baumgartner N, Kane SF, Kraemer WJ, et al. Consortium for Health and Military Performance and American College of Sports Medicine consensus paper on extreme conditioning programs in military personnel. Curr Sports Med Rep. 2011;10:383–9.
Poston WSC, Haddock CK, Heinrich KM, Jahnke SA, Jitnarin N, Batchelor DB. Is high-intensity functional training (HIFT)/CrossFit safe for military fitness training? Mil Med. 2016;181:627–37.
Akenhead R, Nassis GP. Training load and player monitoring in high-level football: current practice and perceptions. Int J Sports Physiol Perform. 2016;11:587–93.
Borresen J, Lambert MI. The quantification of training load, effect on performance. Sports Med. 2009;39:779–95.
Siff MC. In: CO, editor. Supertraining. 6th ed. Denver: Supertraining Institute; 2003.
Halson SL. Monitoring training load to understand fatigue in athletes. Sports Med. 2014;44:139–47.
Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder? BrJ Sports Med. 2016;50:273–80.
Amadio AC, Serrão JC. A biomecânica em educação física e esporte. Rev Bras Educ Fis Esporte. 2011;25:15–24.
Elliott B. Biomechanics: an integral part of sport science and sport medicine. J Sci Med Sport. 1999;2:299–310.
Jones CM, Griffiths PC, Mellalieu SD. Training load and fatigue marker associations with injury and illness: a systematic review of longitudinal studies. Sports Med. 2017;47:943–74.
Hopkins WG. Quantification of training in competitive sports. Methods and applications. Sports Med. 1991;12:161–83.
Claudino JG, Cronin JB, Mezêncio B, Pinho JP, Pereira C, Mochizuki L, et al. Autoregulating jump performance to induce functional overreaching. J Strength Cond Res. 2016;8:2242–9.
Claudino JG, Mezêncio B, Soncin R, Ferreira JC, Couto BP, Szmuchrowski LA, et al. Pre vertical jump performance to regulate the training volume. Int J Sports Med. 2012;33:101–7.
Claudino JG, Cronin J, Mezêncio B, McMaster DT, McGuigan M, Tricoli V, et al. The countermovement jump to monitor neuromuscular status: a meta-analysis. J Sci Med Sport. 2017;20:397–402.
Gross A, Schirm S, Scholz M. Ycasd—a tool for capturing and scaling data from graphical representations. BMC Bioinformatics. 2014;15:219.
Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5:13.
Begg C, Cho M, Eastwood S, Horton R, Moher D, Olkin I, et al. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA. 1996;276:637–9.
Group OL of EW. The Oxford Levels of Evidence 2. In: Medicine OC for E-B. 2011.
Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of iInterventions. Version 5. The Cochrane Collaboration; 2011.
Pas HI, Winters M, Haisma HJ, Koenis MJ, Tol JL, Moen MH. Stem cell injections in knee osteoarthritis: a systematic review of the literature. Br J Sports Med. 2017;15:1125–33.
Winters M, Eskes M, Weir A, Moen MH, Backx FJG, Bakker EWP. Treatment of medial tibial stress syndrome: a systematic review. Sports Med. 2013;43:1315–33.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale: L. Erlbaum Associates; 1988.
Hak PT, Hodzovic E, Hickey B. The nature and prevalence of injury during CrossFit training. J Strength Cond Res. 2013; https://doi.org/10.1519/JSC.0000000000000318.
Joondeph SA, Joondeph BC. Retinal detachment due to CrossFit training injury. Case Rep Ophthalmol Med. 2013;2013:189837.
Smith MM, Sommer AJ, Starkoff BE, Devor ST. Crossfit-based high-intensity power training improves maximal aerobic fitness and body composition. J Strength Cond Res. 2013;27:3159–72.
Alexandrino GM, Damásio J, Canhão P, Geraldes R, Melo TP, Correia C, et al. Stroke in sports: a case series. J Neurol. 2014;261:1570–4.
Heinrich KM, Patel PM, O’Neal JL, Heinrich BS. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: an intervention study. BMC Public Health. 2014;14:789.
Larsen C, Jensen MP. Rhabdomyolysis in a well-trained woman after unusually intense exercise. Ugeskr Laeger. 2014;176:1–2.
Partridge JA, Knapp BA, Massengale BD. An investigation of motivational variables in CrossFit facilities. J Strength Cond Res. 2014;28:1714–21.
Weisenthal BM, Beck CA, Maloney MD, DeHaven KE, Giordano BD. Injury rate and patterns among CrossFit athletes. Orthop J Sport Med. 2014;2:2325967114531177.
Bellar D, Hatchett A, Judge LW, Breaux ME, Marcus L. The relationship of aerobic capacity, anaerobic peak power and experience to performance in CrossFit exercise. Biol Sport. 2015;32:315–20.
Butcher S, Neyedly T, Horvey K, Benko C. Do physiological measures predict selected CrossFit(®) benchmark performance? Open Access J Sport Med. 2015;6:241–7.
Fernández JF, Solana RS, Moya D, Marin JMS, Ramón MM. Acute physiological responses during Crossfit® workouts. Eur J Hum Mov. 2015;35:114–24.
Friedman MV, Stensby JD, Hillen TJ, Demertzis JL, Keener JD. Traumatic tear of the latissimus dorsi myotendinous junction: case report of a CrossFit-related injury. Sport Heal. 2015;7:548–52.
Heinrich KM, Becker C, Carlisle T, Gilmore K, Hauser J, Frye J, et al. High-intensity functional training improves functional movement and body composition among cancer survivors: a pilot study. Eur J Cancer Care. 2015;24:812–7.
Kliszczewicz B, John QC, Daniel BL, Gretchen OD, Michael ER, Kyle TJ. Acute exercise and oxidative stress: CrossFit™ vs. treadmill bout. J Hum Kinet. 2015;47:81–90.
Lu A, Shen P, Lee P, Dahlin B, Waldau B, Nidecker AE, et al. CrossFit-related cervical internal carotid artery dissection. Emerg Radiol. 2015;22:449–52.
Sánchez-Alcaraz Martínez BJ, Gómez-Mármol A. Percepción de esfuerzo, diversión y aprendizaje en alumnos de educación secundaria en las clases de Educación Física durante una unidad didáctica de CrossFit. Sport Rev Euroam Ciencias del Deport. 2015;4:63–8.
Murawska-Cialowicz E, Wojna J, Zuwala-Jagiello J. Crossfit training changes brain-derived neurotrophic factor and irisin levels at rest, after wingate and progressive tests, and improves aerobic capacity and body composition of young physically active men and women. J Physiol Pharmacol. 2015;66:811–21.
Shaw BS, Dullabh M, Forbes G, Brandkamp J-L, Shaw I. Analysis of physiological determinants during a single bout of Crossfit. Int J Perform Anal Sport. 2015;15:809–15.
Drum SN, Bellovary BN, Jensen RL, Moore MMT, Donath L. Perceived demands and post-exercise physical dysfunction in CrossFit® compared to an ACSM based training session. J Sports Med Phys Fitness. 2017;57:604–9.
Eather N, Morgan PJ, Lubans DR. Effects of exercise on mental health outcomes in adolescents: findings from the CrossFit™ teens randomized controlled trial. Psychol Sport Exerc. 2016;26:14–23.
Eather N, Morgan PJ, Lubans DR. Improving health-related fitness in adolescents: the CrossFit teens™ randomised controlled trial. J Sports Sci. 2016;34:209–23.
Fisher J, Sales A, Carlson L, Steele J. A comparison of the motivational factors between CrossFit participants and other resistance exercise modalities: a pilot study. J Sports Med Phys Fitness. 2016;9:1227–34.
Kötele F, Kollsete M, Kollsete H, Köteles F, Kollsete M, Kollsete H, et al. Psychological concomitants of CrossFit training: does more exercise really make your everyday psychological functioning better? Kinesiology. 2016;48:39–48.
Lichtenstein MB, Jensen TT. Exercise addiction in CrossFit: prevalence and psychometric properties of the Exercise Addiction Inventory. Addict Behav Reports. 2016;3:33–7.
Middlekauff ML, Egger MJ, Nygaard IE, Shaw JM. The impact of acute and chronic strenuous exercise on pelvic floor muscle strength and support in nulliparous healthy women. Am J Obstet Gynecol. 2016;215:316. e1-7
Perciavalle V, Marchetta NS, Giustiniani S, Borbone C, Perciavalle V, Petralia MC, et al. Attentive processes, blood lactate and CrossFit®. Phys Sportsmed. 2016;44:403–6.
Pickett AC, Goldsmith A, Damon Z, Walker M. The influence of sense of community on the perceived value of physical activity: a cross-context analysis. Leis Sci. 2016;38:199–214.
Summitt RJ, Cotton RA, Kays AC, Slaven EJ. Shoulder injuries in individuals who participate in CrossFit training. Sports Health. 2016;8:541–6.
Tibana RA, de Almeida LM, Frade de Sousa NM, Nascimento D Da C, Neto IV de S, de Almeida JA, et al. Two consecutive days of CrossFit training affects pro and anti-inflammatory cytokines and osteoprotegerin without impairments in muscle power. Front Physiol. 2016;7:260.
Whiteman-Sandland J, Hawkins J, Clayton D. The role of social capital and community belongingness for exercise adherence: an exploratory study of the CrossFit gym model. J Health Psychol. 2016;1:1359105316664132.
Smith MM. CrossFit-based high intensity power training improves maximal aerobic fitness and body composition: retraction. J Strength Cond Res. 2017;31:e76.
Zernicke RF, Whiting WC. Mechanisms of musculoskeletal injury. In: Zatsiorsky VM, editor. Biomechanics in Sport. Oxford: Blackwell Science Ltd; 2000:507–22.
Acknowledgements
We would like to thank the authors of the cited articles who collaborated to obtain the data and “Coordenação de Aperfeiçoamento de Pessoal de Nível Superior/ Programa de Excelência Acadêmica” (CAPES/PROEX), “Conselho Nacional de Desenvolvimento Científico e Tecnológico” (CNPq), “Fundação de Amparo à Pesquisa do Estado de Minas Gerais” (FAPEMIG), and “Fundação de Amparo à Pesquisa do Estado de São Paulo” (FAPESP).
Funding
No sources of funding were used to assist in the design, collection, analysis, and interpretation of data or in writing of this manuscript.
Availability of data and materials
After publication, all data necessary to understand and assess the conclusions of the manuscript are available to any reader of Sports Medicine-Open.
Author information
Authors and Affiliations
Contributions
JGC contributed in the design, collection, analysis, and interpretation of data and in writing. TJG contributed in the interpretation of data and in writing. FB and HSS helped in the design, collection, analysis, and interpretation of data and in writing. RM, BM, RS, CACF, AJH, and MB contributed in the design and interpretation of data and in writing.. ACA and JCS helped in the design, analysis, and interpretation of data and in writing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Not applicable.
Competing interests
All authors – João Gustavo Claudino, Tim J. Gabbett, Frank Bourgeois, Helton de Sá Souza, Rafael Chagas Miranda, Bruno Mezêncio, Rafael Soncin, Carlos Alberto Cardoso Filho, Martim Bottaro, Arnaldo Jose Hernandez, Alberto Carlos Amadio and Julio Cerca Serrão – declare that they have no conflicting interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Table S1. The Consolidated Standards of Reporting Trials (CONSORT). (DOCX 43 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Claudino, J.G., Gabbett, T.J., Bourgeois, F. et al. CrossFit Overview: Systematic Review and Meta-analysis. Sports Med - Open 4, 11 (2018). https://doi.org/10.1186/s40798-018-0124-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-018-0124-5