
Abstract
Background
Understanding of an athlete’s lifespan is limited with a much more sophisticated knowledge of their competitive careers and little knowledge of post-career outcomes. In this review, we consider the relationship between participation at elite levels of sport and mortality risk relative to other athletes and age- and sex-matched controls from the general population. Our objective was to identify, collate, and disseminate a comprehensive list of risk factors associated with longevity and trends and causes of mortality among elite athletes.
Methods
English language articles were searched using the Web of Science database. Keywords athletes, death, elite, “high performance” life expect*, longevity, mortality, players, professional, and sport were used to locate research articles. Seventeen additional articles were retrieved from reference lists found in these papers and a general web search. The inclusion criteria were the following: (1) publication year 1980 or later; (2) the study examined elite-level athletes; and (3) outcome data measured mortality/longevity trends and/or causes.
Results
Fifty-four peer-reviewed publications and three articles from online sources met the criteria for inclusion. Baseball, football, soccer, basketball, and cycling had the most reported data on elite athletes’ lifespan longevities. A variety of mechanisms have attempted to explain mortality risk (e.g., handedness, playing position, achievement, etc.). Considerable support was found for superior longevity outcomes for elite athletes, particularly those in endurance and mixed sports.
Conclusions
Future research into the mechanisms that may affect mortality risk is important for a better understanding of life expectancies in both eminent and non-eminent populations. Participation in elite sport is generally favorable to lifespan longevity.
Key Points
-
A majority of studies included in this review reported superior lifespan longevity outcomes for elite athletes compared to age- and sex-matched controls from the general population and other athletes.
-
Several mechanisms within and between sports may have powerful effects on the overall lifespan longevities of players (e.g., type of sport, playing position, race, and energy system).
-
Future research on mortality in elite athletes would benefit from more comprehensive statistical measures and reliable databases to determine potential mechanisms that may influence mortality trends and causes in both athlete and non-athlete samples.
Similar content being viewed by others
Background
Rationale
Researchers have given considerable attention to the athlete development process (e.g., positive youth development through sport) (see [1]). Interestingly, insight into post-career outcomes is significantly limited. For instance, our knowledge of how participation in elite sport affects lifespan longevity is particularly incomplete. This lack of information about later phases of athletes’ lifespans may be attributable to several factors, such as the greater access to athletes during their competitive careers as well as the preponderance of participation- and performance-based theories focusing on elements related to understanding the antecedents of sporting success (e.g., [2]). Attaining a complete understanding of an athlete’s lifespan requires knowledge of the inherent complexity of relationships that link hereditary and environmental characteristics to developmental outcomes. In this study, we focus on mortality of previously elite athletes.
An important challenge to mortality research in sport is the lack of data on the health behaviors of athletes post retirement. Much of our current understanding of trends and causes in elite athlete mortality derives from what appear to be “one-off” studies by small teams of researchers. Past work examining this issue in depth appears to be limited, although the Finnish studies that examined lifespan longevities of former elite endurance, team, and power athletes who represented Finland between the years 1920 and 1965 are exceptions (e.g., [3–6]). In addition, views on elite athlete mortality are largely shaped by popular media sources, which may downplay tenets of the lifespan and create false perceptions of early mortality in athletes (e.g., MLB’s Tony Gwynn at 54 years [cancer], the NFL’s Junior Seau at 43 years [suicide], boxing’s Tommy Morrison at 44 years [AIDS], sailing’s Andrew Simpson at 36 years [drowning] and skiing’s Sarah Burke at 29 years [training fall]).
A recent meta-analysis completed by Garatachea et al. [7] indicated that elite athletes live longer than the general population, with an all-cause pooled standard mortality ratio (SMR) of 0.67 (95 % confidence interval [CI] 0.55–0.81; P < 0.001). Further, they found a lower risk of cardiovascular disease (CVD) and cancer in those who participated in high-performance sport, which emphasized the health benefits of exercise [7]. While their study makes an important contribution to our knowledge of longevity outcomes in elite sport, the restrictive sampling frame necessary for a meta-analysis excluded numerous studies that could inform our broader understanding of elite athlete health. For example, Garatachea et al. [7] included 10 studies of elite athlete longevity in their meta-analyses, but their inclusion criteria excluded studies that did not use SMR as a statistical measure of mortality (38 studies were excluded for this reason). As a result, studies with important information regarding longevity in elite athletes were excluded, such as greater longevity in Norwegian professional divers (hazard ratio [HR] = 0.79, 95 % CI 0.63–0.997) [8], and important mechanisms that may influence longevity, such as sex, as indicated by Olympic medal-winning females having greater longevity relative to Olympic medal-winning male athletes (HR = 0.61, 95 % CI 0.51–0.72) [9], and race, as indicated by African-American professional basketball players having a 77 % greater risk of death compared with white players (HR = 1.77, 95 % CI 1.35–2.32) [10]. Further, several studies which reported SMRs were not included in the meta-analysis (e.g., [11–15]). As such, there is an opportunity to grow our current limited understanding of longevity outcomes of elite athletes by examining a wider range of studies and sports through a systematic review.
Similarly, Teramoto and Bungum [16] completed a narrative review of mortality and longevity of elite athletes; however, a relatively small sample of 14 epidemiological studies was included. Their primary method of literature retrieval was through the PubMed (1950-) and Scopus (1960-) databases, using keywords mortality, longevity, life expectancy, death, and (elite/professional) athletes and players. While this literature search strategy was appropriate, a large number of studies on elite athlete mortality and longevity were published during or after their publication year of 2010 (e.g., [3, 8–10, 12, 13, 15, 17–31]). As a result, mechanisms such as race have since been validated as more consistent indicators of early mortality (e.g., [10, 19]). Currently, it may be premature to make conclusions about the long-term value of being a professional athlete considering the new evidence that has emerged from literature.
Although it appears that there are many unanswered questions concerning athletes’ lifespan longevities, Teramoto and Bungum [16] presented enough empirical evidence to determine some cross-sport and energy system trends. Teramoto and Bungum [16] found a trend towards endurance (e.g., long-distance runners) and mixed-sport (e.g., soccer) athletes having more favorable survival outcomes relative to power sport (e.g., weightlifters) athletes and the general population. Similarly, a meta-analysis performed by Löllgen et al. [32] examined 38 studies that measured physical activity and all-cause mortality in samples of physically active individuals (non-elite athletes) and reported an overall significant relationship between physical activity participation and lower all-cause mortality. Light and moderate intensity levels of activity were generally associated with a reduction in mortality, whereas training at high intensities was not required for the main prevention against all-cause mortality [32]. While Löllgen and colleagues [32] provided evidence of physical activity positively influencing lifespan longevity independent of age and sex, the relationship between participation in elite sport and longevity can enhance our understanding of the benefits of physical activity at the highest levels of competition in unique athletic cohorts.
Teramoto and Bungum’s [16] review suggested that the type and dose of elite sport participation may ultimately determine mortality risk. In addition, Teramoto and Bungum [16] highlighted the importance of considering elite athletes as a heterogeneous group with respect to mortality trends; differences between and within sports exist. In particular, the differences in health-related behaviors between and within sports may also create modifiable factors that are associated with longevity and mortality. As a result, overall mortality risk is explained by several modifiable factors, such as obesity and physical inactivity, and non-modifiable (unchangeable) factors, such as age and race, that are unique to athletes. For instance, Baron et al. [19] found an overall decrease in mortality in National Football Players (NFL) who were active between 1959 and 1988; however, defensive linemen had increased mortality from CVD and cardiomyopathy. Moreover, those with a playing time body mass index (BMI) of >30 kg/m2 had a significantly higher risk of CVD, which was also influenced by race/ethnicity [19]. Although the effects of playing position on lifespan longevity may be more pronounced in contact sports such as football, we cannot overlook the differences and nuances in health-related behaviors between and within sports that may influence lifespan longevities.
Objectives
A subject such as death rates in professional athletes may be more susceptible to sensationalism when trends begin to emerge; therefore, it is essential that the data being disseminated are transparent and accurate. In this review, we consider the relationship between participation at elite levels of sport and mortality risk relative to other athletes and age- and sex-matched controls from the general population. Our objective was to extend the narrative review of Teramoto and Bungum [16] with a more comprehensive and up-to-date list of studies on mortality and longevity in previously elite athletes. More specifically, our aim was to advance knowledge in this area by collating athlete mortality/longevity literature that may help refine future analytic methods, form evidence-based models of athlete longevity, and determine whether elite-level participation in high-performance sport produces a lifespan longevity advantage. Similar to Teramoto and Bungum’s [16] research questions, we asked the following: (1) do elite athletes have superior longevity outcomes relative to the general population, and (2) which mechanisms and risk factors are associated with longevity and are potential precursors to early mortality?
Methods
Literature Search
A systematic review of literature was performed using the Web of Science database (1 January 1980–30 September 2014; see Tables 1 and 2). Web of Science was chosen as our primary citation index as it contained over 90 million records through its 7 online databases, which would have made searches into smaller citation indexes largely redundant (e.g., EMBASE contains over 28 million records). Further, given this review’s objective, Web of Science’s databases appeared to be the most relevant to our study (e.g., Science Citation Index Expanded). Keywords, including athletes, death, elite, “high performance” life expect*, longevity, mortality, players, professional, and sport, were used to locate research articles. While a full electronic search strategy for at least one database is recommended [33], we further located research articles by searching the references of records that were identified through our database search, in addition to performing a general web search through the Google Scholar search engine.
Inclusion Criteria
The inclusion criteria were the following: (1) publication year 1980 or later; (2) the study examined elite-level athletes; and (3) outcome data measured mortality/longevity trends and/or causes. We excluded studies with no full-text availability (abstracts, conference proceedings, commentaries, and editorials), no English-text availability (a small proportion of international articles were unavailable for translation to English), other literature reviews with different inclusion criteria (e.g., non-elite samples), duplicates, case reports, studies on morbidity (i.e., CVD risk factors, etc.), psychosocial measures, collegiate athletes, and studies on the effectiveness of pre-screening strategies and prevention. For consistency, we use “elite” synonymously with any form of high-performance participation in sport (i.e., national, professional, and international competition such as the Olympics).
Data Extraction
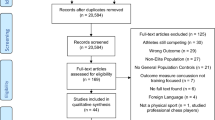
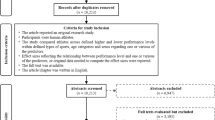
We identified 1001 records through database searching using the aforementioned keywords. After review of title and abstract, we excluded 961 of those records (identical papers, n = 31; inclusion criteria not fulfilled, n = 930; most commonly due to studies not examining elite athletes and/or mortality/longevity trends), which left 40 eligible full-text articles from the Web of Science database search. Seventeen additional articles were retrieved from reference lists found in these papers and a general web search. In total, 57 studies filled the criteria for inclusion (Tables 1 and 2): 54 peer-reviewed publications (see Table 1), in addition to three articles from online sources included to investigate findings of mortality risk in elite athletes that may be disseminated to a different cohort of the population (e.g., social media users; see Table 2). Specifically, these three additional articles were located through Google Scholar’s search engine using the same keywords as used in the Web of Science database search (e.g., athletes, death, etc.). We assessed the quality of each of these records through the Newcastle-Ottawa Quality Assessment Scale for cohort studies [34]. See Fig. 1 for the PRISMA statement [33].

Flow of information through the different phases of the systematic review, as per the PRISMA statement [33]. *Additional records were identified through searching the references of records that were identified through database searching and a general web search (i.e., Google Scholar)
Measured Outcomes
This review was comprised of elite athlete mortality/longevity studies from 13 different countries: USA, France, Italy, Belgium, Norway, Sweden, Finland, New Zealand, Netherlands, Germany, Japan, Poland, and the UK. Measures of mortality included hazard rate/ratio of death (HR), life expectancy (LE), mortality rate (MR), odds ratio for mortality (OR), relative conditional survival (RCS), relative survival ratio (RSR), standardized mortality ratio (SMR), and standardized proportionate mortality ratio (SPMR). All LE and MR data were compared to age-matched controls from the general population and all studies were on male participants, unless stated otherwise in the tables.
Results
Literature Search
From 1 January 1980 to 30 September 2014, we located 54 peer-reviewed studies [3–6, 8–15, 17–31, 35–61] and three online articles [62–64] that examined mortality and longevity in elite athletes (n = 57). This is an addition of 43 peer-reviewed studies that were not included in Teramoto and Bungum’s [16] review (11 peer-reviewed studies overlap). Three peer-reviewed studies from their review did not match our inclusion criteria (<1980).
Summary of Life Expectancy in Elite Athletes from Literature
This review included a total of 465,575 athletes: 450,295 from peer-reviewed literature (Table 1) and 15,280 from online articles (Table 2). Of those 465,575 examined, only 5610 (1.2 %) were female athletes. Although it appears that females have been grossly underrepresented in mortality and longevity studies of elite athletes, the extremely low proportion of 1.2 % is skewed by separate studies examining the same cohort of players [e.g., 12 and 19, n = 3439; 3–6, active Finnish athletes from 1920 to 1965), single studies that contained very large sample sizes of male athletes [e.g., 11; n = 300,818), and instances where the breakdown of sex in the sample went unreported (e.g., [31]). Nevertheless, only 6 peer-reviewed studies on elite athlete mortality and longevity that included females in their samples were identified [9, 20, 24, 31, 58, 60] and no studies that investigated females exclusively.
From the 9-point Newcastle-Ottawa Quality Assessment Scale [34], 1 study had a quality score of 6, 6 studies had a quality score of 7, 32 studies had a quality score of 8, and 15 studies had a quality score of 9 (only peer-reviewed articles were assessed). Therefore, the majority of the studies included in this review were generally of high quality (e.g., representative sample sizes, age- and sex-matched control groups from the general population, etc.).
Of the 54 peer-reviewed studies included, 4 were responses to the authors of different studies related to mortality and longevity of elite athletes [29, 30, 42, 44]. Aside from the studies or reviews that examined multiple sports, professional baseball players (n = 16), football players (4 peer-reviewed, 2 online), soccer players (n = 4), basketball players (n = 3), and cyclists (n = 3) were identified through our literature search as having the most reported data on elite athletes’ mortality outcomes. In particular, MLB players [15, 36, 38, 45–47], NFL players [12, 19, 49, 62], cyclists [13, 27, 28], NBA players [10, 48], and golfers [11, 21] had the most robust evidence of greater longevity. These LE benefits generally ranged from 4 to 8 years [e.g., 36 and 28, respectively].
The majority of studies included in this review examined sport organizations that were primarily located in the USA and used age- and sex-matched controls that were also American (MLB, NBA, and NFL). The general finding of these studies was a greater longevity for elite athletes relative to their American controls. Notably, the majority of mixed-sport studies included in this review also found support for greater longevity for athletes who competed at elite levels of competition (e.g., Olympics). Similarly, the “one-off” studies from international researchers whose controls spanned 12 different countries also reflect a general trend towards increased survival rates for a diverse group of athletes relative to their country-specific controls from the general population. For example, elite cyclists, such as French, Italian, and Belgian Tour de France participants, had greater lifespan longevities when compared to the pooled general population from their respective countries for the appropriate age cohorts [13, 27, 28]. Further, Norwegian divers [8] and skiers [22] and Italian track and field athletes [58] had greater lifespan longevities relative to controls from their respective countries as well. Alternatively, less consistent results were found in soccer players, in which both superior survival rates in Dutch players [23] and inferior survival rates in German players [24] were reported, alongside increases in amyotrophic lateral sclerosis (ALS) prevalence in Italian players [55, 56]. In addition, elite Finnish powerlifters [53] displayed lower lifespan longevities compared to the Finnish general population.
Mechanisms of Mortality and Primary Outcomes
Considerable research attention has been given to identifying which mechanisms may be precursors to early mortality, including handedness, precocity, names and initials of players/athletes, playing position and weight, education and race, achievement, and energy system classifications. First, the relationship between handedness and mortality in elite athletes has received increased attention within the last two decades. Nevertheless, differences in longevity related to handedness appear to be non-existent in MLB [35, 42, 44] and NBA players [25]. While a relationship between longevity and handedness was identified in elite cricketers [51], the inclusion of a larger sample size appears to have washed out previous significant findings [52]. Second, the precocity-longevity hypothesis (see [65]), which investigates the relationship between precociousness (i.e., career debut) and early death, has been shown to affect MLB players’ longevities [39]. Third, MLB players with positive initials in their names (e.g., A.C.E.) were found to live significantly longer than players with negative initials (e.g., D.E.D.) [40] while baseball, hockey, football and basketball players with names beginning with D had shorter lifespans than those with names beginning with E to Z [17]. It is noteworthy that there has been some criticism regarding the methodologies used in these studies, such as using selective data and the appropriateness of the statistical tests performed [29, 30]. Further, while it has been suggested that health is influenced by certain symbolic aspects of the environment [66], such as a decreased prevalence of death before birthdays (e.g., [67]), the scientific rationale behind the initials of a name affecting lifespan longevity is limited. In turn, the emergence of a hypothetical name-longevity relationship in elite athletes emphasizes the need for greater replication in this area of research.
An athlete’s playing position is arguably the most obvious mechanism that influences mortality risk, largely due to perceived anthropometric differences that are determinants of health (e.g., weight). Longevity was found to be correlated with position in MLB [47] and NBA players [48]. In particular, weight and position significantly influenced mortality risk in NFL players [19, 49, 50, 61–63, 68]. Further, weight also influenced the lifespan longevities of baseball players [61, 69] and played a role in the longevities of Japanese sumo wrestlers, although its influence appeared to be small [OR = 1.08, CI 1.01–1.15; 57]. With regard to athlete race, this has been shown to be associated with longevity in NBA [10] and NFL players [19], as well as with education and longevity in MLB players [45]. Sixth, high achievement in sport emerged as a determinant of mortality, specifically through winning percentage in Japanese sumo wrestlers [57], handicap in Swedish golfers [11], and Hall of Fame (HOF) induction in a diverse range of sports [37, 59]. Although Abel and Kruger [37] reported differences in the life expectancies of MLB HOFs compared to non-inductees, Smith [30] did not find a statistically significant difference using corrected data from the same sample.
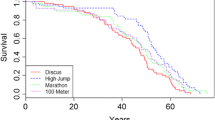
The last trend that developed from these studies, which served as a classification method for Teramoto and Bungum’s [16] review, was the relationship between the type of sport and required energy systems for participation (i.e., aerobic/endurance, mixed, and anaerobic/power) and mortality. Similar to Teramoto and Bungum’s [16] findings, the largest gains in lifespan longevities were in endurance and mixed-sport athletes. The greatest LE advantages were found in European cyclists [13, 27, 28], whereas the lowest LEs were found in Finnish powerlifters [53]. Cross-sport analyses uniformly reported LE advantages in endurance and mixed-sport athletes compared to power sport athletes [3–6, 20, 31], who had some evidence of increased premature mortality from suicide suspected from prior anabolic steroid use [26, 53]. The inconsistent mortality outcomes in power sport athletes make it difficult to generalize across all sports. Nevertheless, there was considerable support in the existing literature for superior longevity outcomes for elite athletes compared to the age- and sex-matched controls from the general population.
Discussion
The objective of our review was to advance knowledge on elite athlete mortality and longevity to ultimately determine whether elite-level participation in high-performance sport produces a lifespan longevity advantage. As a whole, the empirical evidence suggests that several mechanisms within and between sports have powerful effects on the overall lifespan longevities of players. Our first research question considered whether elite athletes had superior longevity outcomes relative to the general population. An overwhelming majority of studies included in this review reported favorable lifespan longevities for athletes compared to their age- and sex-matched controls from the general population. In fact, only two studies reported lower lifespan longevities in athletes relative to the controls: 812 male and female soccer players who participated in international matches for Germany between 1908 and 2006 (RSR ≤ 1) [24], and 62 male Finnish powerlifters who placed first–fifth in their respective weight category in the Finnish championships between 1977 and 1982 (SMR = 4.6) [53]. Our second research question explored the mechanisms and risk factors associated with longevity and whether there were precursors to early mortality. Although our overall understanding of modifiable and non-modifiable factors that contribute to mortality risk in elite athletes remains limited, in part due to methodological and data source inconsistencies [29, 30], some trends emerged from our investigation. In particular, our review supports previous conclusions that aerobic and mixed-sport athletes have superior longevity outcomes relative to more anaerobic sport athletes. In addition, playing position and weight, as well as education and race, appeared to be consistent indicators of mortality risk, whereas other mechanisms such as handedness, precocity, and names and initials appeared to be less consistent and/or examined.
In their review of the relationship between body size and lifespan longevity, Samaras et al. [61] drew attention to several confounders that may positively influence longevity outcomes, such as higher socioeconomic status, smaller body size, and positive environmental and health benefits. As highlighted in this review, weight is an important predictor of mortality risk. Likewise, significant empirical evidence suggests that obesity is one of the major risk factors for premature death (e.g., [70]). While it is premature to undervalue the relationship between weight and mortality in athletes, particularly post-retirement, research has also highlighted the importance of accounting for body composition. For example, it has been suggested that a measure of BMI is likely to overestimate adiposity in muscular athletes (e.g., [71]), particularly in NFL players [19]. In addition, Koning and Amelink [23] highlighted that self-selecting to participate in an occupation where health is important may predispose athletes to favorable survival outcomes relative to population comparisons. Factors such as these, in addition to a bevy of other confounders such as access to high-quality medical care [23], are what make LE a difficult outcome to accurately predict.
As a variety of confounders may impact longevity, the reasons for the differences in lifespans between elite athletes and the general population are likely to be multifactorial. Teramoto and Bungum [16] provided possible explanations of increased survival in the elite athlete cohort; namely, participation in higher volumes of exercise training leading to higher physical fitness levels, the likelihood that elite athletes are comprised of the healthiest and fittest individuals, and the maintenance of active and healthy lifestyles later in life. The extents to which these confounders contribute to mortality risk are still largely unknown however, as survival statistics may undermine the interplay of complex socioeconomic factors [72]. For example, medical care accessibility made available by higher income may improve the LE of athletes when compared to other groups. Further, plenty of corroborating evidence suggests health-care services alone do not result in improved health outcomes, but a variety of social factors such as education and employment produce these widespread biases in health (e.g., [73]). As a result, the historical investigations of elite athletes and longevity outcomes need to be cautiously interpreted and discussed in the contexts of a variety of possible influential factors of mortality.
Abel and Kruger [17] discussed two advantages to studying elite athletes with regards to longevity. First, they represent a relatively homogenous occupational population, similar to Teramoto and Bungum’s [16] classification of a distinct physically fit and healthy group, and, perhaps more importantly, many sports contain detailed statistical and historical databases that track a variety of variables that can influence longevity (e.g., anthropometrics, performance-based indicators such as induction into the HOF, etc.). These advantages help contribute to the growing body of research on elite athlete mortality trends, which in turn can advance research by forming evidence-based models of athlete longevity through investigations into a variety of variables. In contrast, a caveat to this tendency of measuring the effects of sport-specific variables on mortality is that the amount of data available varies from sport to sport and may be somewhat arbitrary. For example, handedness is unlikely to be measured in soccer players, and the influence of position in non-contact sports may be more relevant in life quality research rather than life longevity. In addition, each sport will have a different inaugural season, which limits the amount of deceased players in the relatively newer sports (e.g., mixed martial arts). Therefore, each sport will have unique statistical variables that may make it more difficult for researchers to draw cross-sport comparisons.
Limitations
The main finding of this systematic review indicates favorable lifespan longevity advantages for elite athletes relative to age- and sex-matched controls from the general population; however, limitations in reviewing literature on mortality and longevity in elite athletes exist. We will first examine the possible biases in epidemiological research in historical samples of athletes.
Databases
The use of accurate and up-to-date databases is extremely important when analyzing a sample longitudinally; however, some statistical databases for past players have been found to be incomplete. For example, Smith [30] discovered a substantial portion of missing death date data (e.g., unknown death dates) in former MLB players in the Sean Lahman Baseball Archive [74]. Unfortunately, Smith’s [30] critique of Abel and Kruger’s [37] conclusion (cases without death date data were treated as living players) that HOF non-inductees had a 5-year lifespan longevity advantage was not the only study on MLB player longevity that used the same database (e.g., [17, 35, 36, 38–40, 45]). Although it may be premature to conclude that other databases have similar fallibility (e.g., missing death date data), we must be cautious of the possible incongruency between reported and unreported/unknown death date data in other studies that bias lifespan longevity results.
Holistic Health
As a variety of socioeconomic, demographic, and epidemiologic factors dynamically interact to shape population change [72], so do factors that influence holistic health. Arguably, the most objective measurement of elite athlete health is rate of mortality. Using mortality statistics of elite athletes who played in the earlier decades to make inferences regarding holistic health in present-day athletes may be deceptive. The information age has made information on elite athletes easy to access, whereas information on elite athletes from the earlier eras often fails to depict the mental and social wellbeing characteristics that encompass holistic health. Sorenson et al.’s [75] investigation of lifespan exercise among elite intercollegiate athletes is one of few studies that have presented empirical evidence of lifetime health and wellbeing in modern competitive athletes relative to age- and sex-matched controls. They found that current student athletes reported higher volumes of weekly exercise, perceived exercise importance, and likelihood of compliance with American College of Sports Medicine (ACSM) exercise guidelines relative to non-athletes [75]. Interestingly, Sorenson et al. [75] found no significant differences between alumni student athletes and non-athletes, suggesting that former athletes failed to maintain higher exercise levels later in life. Further, in their follow-up study on the same sample, Sorenson et al. [76] found that relatively older former student athletes (age 43+ years) had a greater risk for joint health concerns later in life compared to a non-athlete control group. These findings seem counterintuitive since physical activity is often associated with a substantial reduction of chronic disease risk and being important to overall health and wellbeing (e.g., [77]).
To broaden our knowledge on holistic health outcomes and behavior in former athletes, it is important to consider the totality of data that have been collected and analyzed to date, particularly as research pertaining to the “whole person” (e.g., physical and psychosocial measures) in modern competitive athletes gains momentum. It is equally important to make the distinction between “quality of life” and “longevity,” as physical health likely moderates psychosocial health. For example, evidence suggests that physical activity plays an important role in managing mental health diseases, such as anxiety and depression (e.g., [78]). Thus, factors such as being physically capable to participate in physical activity are important to consider when determining an individual’s quality of life. As such, our current understanding of elite athletes’ quality of life during and after sport is limited relative to their lifespan longevity trends.
Statistical Measures
Another criticism of the athlete-mortality literature is on methodological grounds; more specifically, cross-study discrepancies in the statistical tests and/or measures used. Although the relative paucity of lifespan longevity studies of elite athletes may serve as a temporary explanation for why different measures and control variables are used to analyze mortality, we cannot ignore the impact of possible statistical bias risk. Risk of bias can affect the cumulative evidence of a review of literature [33], such as selective reporting within studies, whereby researchers may under-report variables that were found to have less statistical impact on longevity outcomes in the course of reporting results that support the direction of their findings. As a result, the extent of our knowledge about the influence of certain variables on longevity may be restricted. Future work in this area of research would benefit from replication of control variables when analyzing the same or similar athletic populations to better establish important predictors of longevity. Further, meta-analyses on the longevity of elite athletes, such as the review completed by Garatachea and colleagues [7], can provide more evidence-based data on the benefits of participating in physical activity. Moreover, it is notable that the sports examined have examined periods of different length. Ideally, comparisons would be best when comparing timespans of similar length; however, the timespans investigated have ranged from players being born from as early as 1840 [52] to being active as recently as 2012 [27]. These differences could affect the proportion of those living or dead in a sample, which may affect measures such as SMR. The implication of these biases on the cumulative evidence of this review is unclear, and as a result, it is important to consider how publication bias can under- and overestimate certain predictors of longevity.
Longitudinal Lifestyle Factors
Given that empirical evidence is necessary for coherent explanations of longevity outcomes of elite athletes, do mechanisms that influence mortality become ineffective and/or less powerful if maintenance of physical activity ceases? Although there has been some evidence that former intercollegiate student athletes fail to maintain higher exercise levels later in life [75], our understanding of the impact of different longitudinal lifestyle factors influencing lifespan longevity remains incomplete. For example, former male Finnish world class athletes were found to be more active than their non-competitive controls [79], and participation in physical activity at a young age predicted later life involvement, which reduced the prevalence of coronary heart disease [80]. In addition, former athletes have been found to partake in fewer negative health habits, such as smoking and drinking alcohol [79].
Another issue that is emerging from more recent research relates to the possible detrimental effects of high levels of training. In particular, O’Keefe (e.g., [81, 82]) has advocated that “excessive” aerobic training can result in cardiovascular damage (e.g., atrial fibrillation, coronary artery disease, and malignant ventricular arrhythmias). These effects may have particular relevance for studies of mortality in previously elite athletes. It is important for future research to determine which factors are more robust predictors of longevity and if they continue to be relevant in later life. In turn, these findings will have implications on the generalizability of factors found to predict mortality and longevity in elite athletes that were measured at one point in time (i.e., active athletic career).
Future Directions
The relationship between sport and health has evolved considerably over the past 100 years. The context in which the historical data are transferable is important to consider, particularly when discussing the social determinants of health [73]. Despite its limitations, historical analyses of sport and health shape our present understanding of its relationship and influence.
Reliable Databases, Repetition, Causes of Mortality, and Follow-up Studies
Continued contributions to the growing body of research on longevity outcomes of elite athletes should utilize appropriate statistical testing with reliable and complete databases. Although there are a variety ways to statistically measure and report mortality, research must be substantiated through repetition. An important first step is locating or comprising a reliable and comprehensive database that embodies all accessible and applicable data. To this end, future research of athlete lifespan outcomes can arguably have the greatest impact by determining the causes of mortality. Current empirical evidence on the rates of mortality in athletes is far superior to our knowledge on the causes of mortality. Epidemiological studies with long-term follow-ups are also rare [55]. For example, available evidence suggests a possible connection between dietary supplements and/or drug use and the high prevalence of amyotrophic lateral sclerosis (ALS) in former soccer players [55, 56]. This potential association emphasizes negative long-term neurological outcomes of performance demands that are not reflected in MR occurrence.
Cross-sport Comparisons and Generalizability
Several sports were noticeably absent from the elite athlete mortality literature (e.g., ice hockey, field hockey, handball, snowboarding, table tennis, volleyball, and motorsports). In addition, sex-related differences in lifespan longevity remain largely unknown due to the paucity of studies on elite female athletes. This raises an important concern about the cross-sport generalizability disseminated in this review. Perhaps more importantly, the applicability of these results to the general population (i.e., non-elite-athletes) can likely be best explained by mechanisms of mortality that have not been extensively examined to date in the athlete cohort. Some examples include smoking and diet/nutrition (as stated by Teramoto and Bungum) [16], lifespan health (psychosocial and physical, such as the influence of morbidity on life quality, etc.), and the interplay of nature (hereditary, such as superior genotypes for physical fitness) (e.g., [83]) and nurture (environmental influences). Presumably, elite athletes possess advantageous genetic traits. Research on the heritability of physical fitness (e.g., [84]) suggests that we cannot discount the influence of advantageous genetic inheritance coupled with high levels of participation and competition in sport.
Conclusions
Mechanisms such as type of sport, playing position, weight, education, and race can inform our understanding of lifespan longevity, which places increased responsibility on future research to demystify and contextualize mortality risk in both eminent and non-eminent populations. In conclusion, while additional research studies are needed to address quality of life and wellness outcomes, this review highlights mortality trends among elite athletes and concludes that participation in elite sport is generally favorable to lifespan longevity.
Ethical Standards
This manuscript does not contain clinical studies or patient data.
References
Holt NL. Positive youth development through sport. UK: Routledge; 2008.
Baker J, Horton S. A review of primary and secondary influences on sport expertise. High Abil Stud. 2004;15:211–28.
Kettunen JA, Kujala UM, Kaprio J, Bäckmand H, Peltonen M, Eriksson JG, et al. All-cause and disease-specific mortality among male, former elite athletes: an average 50-year follow-up. Br J Sports Med. Published Online First: [2 Sept 2014]. doi:10.1136/bjsports-2013-093347
Kujala UM, Tikkanen HO, Sarna S, Pukkala E, Kaprio J, Koskenvuo M. Disease-specific mortality among elite athletes. The J of the Am Med Assoc. 2001;285:43–4.
Sarna S, Sahi T, Koskenvuo M, Kaprio J. Increased life expectancy of world class male athletes. Med and Sci in Sports and Exerc. 1993;2:237–44.
Sarna S, Kaprio J, Kujala UM, Koskenvuo M. Health status of former elite athletes. The Finnish experience. Aging Clin Exp Res. 1997;9:35–41.
Garatachea N, Santos-Lozano A, Sanchis-Gomar F, Fiuza-Luces C, Pareja-Galeano H, Emanuele E, et al. Elite athletes live longer than the general population: A meta-analysis. Mayo Clin Proc. 2014 Sep;89:1195–200. doi:10.1016/h.mayocp.2014.06.004. Epub 2014 Aug 12.
Irgens Å, Troland K, Thorsen E, Grønning M. Mortality among professional divers in Norway. Occup Med. 2013;63:537–43.
Coate D, Sun R. Survival estimates for elite male and female Olympic athletes and tennis championship competitors. Scand J of Med and Sci in Sports. 2013;23:722–7.
Lawler TP, Lawler FH, Gibson J, Murray R. Does the African-American-white mortality gap persist after playing professional basketball? A 59-year historical cohort study. Ann of Epidemiol. 2012;22:406–12.
Farahmand B, Broman G, de Faire U, Vågerö D, Ahlbom A. Golf: a game of life and death—reduced mortality in Swedish golf players. Scand J of Med and Sci in Sports. 2009;19:419–24.
Lehman EJ, Hein MJ, Baron SL, Gersic CM. Neurodegenerative causes of death among retired National Football League players. Neurol. 2012;79:1970–4.
Morcet J, Perrin M, Trégaro M, Carré F, Deugnier Y. Mortality in a cohort of 514 elite road cyclists. Sci and Sports. 2012;27:9–15.
Poznańska A, Gajewski AK. Mortality of male members of the Polish Olympic teams in 1981–1998. Przeglad Epidemiologiczny. 2001;55:305–12.
Reynolds R, Day S. Life expectancy and comparative mortality of Major League Baseball players, 1900–1999. Webmed Central Sports Medicine. 2012;3(5):WMC003380. doi:10.9754/journal.wmc.2012.003380.
Teramoto M, Bungum TJ. Mortality and longevity of elite athletes. J of Sci and Med in Sport. 2010;13:410–6.
Abel EL, Kruger ML. Athletes, doctors, and lawyers with first names beginning with “D” die sooner. Death Stud. 2010;34:71–81.
Baird LC, Newman CB, Volk H, Svinth JR, Conklin J, Levy ML. Mortality resulting from head injury in professional boxing. Neurosurg. 2010;67:1444–50.
Baron SL, Hein MJ, Lehman E, Gersic CM. Body mass index, playing position, race, and the cardiovascular mortality of retired professional football players. The Am J of Cardiol. 2012;109:889–96.
Clarke PM, Walter SJ, Hayen A, Mallon WJ, Heijmans J, Studdert DM. Survival of the fittest: retrospective cohort study of the longevity of Olympic medallists in the modern era. Br Med J. 2012. doi:10.1136/bmj.e8308.
Coate D, Schwenkenberg J. Survival function estimates for champions tour golfers. J of Sports Econ. 2012;14:656–63.
Grimsmo J, Maehlum S, Moelstad P, Arnesen H. Mortality and cardiovascular morbidity among long-term endurance male cross country skiers followed for 28–30 years. Scand J of Med and Sci in Sports. 2011;21:351–8. doi:10.1055/s-0028-1128150.
Koning RH, Amelink R. Medium-term mortality of Dutch professional soccer players. The Econ and Labour Relations Rev. 2012;23:55–68.
Kuss O, Kluttig A, Greiser KH. Longevity of soccer players: an investigation of all German internationals from 1908 to 2006. Scand J of Med and Sci in Sports. 2011;21:260–5.
Lawler TP, Lawler FH. Left-handedness in professional basketball: prevalence, performance, and survival. Percept and Mot Skills. 2011;113:815–24.
Lindqvist AS, Moberg T, Ehrnborg C, et al. Increased mortality rate and suicide in Swedish former elite male athletes in power sports. Scand J of Med and Sci in Sports. 2013. doi:10.1111/sms.12122.
Marijon E, Tafflet M, Antero-Jacquemin J, El Helou N, Berthelot G, Celermajer DS, et al. Mortality of French participants in the Tour de France (1947–2012). Eur Heart J. 2013;34:3145–50.
Sanchis-Gomar F, Olaso-Gonzalez G, Corella D, Gomez-Cabrera MC, Vina J. Increased average longevity among the “Tour de France” cyclists. Int J of Sports Med. 2011;32:644–7.
Smith G. Another look at baseball player initials and longevity. Percept and Mot Skills. 2011;112:211–6.
Smith G. The baseball hall of fame is not the kiss of death. Death Stud. 2011;35:949–55.
Zwiers R, Zantvoord FWA, Engelaer FM, van Bodegom D, van der Ouderaa FJG, Westendorp RGJ. Mortality in former Olympic athletes: retrospective cohort analysis. Br Med J. 2012;345:19–27.
Löllgen H, Böckenhoff A, Knapp G. Int J Sports Med. 2009 Mar;30:213–24. doi:10.1055/s-0028–1128150. Epub 2009 Feb 6.
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;e1000097. doi:10.1371/journal.pmed1000097
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. Newcastle-Ottawa Scale for assessing the quality of non-randomized studies in meta-analysis. Ottawa Hospital Research Institute website. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed March 14, 2015.
Abel EL, Kruger ML. Left-handed major-league baseball players and longevity re-examined. Percept and Mot Skills. 2004;99:990–2.
Abel EL, Kruger ML. Longevity of Major League Baseball players. Res in Sports Med. 2005;13:1–5.
Abel EL, Kruger ML. The longevity of baseball hall of famers compared to other players. Death Stud. 2005;29:959–63.
Abel EL, Kruger ML. The healthy worker effect in Major League Baseball revisited. Res in Sports Med. 2006;14:83–7.
Abel EL, Kruger ML. Precocity predicts shorter life for major league baseball players: confirmation of McCann’s precocity-longevity hypothesis. Death Stud. 2007;31:933–40.
Abel EL, Kruger ML. Symbolic significance of initials on longevity. Percept and Mot Skills. 2007;104:179–82.
Boren S, Erickson TB. Toxicological deaths of Major League Baseball players. J of Toxicol: Clin Toxicol. 1998;36:737–42.
Fudin R, Renninger L, Lembessis E, Hirshon J. Sinistrality and reduced longevity: Reichler’s 1979 data on baseball players do not indicate a relationship. Percept Mot Skills. 1993;76:171–82.
Halpern DF, Coren S. Do right-handers live longer? Nature. 1988;333:213.
Hicks RA, Johnson C, Cuevas T, Deharo D, Bautista J. Do right handers live longer? An updated assessment of baseball player data. Percept and Mot Skills. 1994;78:1243–7.
Kalist DE, Peng Y. Does education matter? Major League Baseball players and longevity. Death Stud. 2007;31:653–70.
Saint Onge JM, Rogers RG, Krueger PM. Major League Baseball players’ life expectancies. Soc Sci Q. 2008;89:817–30.
Waterbor J, Cloe P, Delzell E, Andjelkovich D. The mortality experience of Major League Baseball players. New Engl J of Med. 1988;318:1278–80.
Fafian Jr J. Mortality experience of National Basketball Association players. North Am Actuar J. 1997;1:45–8.
Abel EL, Kruger ML. The healthy worker effect in professional football. Res in Sports Med: An Int J. 2006;14:239–43.
Selden MA, Helzberg JH, Waeckerle JF. Early cardiovascular mortality in professional football players: fact or fiction? The Am J of Med. 2009;122:811–4.
Aggleton JP, Kentridge RW, Neave NJ. Evidence for longevity differences between left handed and right handed men: an archival study of cricketers. J Epidemiol Community Health. 1993;47:206–9.
Aggleton JP, Bland JM, Kentridge RW, Neave NJ. Handedness and longevity: archival study of cricketers. Br Med J. 1994;309:24–31.
Pärssinen M, Kujala U, Vartiainen E, Sarna S, Seppälä T. Increased premature mortality of competitive powerlifters suspected to have used anabolic agents. Int J of Sports Med. 2000;21:225–7.
Beaglehole R, Stewart A. The longevity of international rugby players. The NZ Med J. 1983;96:513–5.
Belli S, Vanacore N. Proportionate mortality of Italian soccer players: is amyotrophic lateral sclerosis an occupational disease? Euro J of Epidemiol. 2005;20:237–42.
Taioli E. All causes of mortality in male professional soccer players. Euro J of Public Heal. 2007;17:600–4.
Kanda H, Hayakawa T, Tsuboi S, Mori Y, Takahashi T, Fukushima T. Higher body mass index is a predictor of death among professional sumo wrestlers. J of Sports Sci and Med. 2009;8:711–2.
Menotti A, Amici E, Gambelli GC, Milazzotto F, Bellotti P, Capocaccia R, et al. Life expectancy in Italian track and field athletes. Euro J of Epidemiol. 1990;6:257–60.
Bianco M, Fabbricatore C, Sanna N, Fabiano C, Palmieri V, Zeppilli P. Elite athletes: is survival shortened in boxers? Int J of Sports Med. 2007;28:697–702.
Gajewski AK, Poznańska A. Mortality of top athletes, actors and clergy in Poland: 1924–2000 follow-up study of the longer term effect of physical activity. Euro J of Epidemiol. 2008;23:335–40.
Samaras TT, Storms LH, Elrick H. Longevity, mortality and body weight. Ageing Res Rev. 2002;1:673–91.
Baron S, Rinsky R. Health hazard evaluation report, National Football League players mortality study. Report No. HETA 88–085. Atlanta, GA: Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, 1994. http://www.cdc.gov/niosh/pdfs/nflfactsheet.pdf. Accessed 15 Sept 2014.
Hargrove T. Supersized in the NFL: many ex-players dying young. Scripps Howard News Service Online. 31 Jan 2006. http://sports.espn.go.com/nfl/news/story?id=2313476. Accessed 15 Sept 2014.
Barnwell B. Mere mortals: what we learned by comparing the mortality rates of baseball players and their NFL counterparts. Grantland. 17 Aug 2012.
McCann SJH. The precocity-longevity hypothesis: earlier peaks in career achievement predict shorter lives. Per Soc Psych Bull. 2001;27:1429–39.
Christenfeld N, Phillips DP, Glynn LM. What’s in a name: mortality and the power of symbols. J of Psychosom Res. 1999;47:241–54.
Phillips DP, Van Voorhees CA, Ruth TE. The birthday: lifeline or deadline? Psychosom Med. 1992;54:532–42.
Maher T, Gill B. Pro Football Encyclopedia. Macmillan, New York; 1997. http://grantland.com/features/comparing-mortality-rates-football-baseball/. Accessed 12 Sept 2014.
Samaras TT, Storms LH. Impact of height and weight on life span. Bull of the World Health Organ. 1992;70:259–67.
Bahrami H, Bluemke DA, Kronmal R, Bertoni AG, Lloyd-Jones DM, Shahar E, et al. Novel metabolic risk factors for incident heart failure and their relationship with obesity: the MESA (Multi-Ethnic Study of Atherosclerosis) study. J Am Coll Cardiol. 2008;51:1775–83.
Okorodudu DO, Jumean MF, Montori VM, Romero-Corral A, Somers VK, Erwin PJ, et al. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: a systematic review and meta- analysis. Int J Obes (Lond). 2010;34:791–9.
Omran AR. The epidemiologic transition: a theory of the epidemiology of population change. The Milbank Quart. 2005;83:731–57.
Kelly MP, Morgan A, Bonnefoy J, Butt J, Bergman V. The social determinants of health: developing an evidence base for political action. Final Report to World Health Organization Commission on the Social Determinants of Health. National Institute for Health and Clinical Excellence. 2007;1–165.
Sean Lahman’s Baseball Archive. 2010. http://www.baseball1.com.
Sorenson SC, Romano R, Azen SP, Schroeder T, Salem GJ. Life span exercise among elite intercollegiate student athletes. Sports Helath. 2014. doi:10.1177/1941738114534813.
Sorenson SC, Romano R, Scholefield RM, Martin BE, Gordon JE, Azen SP, et al. Holistic life-span health outcomes among elite intercollegiate student-athletes. J of Athl Train. 2014. doi:http://dx.doi.org/10.4085/1062-6050-49.3.18
Miles L. Physical activity and health. Nutr Bull. 2007;32:314–63.
Paluska SA, Schwenk TL. Physical activity and mental health. Sports Med. 2000;29:167–80.
Fogelholm M, Kaprio J, Sarna S. Healthy lifestyles of former Finnish world class athletes. Med Sci Sports Exerc. 1994;26:224–9.
Kujala UM, Sarna S, Kaprio J, Tikkanen HO, Koskenvuo M. Natural selection to sports, later physical activity habits, and coronary heart disease. Br J Sports Med. 2000;34:445–9.
Lavie CJ, O’Keefe JH, Sallis RE. Exercise and the heart—the harm of too little and too much. Curr Sports Med Rep. 2015;14:104–9.
O’Keefe JH, Patil HR, Lavie CJ, Magalski A, Vogel RA, McCullough PA. Potential adverse cardiovascular effects from excessive endurance exercise. Mayo Clin Proc. 2012;87:587–95.
Montgomery H, Safari L. Genetic basis of physical fitness. Annu Rev Anthropol. 2007;36:391–405.
Garatachea N, Lucia A. Genes, physical fitness and ageing. Ageing Res Rev. 2013;12:90–102.
Acknowledgements
This project was not funded.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing Interests
Both authors declare that they have no competing interests.
Authors’ contribution
SL and JB designed the study, developed the methodology, interpreted the data, and drafted the manuscript. SL collected the data. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Lemez, S., Baker, J. Do Elite Athletes Live Longer? A Systematic Review of Mortality and Longevity in Elite Athletes. Sports Med - Open 1, 16 (2015). https://doi.org/10.1186/s40798-015-0024-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-015-0024-x