
Abstract
Background
Early type IIIb endoleak is a very rare complication of endovascular aneurysm repair (EVAR).
Case presentation
An 87-year-old man was diagnosed with infrarenal abdominal aortic aneurysm. The patient underwent EVAR using the Endurant stent graft. Postoperative color duplex ultrasound revealed a regular row of pulsatile blood flow from the main body and left leg. The blood flow appeared to be bleeding from the stent suture lines because of its regularity. Type IIIb endoleak was suspected due to stent suture line fabric breakage but was not treated surgically or endovascularly because of the patient’s poor general health status. Six months later, contrast-enhanced CT demonstrated a deformation and enlargement of the aneurysm sac as well as an oozing of the contrast medium on the main body and left limb. Thereafter, he died of a subdural hematoma due to a fall. Autopsy showed no visible abnormal erosion or holes on the graft fabric, suggesting that suture line fabric breakage may have existed during the manufacturing process.
Conclusions
Although rare, type IIIb endoleaks can occur even in the perioperative period after EVAR. Early type IIIb endoleaks may not resolve spontaneously and should be treated promptly, if possible.
Similar content being viewed by others


Introduction
Type IIIb endoleak, defined as a fracture or tear in the graft material [1], is a rare complication of endovascular aneurysm repair (EVAR). Type IIIb endoleak is a high-pressure, high-risk leak [2] that leads to rapid growth of the aneurysmal sac and rupture [3]. Type IIIb endoleaks have been reported to occur as early as during operation to beyond 16 years postoperative, emphasizing the need for continuous surveillance [4, 5].
Herein, we report a rare case of type IIIb endoleak, likely due to stent suture line breakage and detected by color duplex ultrasound in the perioperative period, and we discuss the mechanism of occurrence and the fate of fabric breakage in early type IIIb endoleak.
Case report
An 87-year-old man presented with appetite loss and was referred to a neighborhood hospital. His medical history included angina pectoris after percutaneous coronary intervention, aortic valve stenosis, chronic heart failure, and stage 4 chronic kidney disease. He was taking antihypertensive and antiplatelet drugs (100 mg aspirin and 75 mg clopidogrel). Plain computed tomography (CT) of the abdomen and pelvis revealed an incidentally large infrarenal abdominal aortic aneurysm (AAA).
The patient was transferred to our university hospital for further treatment. Contrast-enhanced CT was performed to examine the anatomical features of the AAA. The maximum aneurysm diameter was 55 mm × 65 mm. The proximal neck was 24 mm in diameter and 28 mm in length with an angulation of 40°. The right and left common iliac arteries were 16 mm and 16 mm in diameter, respectively, which were within the instructions for use and anatomically suitable for EVAR. In addition, the left kidney was supplied with double renal arteries, the inferior branch of which originated immediately above the aneurysm. The branch was then sacrificed.
EVAR with the Endurant stent graft (Medtronic Endovascular; Santa Rosa, CA, USA) was performed using a mobile C-arm imaging system. The bilateral common femoral arteries were surgically exposed under sedation and regional anesthesia. A 4F catheter was placed just above the renal arteries through the left brachial artery for intraoperative angiography. The main body (28 mm × 16 mm × 166 mm) was positioned through the left common iliac artery, by which the left inferior renal artery was consequently sacrificed. The main body was extended to the right common iliac artery with a contralateral leg (16 mm × 24 mm × 124 mm). Balloon inflation with a compliant aortic occlusion balloon (Coda Balloon Catheter, Bloomington, IN, USA) was performed in the proximal neck, component junction, and bilateral distal neck but not excessively. Angiography revealed an endoleak in the proximal sealing zone. An aortic cuff was placed inside the proximal neck zone, because the type IV endoleak was indistinguishable from type Ia endoleak. Completion angiography showed that the endoleak had almost disappeared and the procedure was completed.
A color duplex ultrasound was performed 7 days after the operation instead of a contrast-enhanced CT because of severe renal insufficiency and revealed a regular row of pulsatile blood flow from the main body and left leg (Additional file 1: Movie 1A and Additional file 2: 1B; Fig. 1A, B). The blood flow appeared to be bleeding from the stent suture lines because of its regularity. Type IV but not type IIIb endoleak was suspected, likely due to stent suture line fabric breakage. However, it was not treated surgically or endovascularly but was followed by CT because of the patient’s poor general health status and the expectation of spontaneous resolution of the leak. The patient was transferred from our hospital to a neighborhood hospital.

Sagittal (A) and axial (B) views of the duplex scan showing a regular row of pulsatile blood flow from the main body and left limb
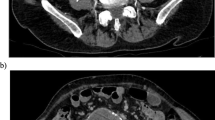
Six months later, the patient was readmitted to our hospital because of recurrent fever of unknown origin. Contrast-enhanced CT showed a deformation and enlargement of the aneurysm sac as well as oozing of the contrast medium on the main body and left limb (Fig. 2), suggestive of persistent type IIIb endoleak. However, the patient was considered unsuitable for further surgical intervention because of his deteriorating general health condition. He experienced subdural hematoma due to a fall during his hospital stay and died of uncontrolled subdural hematoma 7 weeks after readmission. Autopsy was performed with the informed consent of his family; it showed no visible abnormal erosion or hole on the graft fabric, suggesting that tiny fabric breakage may have existed along the stent suture line at the time of the manufacturing process.

Contrast-enhanced CT showing an oozing of contrast medium on the main body and left limb
Discussion
This case report highlights the occurrence of an early type IIIb endoleak with the Endurant stent graft, which is one of the most commonly used devices in Japan. Although type IIIb endoleaks occur on any devices and at any time after EVAR, they are very rare in the perioperative period [6].
An important issue is the mechanism of fabric defects in early type IIIb endoleaks. The following four hypotheses have been proposed to explain the damage to the fabric: (1) excessive endovascular manipulation; (2) excessive pressure of ballooning; (3) damage to the fabric by the acute tip of a stent displaced by severe neck angulations; and (4) manufacturing defect [6]. In this case, the autopsy showed no visible abnormal erosion or hole on the graft fabric, suggesting that fabric breakage may not have been caused by excessive endovascular manipulation, excessive pressure of ballooning, or acute tip, but may have existed along stent suture lines at the time of the manufacturing process. This is consistent with the report by Matsumura et al. that in a certain graft design, a broken suture line caused a small defect in the graft, leading to “microendoleaks” [7].
Furthermore, we contacted Medtronic, Inc. to ask if this could happen in the Endurant stent graft, but they were not aware of a similar case or provided no explanations.
Type IIIb endoleaks due to suture holes can occur in other commercially available stent grafts, in which metallic stents and polyester grafts are stitched together with sutures. During reoperation due to aneurysmal sac enlargement, intraoperative inspection revealed multiple oozing sites from stent suture line in the Zenith stent graft (Cook Inc, Bloomington, Indiana), the Talent abdominal stent graft (Medtronic, Santa Rosa, CA), and the Valiant thoracic stent graft (Medtronic, Santa Rosa, Calif) [8,9,10].
Another important issue is the fate of early type IIIb endoleaks. Minor fabric breakage along stent suture lines should not be of any clinical importance; in one report, blood leakage from minor fabric breakage spontaneously resolved in most cases [11]. However, no spontaneous resolution was observed in the report of Matsumura et al., and it did not occur even 6 months after stent graft placement in the present case. Therefore, early type III endoleaks should be treated promptly by endovascular or open surgery, or should be closely monitored if patients might not have been fit for intervention.
In addition, a publication review of type IIIb endoleaks indicated that definitive diagnosis is challenging even with multimodal imaging because of the dynamic nature of detection failure [4, 12]. In this study, color duplex ultrasound clearly demonstrated a regular row of pulsatile blood flow from the main body and left leg, suggesting a type IIIb endoleak likely due to stent suture line breakage. Color duplex ultrasound can provide real-time data in multiple planes, including the longitudinal and circumferential planes, and verify the location and flow characteristics of the endoleak [12]. The use of color duplex ultrasound for surveillance after EVAR will improve the risk management of stent-graft complications.
Conclusions
This case report describes a rare case of early type IIIb endoleak that is likely due to stent suture line fabric breakage in the Endurant stent graft. Although rare, type IIIb endoleaks can occur even in the perioperative period after EVAR. Early type IIIb endoleaks may not resolve spontaneously and should be treated promptly, if possible.
Availability of data and materials
Data sharing is not applicable to this article as no data sets were generated or analyzed during the current study.
Change history
11 May 2022
A Correction to this paper has been published: https://doi.org/10.1186/s40792-022-01443-4
Abbreviations
- EVAR:
-
Endovascular aneurysm repair
- CT:
-
Computed tomography
- AAA:
-
Abdominal aortic aneurysm
References
Cao P, De Rango P, Verzini F, Parlani G. Endoleak after endovascular aortic repair: classification, diagnosis and management following endovascular thoracic and abdominal aortic repair. J Cardiovasc Surg (Torino). 2010;51:53–69.
Baum RA, Stavropoulos SW, Fairman RM, Carpenter JP. Endoleaks after endovascular repair of abdominal aortic aneurysms. J Vasc Interv Radiol. 2003;14:1111–7.
van Marrewijk C, Buth J, Harris PL, Norgren L, Nevelsteen A, Wyatt MG. Significance of endoleaks after endovascular repair of abdominal aortic aneurysms: the EUROSTAR experience. J Vasc Surg. 2002;35:461–73.
Kwon J, Dimuzio P, Salvatore D, Abai B. Incidence of stent graft failure from type IIIB endoleak in contemporary endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2020;71:645–53.
Murakami Y, Toya N, Fukushima S, Ito E, Akiba T, Ohki T. Aneurysm sac enlargement 16 years after endovascular aortic aneurysm repair due to late type IIIb endoleak: a case report. Int J Surg Case Rep. 2018;49:215–8.
Abouliatim I, Gouicem D, Kobeiter H, Majeski M, Becquemin JP. Early type III endoleak with an Endurant endograft. J Vasc Surg. 2010;52:1665–7.
Matsumura JS, Ryu RK, Ouriel K. Identification and implications of transgraft microleaks after endovascular repair of aortic aneurysms. J Vasc Surg. 2001;34:190–7.
Nishibe T, Iwahashi T, Kamiya K, Kano M, Maruno K, Koizumi J, et al. Type IIIb Endoleak after endovascular aneurysm repair using the zenith stent graft. Vasc Endovasc Surg. 2019;53:515–9.
Seike Y, Nishibe T, Ogino H, Koizumi N. Hybrid repair of rare type IIIb endoleaks from an abdominal endograft: repeatedly undetected endoleaks. Interact Cardiovasc Thorac Surg. 2015;21:129–31.
Uehara K, Inoue T, Matsuo J, Sasaki H, Matsuda H. Type IIIB endoleak from stent suture lines of a thoracic endograft. J Vasc Surg Cases Innov Tech. 2019;5:214–7.
Wanhainen A, Nyman R, Eriksson MO, Bjorck M. First report of a late type III endoleak from fabric tears of a Zenith stent graft. J Vasc Surg. 2008;48:723–6.
Varsanik MA, Pocivavsek L, Babrowski T, Milner R. Diagnostic colour duplex ultrasound for type IIIb endoleak. EJVES Vasc Forum. 2020;47:43–6.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
ST, TN, MK, SA, TI, and HO participated in the treatment of the patient and reviewed the literature. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report at the initial consultation.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised: the Additional files were updated.
Supplementary Information
Additional file 1: Movie 1A. Sagittal view of the duplex scan showing a regular row of pulsatile blood flow from the main body and left limb (movie and still images)
Additional file 2: Movie 1B. Axial view of the duplex scan showing a regular row of pulsatile blood flow from the main body and left limb (movie and still images).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Takahashi, S., Nishibe, T., Kano, M. et al. Type IIIb endoleak due to stent suture line fabric breakage in the Endurant stent graft: a case report. surg case rep 8, 72 (2022). https://doi.org/10.1186/s40792-022-01415-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40792-022-01415-8