
Abstract
Background
Concurrent use of marijuana and alcohol in drivers is of increasing concern but its role in crash causation has not been well understood.
Methods
Using a case–control design, we assessed the individual and joint effects of marijuana and alcohol use on fatal crash risk. Cases (n = 1944) were drivers fatally injured in motor vehicle crashes in the United States at specific times in 2006, 2007 and 2008. Controls (n = 7719) were drivers who participated in the 2007 National Roadside Survey of Alcohol and Drug Use by Drivers.
Results
Overall, cases were significantly more likely than controls to test positive for marijuana (12.2% vs. 5.9%, p < 0.0001), alcohol (57.8% vs. 7.7%, p < 0.0001) and both marijuana and alcohol (8.9% vs. 0.8%, p < 0.0001). Compared to drivers testing negative for alcohol and marijuana, the adjusted odds ratios of fatal crash involvement were 16.33 [95% confidence interval (CI): 14.23, 18.75] for those testing positive for alcohol and negative for marijuana, 1.54 (95% CI: 1.16, 2.03) for those testing positive for marijuana and negative for alcohol, and 25.09 (95% CI: 17.97, 35.03) for those testing positive for both alcohol and marijuana.
Conclusions
Alcohol use and marijuana use are each associated with significantly increased risks of fatal crash involvement. When alcohol and marijuana are used together, there exists a positive synergistic effect on fatal crash risk on the additive scale.
Similar content being viewed by others

Background
Driving under the influence of drugs (DUID) is a serious public safety concern in the United States and around the world (Brady & Li 2013; Romano & Voas 2011; Kaplan et al. 2006; Berning et al. 2015; Hartman & Huestis 2013; Walsh et al. 2005; Dubois et al. 2015). About one third of fatally injured drivers in the United States tested positive for nonalcohol drugs and 20% tested positive for two or more drugs (Brady & Li 2013; Romano & Voas 2011; Kaplan et al. 2006). The prevalence of non-alcohol drugs in weekend nighttime drivers is about 20% (Berning et al. 2015). Marijuana is the most frequently detected nonalcohol drug and the concurrent use of marijuana and alcohol is the most frequently detected poly-drug combination in the general driver population (Berning et al. 2015) and in fatally injured drivers (Walsh et al. 2005; Dubois et al. 2015; Li et al. 2013). Over the past decade, traffic fatalities involving nonalcohol drugs have increased markedly while fatalities involving alcohol have remained fairly stable (Brady & Li 2013; Li et al. 2013; Brady & Li 2014). Specifically, the prevalence of marijuana positivity in fatally injured drivers had tripled from 4% in 1999 to 12% in 2010 (Brady & Li 2014). Evidence from experimental studies has shown that marijuana impairs almost every aspect of performance associated with safe driving (Lenné et al. 2010; Bosker et al. 2012; Downey et al. 2013; Hartman et al. 2015) and recent epidemiologic studies have found that marijuana use may double the risk of car crash involvement (Li et al. 2012, Asbridge et al. 2012).
Since 1996, 28 states and Washington, DC have enacted legislation to decriminalize marijuana for medical use (NCSL 2016). Of these states, eight have further decriminalized possession of small amounts of marijuana for adult recreational use (NCSL 2016). Colorado has registered an increase in fatal motor vehicle crashes involving marijuana since legalizing marijuana for medical use in 2000 (Urfer et al. 2014) compared to insignificant changes in states without medical marijuana laws (Salomonsen-sautel et al. 2014).
Young adults may be at a particularly high risk from the increased availability and potency of marijuana (Brady & Li 2013; Cerda et al. 2012; Lynne-Landsman et al. 2013; Harper et al. 2012; Wall et al. 2011; O’Malley & Johnston 2007). Given the increasing prevalence of DUID (Brady & Li 2013; Berning et al. 2015; Dubois et al. 2015; Brady & Li 2014) and the increasing permissibility and accessibility of marijuana (NCSL 2016), it is urgent to better understand the role of marijuana and its interaction with alcohol in motor vehicle crashes. Previous research on the interaction between alcohol and marijuana has reported conflicting results, with some indicating the interaction effect to be possibly synergistic (i.e., the combined effect is more than the sum of the net effects of marijuana and alcohol) (Bates & Blakely 1999; Brault et al. 2004; Biecheler et al. 2008; Ramaekers et al. 2000; Ramaekers et al. 2004; Sewell et al. 2009; Sutton 1983; Perez-Reyes et al. 1988) or additive (i.e., the combined effect is equal to the sum of the net effects of marijuana and alcohol) (Ramaekers et al. 2004; Sewell et al. 2009; Bramness et al. 2010; Drummer et al. 2004; Chesher 1986; Kelly et al. 2004) and others suggesting no additive effect (Lamers & Ramaekers 2001; Liguori et al. 2002). Understanding the role of marijuana and its interaction with alcohol in motor vehicle crashes is important in order to develop targeted, effective public health interventions and prudent use of resources in mitigating the rising prevalence of DUID. In the present study, we use a population-based case–control study design and data from two national surveillance systems to assess the individual and joint effects of marijuana and alcohol use on the risk of fatal crash involvement.
Methods
Data sources
Data for this study came from two sources: 1) the Fatality Analysis Reporting System (FARS) and 2) the 2007 National Roadside Survey of Alcohol and Drug Use by Drivers (NRS). Both data systems are sponsored and maintained by the National Highway Traffic Safety Administration (Washington, DC). The FARS is a census of all crashes that occur on public roads in the United States and result in at least one death of an occupant or non-occupant within 30 days of the crash (National Highway Traffic Safety Administration 2012). This data repository includes detailed information on the people and vehicles involved as well as circumstances of the crash. Data elements include driver characteristics (e.g., age, sex, survival status, drug and alcohol test results, driving history within the past 3 years), vehicle characteristics (e.g., model, make, type, year, weight rating) and crash circumstances (e.g., date, time, light and atmospheric conditions) (National Highway Traffic Safety Administration 2012). Data are obtained from various state documents such as police accident reports, death certificates, coroner/medical examiner reports, state vehicle registration files, hospital medical reports and vital statistics (National Highway Traffic Safety Administration 2012). To ensure accuracy and completeness, several programs continuously monitor the data and each entry is automatically checked for acceptable range and consistency. Toxicological testing results for nonalcohol drugs are available for only about one-third of fatally injured drivers nationwide due to incomplete testing and reporting (NHTSA 2010, 2012). However, 12 states performed drug testing on more than 80% of fatally injured drivers during the study period.
The 2007 NRS was a national field survey based on voluntary and anonymous random stops of non-commercial drivers at 300 locations across the contiguous United States (Lacey et al. 2009). The sample was selected using a multistage random sampling method that include four levels; primary sampling units, police jurisdictions, survey locations and passing-by drivers (Lacey et al. 2009). Drivers at the designated study locations were randomly stopped and invited to participate in the survey. Verbally consented drivers responded to questions about their trip origin, destination, demographics, mileage and drinking behavior and provided an oral fluid sample for drug testing as well as a breath sample for alcohol testing. The 2007 NRS was conducted between 10 PM and midnight and 1 AM to 3 AM on Fridays and Saturdays and 9:30 AM to 11:30 AM and 1:30 PM to 3:30 PM on Fridays during July 20 through December 1, 2007. The overall response rate for the 2007 NRS was 70.7% (Lacey et al. 2009). For each driver, the final overall sampling probability was equivalent to the product of sampling probabilities at each of the four levels of sampling. The final sampling weight was computed as the inverse of the overall sampling probability, i.e., data from drivers who were unlikely to be interviewed based on the sampling procedure used were given more weight than data from drivers who were more likely to be interviewed (Lacey et al. 2009). Additional details of the sampling method and study protocol are described elsewhere (Lacey et al. 2009).
Study design and study subjects
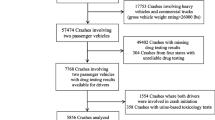
A population-based case–control design was used to assess the role of marijuana and the interaction effect of marijuana and alcohol on the risk of fatal crash involvement. Of the 3735 drivers in the sample, 1605 (42.9%) were excluded from the study due to missing drug testing results and 186 (4.9%) cases from Maryland, New Mexico and North Carolina were excluded because of concerns about the accuracy and reliability of drug testing data recorded in the FARS for these states (NHTSA 2012; SAMHSA 2010). Cases (n = 1944) were drivers with available drug testing results in the FARS who were involved in crashes at the same time of day and the same day of week as controls were interviewed (i.e., between 10 PM and midnight and 1 AM to 3 AM on Fridays and Saturdays and 9:30 AM to 11:30 AM and 1:30 PM to 3:30 PM on Fridays during July 20 through December 1 in 2006, 2007 and 2008 in the continental United States). Controls (n = 7719) were drivers with available drug testing results from oral fluid samples in the 2007 NRS. This study was deemed exempt from review under 45 CFR 46 by the Columbia University Medical Center Institutional Review Board (New York, NY).
Drug testing assessments
Drug tests for cases were performed on blood and/or urine specimens using radioimmunoassay techniques and liquid/gas chromatography coupled with mass spectometry (Kaplan et al. 2006; Li et al. 2011). Overall, 1759 (90.5%) of the 1944 cases included in the analysis had at least one drug test based on blood specimens. For each case, the FARS records the presence of up to three nonalcohol drugs (Kaplan et al. 2006; National Highway Traffic Safety Administration 2012). In the presence of multiple drugs, nonalcohol drugs are recorded in the following order: narcotics, depressants, stimulants, marijuana and other illicit drugs including phencyclidine, anabolic steroid, inhalant and medications (Kaplan et al. 2006; National Highway Traffic Safety Administration 2012). If a drug and its metabolite were detected, only the parent drug was recorded. Cannabinoids was the drug class for marijuana products such as hashish, pot or weed (National Highway Traffic Safety Administration 2012). Blood alcohol concentrations (BACs) were recorded separately from nonalcohol drugs. Drug tests for controls were performed on oral fluid samples that were screened using enzyme-linked immunosorbent assay and then confirmed using liquid/gas chromatography–mass spectrometry (National Highway Traffic Safety Administration 2012). BACs for controls were determined from breath samples measured using a preliminary breath test device (National Highway Traffic Safety Administration 2012; Lacey et al. 2009).
Statistical analysis
The associations of alcohol and marijuana use with the risk of fatal crash involvement were measured by estimated odds ratios (ORs) and 95% confidence intervals (95% CIs) with drivers who tested negative as the reference group. Crude ORs and 95% CIs were computed for driver age, sex, marijuana testing result and blood alcohol concentration. BAC was measured in grams per deciliter and a value of 0.01 g/dL or greater was considered positive. BAC was categorized into 3 levels; 0, 0.01–0.07 and ≥0.08 g/dL according to current per se laws in the United States. Separate and joint effects of marijuana and BAC levels were assessed, with drivers testing negative for marijuana and alcohol as the reference group. Interaction of marijuana and alcohol was first examined as a departure from multiplicativity, i.e., whether the joint effect of alcohol and marijuana differs from the multiplicative model expected on the basis of their separate net effects adjusting for demographic variables. To assess the presence, magnitude and direction of interaction on the multiplicative scale, the estimated adjusted odds ratios from the logistic regression models were substituted into the following equation (Rothman 1986; VanderWeele 2014):
where a value >1 implies presence of positive interaction, a value < 1 implies presence of negative interaction and a value of 1 implies absence of interaction. Interaction was also tested as a departure from additivity, i.e., whether the joint effects of alcohol and marijuana were in excess of the sum of their individual effects. Additive interaction was assessed based on three measures; the relative excess risk due to interaction (RERI), the attributable proportion due to interaction (API) and the synergy index (S) as shown below (Rothman 1986; Knol et al. 2012; VanderWeele & Knol 2014; Andersson et al. 2005):
where RERI = 0, API = 1 and S = 1 denotes absence of interaction. Estimates for RERI and 95% CI from the delta method were computed using an approach suggested by VanderWeele and Knol (VanderWeele & Knol 2014). Lastly, we assessed marijuana as an effect modifier (VanderWeele 2009), i.e., whether the effect of BAC on the risk of crash involvement was homogenous between marijuana positive and negative drivers. The Tarone adjusted Breslow Day test (Breslow & Day 1980; Tarone 1985) was used to assess homogeneity between marijuana strata. To ensure that our findings were robust, we performed three separate sensitivity analyses: first, by including only cases from the 12 states that tested more than 80% of fatally injured drivers during the study period; second, by analyzing weighted data accounting for the complex sampling design among controls (Lacey et al. 2009); and third, by conducting multiple imputation for missing marijuana testing results among cases to assess the potential bias from the missing marijuana data. The missing marijuana testing data were imputed using a logistic regression model with covariates including age, sex, license status, previous incidents, year, day and time of crash, use of restraint, police reported drug use, vehicle role in the crash, and region. Ten imputations were generated. All analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC). The multiple imputation was performed using the SAS callable software IVEware (Survey Research Center, Institute for Social Research, University of Michigan, Ann Arbor, MI).
Results
Compared to the excluded drivers, those included as cases (n = 1944) were younger (mean age =36.8 (standard deviation, 16.8) years vs. 40.1 (standard deviation, 19.7) years), more likely to be involved in nighttime crashes (70.1% vs. 63.3%, P < 0.0001), more likely to be male (82.8% vs. 76.9%, P < 0.0001), and more likely to be involved in a crash in the previous 3 years (12.8% vs. 11.0%, P = 0.01).
Overall, 12.2% of the 1944 cases and 5.9% of the 7719 controls tested positive for marijuana, yielding a crude OR of 2.21 (95% CI: 1.87, 2.60). Positive BACs (BAC ≥ 0.01 g/dL) were present in 57.8% of cases and 7.7% of controls, yielding a crude OR of 16.42 (95% CI: 14.52, 18.57). As expected, the risk of fatal crash involvement increased with BAC levels from a crude OR of 2.65 (95% CI: 2.16, 3.25) for 0.01–0.07 g/dL to 63.14 (95% CI: 52.01, 76.65) for ≥0.08 g/dl (Table 1). Male drivers and drivers aged 16–39 years as well as those aged 65 years and older were at significantly increased risk of fatal crash involvement (Table 1).
Relative to drivers who tested negative for both alcohol and marijuana, the estimated odds of fatal crash involvement increased 16 fold for those testing positive for alcohol and negative for marijuana, 1.5 fold for those testing negative for alcohol and positive for marijuana positive, and over 25 fold for those testing positive for both alcohol and marijuana (Table 2).
The joint odds ratio of marijuana at each BAC level (OR0.01–0.07g/dL = 4.38; OR≥0.08g/dL =95.26) was equivalent to the product of the individual marijuana and alcohol odds ratios at each BAC level (OR0.01–0.07g/dL = 1.56*2.81; OR≥0.08g/dL =1.56*61.11), indicating the absence of interaction on the multiplicative scale (Table 3). However, significant interaction was present on the additive scale for combined BAC levels (RERI = 2.94, 95% CI: 0.60, 5.28) and for the separate BAC levels [(RERI0.07g/dL =1.01, RERI≥0.08g/dL = 32.59), (API0.07g/Dl = 0.23, API≥0.08g/dL =0.34), (S≥0.08g/dL =1.43, S≥0.08g/dL = 1.55)].
The estimated odds ratios of fatal crash involvement increased with BAC level in similar degrees between drivers testing positive for marijuana and those testing negative for marijuana (Table 4) and there was no significant heterogeneity in the estimated odds ratios associated with BAC level between the marijuana strata (Breslow Day Chi-square = 2.49, p = 0.288). Estimated odds ratios from all three sensitivity analyses were consistent with those derived from the actual drug testing data (Appendix). Results from all sensitivity analyses showed a significant positive interaction on the additive scale [(RERI1 = 4.46 95% CI: 0.98, 7.95; RERI2 = 2.90 95% CI: 0.60, 5.27; RERI3 = 2.77 95% CI: 2.11, 3.42)], but no interaction on the multiplicative scale.
Discussion
Results of this study indicate that marijuana use is associated with a significantly increased risk of involvement in fatal motor vehicle crashes, as reported in recent epidemiological studies (Li et al. 2013; Li et al. 2012; Asbridge et al. 2012). The combined effect of marijuana and alcohol was greater than the sum of the net effects of the two substances, which suggests that each substance plays a significant role in drivers’ involvement in fatal motor vehicle crashes. All three measures (RERI, API and S) confirmed the presence of significant positive interaction between alcohol and marijuana on fatal crash risk on the additive scale. Assuming positive monotonicity, i.e., both exposures (marijuana and alcohol) are never protective, the positive additive interaction suffices for mechanistic or sufficient cause interaction (Tarone 1985; VanderWeele & Robins 2007), which is indicative of synergism. These findings are important because the possible interaction between marijuana and alcohol on driving safety has long been a cause of concern (Sutton 1983; Gjerde & Kinn 1991; Stramer & Bird 1984) and recent toxicological data have shown that more that 20% of drivers fatally injured in motor vehicle crashes test positive for two or more drugs (Brady & Li 2013; Romano & Voas 2011; Kaplan et al. 2006) with alcohol and marijuana being the most common combination (Brady & Li 2013; Walsh et al. 2005).
Our results are consistent with previous experimental and epidemiological studies that have reported additive effects of alcohol and marijuana on driving performance and crash risk (Dubois et al. 2015; Bates & Blakely 1999; Sewell et al. 2009; Doty et al. 1992; Belgrave et al. 1979; Drummer et al. 2004; Chesher 1986) and possibly synergistic (Brault et al. 2004; Biecheler et al. 2008; Sutton 1983; Perez-Reyes et al. 1988) effects. For instance, a recent case–control study found that, relative to drivers using neither alcohol nor marijuana, drivers who tested positive for both alcohol (BAC ≤ 0.08 g/dL) and marijuana had up to 128% increased odds of committing an unsafe driver action compared to 16% for those using marijuana alone and 117% for those using alcohol (BAC ≤ 0.08 g/dL) alone (Dubois et al. 2015). Previous studies that reported modest or no interaction between marijuana and alcohol (Lamers & Ramaekers 2001; Liguori et al. 2002) analyzed very small study samples and assessed the effect of drugs on isolated experimental dependent measures such as reaction time (Liguori et al. 2002) or visual search at intersections (Lamers & Ramaekers 2001) instead of crash involvement in real traffic situations. In addition to the large sample size, this study was based on data from 46 states, including 10 out of 13 states that had legalized marijuana for medical use as of 2008. Therefore, the findings of this study could be considered more representative of the United States than those reported in previous studies.
The present study provides valuable evidence for understanding the interaction of drugs and driving safety. Many models in epidemiologic studies are inherently multiplicative and tend to evaluate interaction on the multiplicative scale only (Knol et al. 2009). This study assessed interaction on both multiplicative and additive scales. There has been debate in the epidemiologic literature as to which scale is better for assessing interactions (Blot & Day 1979; Saracci 1980; Rothman et al. 1980). Some epidemiologists have pointed out the potential limitations of using statistical interaction to draw conclusions about biological interaction (Siemiatycki & Thomas 1981; Thompson 1991; Cordell 2002). In this study, we assumed three sufficient causes of the outcome (fatal crash involvement), with marijuana, alcohol and both marijuana and alcohol as the three disparate causal mechanisms. Biological interaction was assessed where both marijuana and alcohol are single component causes in a combined causal mechanism. The additive model underpins the methods for assessing biological interaction (Rothman et al. 1980; Rothman 1976) and the notion of biological synergism (Rothman 1976), which may be difficult to interpret from multiplicative models. Although in some cases the multiplicative scale may naturally correspond to interaction mechanisms (Siemiatycki & Thomas 1981), the additive scale is of greater public health importance (VanderWeele 2011) because it allows researchers to discern the effect difference among subgroups.
The risk of fatal crash involvement associated with alcohol use appears to be homogenous between marijuana strata, indicating that marijuana is not a significant effect modifier in the BAC-fatal crash risk relationship. The homogeneity test results corroborate the absence of interaction on the multiplicative scale. At low doses, marijuana and alcohol may be mostly associated with impairment of low level operational driving skills (Lamers & Ramaekers 2001; Liguori et al. 2002) with gradual impairment of higher-level driving skills such as hazard perception, risk management and self-control as the doses increase. With the rising prevalence of marijuana use, potency, social tolerance, early age of onset and availability (Brady & Li 2014; Cerda et al. 2012; Lynne-Landsman et al. 2013; O’Malley & Johnston 2007), public health efforts should focus on strengthening and expanding drug testing as well as intervention programs for drivers. Although it is illegal to drive under the influence of alcohol and drugs in all states, almost all of the one million registered medical marijuana users are from states with older and less regulated programs that have minimal physician or state oversight (Williams et al. 2016). Therefore it is urgent to develop intervention programs to reduce the unintended health consequences of state laws legalizing marijuana for medical and/or recreational use, such as injuries and fatalities resulting from DUID.
This study has several notable limitations. First, drug testing protocols vary from state to state (Asbridge 2014). Some states have low testing rates, which may introduce selection bias. However, only subjects with known drug testing results were included in this study and results from the sensitivity analyses, including multiply imputed drug testing results for excluded drivers, were consistent with those from the actual testing data. Second, there are additional possible causal components for crash involvement that are not measured in the study, such as driver’s health status, comorbidity, medication use and weather condition and other environmental factors. Third, a positive test for marijuana indicates marijuana use but not necessarily marijuana-induced impairment as marijuana metabolites could remain in the blood for weeks after use (Voas et al. 2011; Skopp & Potsch 2008). Finally, marijuana tests were based on blood and urine specimens for cases and oral fluids for controls. The oral fluid testing method is widely used for detecting recent use of drugs such as marijuana, with reported sensitivity of 86–90% and specificity of 75–77% (Bosker & Huestis 2009; Desrosiers et al. 2012).
Conclusions
Alcohol and marijuana are each associated with heightened risk of fatal crash involvement. When alcohol and marijuana are used together, there exists a positive synergistic effect on the risk of fatal crash involvement on the additive scale. These results suggest that the combined effects of alcohol and marijuana on fatal crash risk are significantly greater than the sum of their separate effects. With the rising prevalence of marijuana use, potency, social tolerance, early age of onset and availability, drug testing in drivers should be strengthened and expanded and effective intervention programs to reduce DUID and its adverse consequences should be implemented. Our findings imply that countermeasures simultaneously targeting alcohol-impaired driving and DUID might be more effective in improving driving safety than interventions targeting alcohol-impaired driving and DUID in isolation. Epidemiologic research aimed at quantifying the dose–response effect of marijuana on crash risk is urgently needed.
Abbreviations
- AP:
-
Attributable proportion due to interaction
- BAC:
-
Blood alcohol concentration
- CI:
-
Confidence interval
- DC:
-
District of Columbia
- FARS:
-
Fatality Analysis Reporting System
- NHTSA:
-
National Highway Traffic Safety Administration
- NRS:
-
National Roadside Survey of Alcohol and Drug Use by Drivers
- OR:
-
Odds ratio
- RERI:
-
Relative excess risk due to interaction
- S:
-
The synergy index
References
Andersson T, Alfredsson L, Källberg H, Zdravkovic S, Ahlbom A. Calculating measures of biological interaction. Eur J Epidemiol. 2005;20(7):575–9.
Asbridge M. Driving after marijuana use: the changing face of “impaired” driving. JAMA Pediatr. 2014;168(7):602–4.
Asbridge M, Hayden JA, Cartwright JL. Acute cannabis consumption and motor vehicle collision risk: systematic review of observational studies and meta-analysis. BMJ. 2012;344:e536.
Bates MN, Blakely TA. Role of cannabis in motor vehicle crashes. Epidemiol Rev. 1999;21(2):222–32.
Belgrave BE, Bird KD, Chesher GB, Jackson DM, Lubbe KE, Starmer GA, et al. The effect of (−) trans-delta9-tetrahydrocannabinol, alone and in combination with ethanol, on human performance. Psychopharmacol (Berl). 1979;64(2):243–6.
Berning A, Compton R, Wochinger K. Results of the 2013–2014 National Roadside Survey of alcohol and drug use by drivers. Washington: National Highway Traffic Safety Administration; 2015 (Traffic Safety Facts Research Note. Report No. DOT HS 812 118).
Biecheler MB, Peytavin JF, SAM Group, Facy F, Martineau H. SAM survey on “drugs and fatal accidents”: search of substances consumed and comparison between drivers involved under the influence of alcohol or cannabis. Traffic Inj Prev. 2008;9(1):11–21.
Blot WJ, Day NE. Synergism and interaction: are they equivalent? Am J Epidemiol. 1979;110(1):99–100.
Bosker WM, Huestis MA. Oral fluid testing for drugs of abuse. Clin Chem. 2009;55(11):1910–31.
Bosker WM, Kuypers KP, Theunissen EL, Surinx A, Blankespoor RJ, Skopp G, et al. Medicinal Δ (9) -tetrahydrocannabinol (dronabinol) impairs on-the-road driving performance of occasional and heavy cannabis users but is not detected in Standard Field Sobriety Tests. Addiction. 2012;107(10):1837–44.
Brady JE, Li G. Prevalence of alcohol and other drugs in fatally injured drivers. Addiction. 2013;108(1):104–14.
Brady J, Li G. Trends in alcohol and other drugs detected in fatally injured drivers in the United States, 1999–2010. Am J Epidemiol. 2014;179(6):692–9.
Bramness JG, Khiabani HZ, Mørland J. Impairment due to cannabis and ethanol: clinical signs and additive effects. Addiction. 2010;105(6):1080–7.
Brault M, Dussault C, Bouchard J, et al. The contribution of alcohol and other drugs among fatally injured drivers in Quebec. [Abstract]. 2004. Presented at the 17th International conference on Alcohol, Drugs and Traffic Safety, Glasgow, United Kingdom, August 8–13.
Breslow NE, Day NE. Statistical methods in cancer research: Volume 1 - The analysis of case–control studies. Lyon: International Agency for Research on Cancer; 1980. IARC Scientific Publications No. 32.
Cerda M, Wall M, Keyes KM, Galea S, Hasin D. Medical marijuana laws in 50 states: investigating the relationship between state legalization of medical marijuana and marijuana use, abuse and dependence. Drug Alcohol Depend. 2012;120(1–3):22–7.
Chesher GB. The effects of alcohol and marijuana in combination: A review. Alcohol, Drugs and Driving. 1986;2(3):105–19.
Cordell HJ. Epistasis: what it means, what it doesn’t mean, and statistical methods to detect it in humans. Hum Mol Genet. 2002;11(20):2463–8.
Desrosiers NA, Lee D, Schwope DM, Milman G, Barnes AJ, Gorelick DA, et al. On-site test for cannabinoids in oral fluid. Clin Chem. 2012;58(10):1418–25.
Doty P, Dysktra LA, Picker MJ. Delta 9-tetrahydrocannabinol interactions with phencyclidine and ethanol: effects on accuracy and rate of responding. Pharmacol Biochem Behav. 1992;43(1):61–70.
Downey LA, King R, Papafotiou K, Swann P, Ogden E, Boorman M, et al. The effects of cannabis and alcohol on simulated driving: Influences of dose and experience. Accid Anal Prev. 2013;50:879–86.
Drummer OH, Gerostamoulos J, Batziris H, Chu M, Caplehorn J, Robertson MD, et al. The involvement of drugs in drivers of motor vehicles killed in Australianroad traffic crashes. Accid Anal Prev. 2004;36(2):239–48.
Dubois S, Mullen N, Weaver B, Bedard M. The combined effects of alcohol and cannabis on driving: Impact on crash risk. Forensic Sci Int. 2015;248:94–100.
Gjerde H, Kinn G. Impairment of drivers due to cannabis in combination with other drugs. Forensic Sci Int. 1991;50(1):57–60.
Harper S, Strumpf EC, Kaufman JS. Do medical marijuana laws increase marijuana use? Replication study and extension. Ann Epidemiol. 2012;22(3):207–12.
Hartman RL, Huestis MA. Cannabis effects on driving skills. Clin Chem. 2013;59(3):478–92.
Hartman RL, Brown TL, Milavetz G, Spurgin A, Pierce RS, Gorelick DA, et al. Cannabis effects on driving lateral control with and without alcohol. Drug Alcohol Depend. 2015;154:25–37.
Kaplan J, Kraner J, Paulozzi L. Alcohol and other drug use among victims of motor-vehicle crashes-West Virginia, 2004–2005. MMWR Morb Mortal Wkly Rep. 2006;55(48):1293–6.
Kelly E, Darke S, Ross J. A review of drug use and driving: epidemiology, impairment, risk factors and risk perceptions. Drug Alcohol Rev. 2004;23(3):319–44.
Knol MJ, Vanderweele TJ. Recommendations for presenting analyses of effect modification and interaction. Int J Epidemiol. 2012;41(2):514–20.
Knol MJ, Egger M, Scott P, Geerlings MI, Vandenbroucke JP. When one depends on the other: reporting of interaction in case–control and cohort studies. Epidemiology. 2009;20(2):161–6.
Lacey JH, Kelley-Baker T, Furr-Holden D, Voas R, Moore C, Brainard K, et al. 2007 National Roadside Survey of Alcohol and Drug Use by Drivers: Methodology. Washington: National Highway Traffic Safety Administration; 2009. DOT HS 811 237.
Lamers CT, Ramaekers JG. Visual search and urban driving under the influence of marijuana and alcohol. Hum Psychopharmacol. 2001;16(5):393–401.
Lenné MG, Dietze PM, Triggs TJ, Walmsley S, Murphy B, Redman JR. The effects of cannabis and alcohol on simulated arterial driving: Influences of driving experience and task demand. Accid Anal Prev. 2010;42(3):859–66.
Li L, Zhang X, Levine B, Li G, Zielke HR, Fowler DR. Trends and pattern of drug abuse deaths in Maryland teenagers. J Forensic Sci. 2011;56(4):1029–33.
Li MC, Brady JE, DiMaggio CJ, Lusardi AR, Tzong KY, Li G. Marijuana use and motor vehicle crashes: A meta-analysis. Epidemiol Rev. 2012;34(1):65–72.
Li G, Brady JE, Chen Q. Drug use and fatal motor vehicle crashes: a case–control study. Accid Anal Prev. 2013;60:205–10.
Liguori A, Gatto CP, Jarrett DB. Separate and combined effects of marijuana and alcohol on mood, equilibrium and simulated driving. Psychopharmacol (Berl). 2002;163(3–4):399–405.
Lynne-Landsman SD, Livingston MD, Wagenaar AC. Effects of state medical marijuana laws on adolescent marijuana use. Am J Public Health. 2013;103(8):1500–6.
National Conference of State Legislatures (NCSL). 2016. State Medical Marijuana Laws. http://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx. Accessed 5 Apr 2016.
National Highway Traffic Safety Administration (NHTSA). Traffic Safety Facts: Drug Involvement of Fatally Injured Drivers. Washington: US Department of Transportation; 2010.
National Highway Traffic Safety Administration (NHTSA). FARS Analytical User’s Manual 1975–2011. Washington: National Highway Traffic Safety Administration; 2012. DOT HS 811 693.
O’Malley PM, Johnston LD. Drugs and driving by American high school seniors, 2001–2006. J Stud Alcohol Drugs. 2007;68(6):834–42.
Perez-Reyes M, Hicks RE, Bumberry J, Jeffcoat AR, Cook CE. Interaction between marihuana and ethanol: effects on psychomotor performance. Alcohol Clin Exp Res. 1988;12(2):268–76.
Ramaekers JG, Robbe HW, O’Hanlon JF. Marijuana, alcohol and actual driving performance. Hum Psychopharmacol. 2000;15(7):551–8.
Ramaekers JG, Berghaus G, Van Laar M, Drummer OH. Dose related risk of motor vehicle crashes after cannabis use. Drug Alcohol Depend. 2004;73(2):109–19.
Romano E, Voas RB. Drug and alcohol involvement in four types of fatal crashes. J Stud Alcohol Drugs. 2011;72(4):567–76.
Rothman KJ. Causes. Am J Epidemiol. 1976;104(6):587–92.
Rothman KJ. Modern Epidemiology. 1st ed. Boston: Little, Brown and Company Publishers; 1986.
Rothman KJ, Greenland S, Walker AM. Concepts of interaction. Am J Epidemiol. 1980;112(4):467–70.
Salomonsen-Sautel S, Min SJ, Sakai JT, Thurstone C, Hopfer C. Trends in fatal motor vehicle crashes before and after marijuana commercialization in Colorado. Drug Alcohol Depend. 2014;140:137–44.
Saracci R. Interaction and synergism. Am J Epidemiol. 1980;112(4):465–6.
Sewell RA, Poling J, Sofuoglu M. The effect of cannabis compared with alcohol on driving. Am J Addict. 2009;18(3):185–93.
Siemiatycki J, Thomas DC. Biological models and statistical interactions: an example from multistage carcinogenesis. Int J Epidemiol. 1981;10(4):383–7.
Skopp G, Potsch L. Cannabinoid concentrations in spot serum samples 24–48 hours after discontinuation of cannabis smoking. J Anal Toxicol. 2008;32(2):160–4.
Stramer GA, Bird KD. Investigating drug-ethanol interactions. Br J Clin Pharmacol. 1984;18(S1):27–35.
Substance Abuse and Mental Health Services Administration. National Survey on Drug Abuse and Health Report. State Estimates of Drunk and Drugged Driving. Rockville: Substance Abuse and Mental Health Services Administration; 2010.
Sutton LR. The effects of alcohol, marihuana and their combination on driving ability. J Stud Alcohol. 1983;44(3):438–45.
Tarone RE. On heterogeneity tests based on efficient scores. Biometrika. 1985;72(1):91–5.
Thompson WD. Effect modification and the limits of biological inference from epidemiologic data. J Clin Epidemiol. 1991;44(3):221–32.
Urfer S, Morton J, Beall V, Feldmann J, Gunesch J. Analysis of Δ 9-tetrahydrocannabinol driving under the influence of drugs cases in Colorado from January 2011 to February 2014. J Anal Toxicol. 2014;38(8):575–81.
VanderWeele TJ. On the distinction between interaction and effect modification. Epidemiology. 2009;20:863–71.
VanderWeele TJ. A word and that to which it once referred: assessing “biologic” interaction. Epidemiology. 2011;22(4):612–3.
VanderWeele TJ, Knol MJ. A tutorial on interaction. Epidemiol Methods. 2014;3(1):33–72.
VanderWeele TJ, Robins JM. The identification of synergism in the sufficient-component-cause framework. Epidemiology. 2007;18:329–39.
Voas RB, DuPont RL, Talpins SK, Shea CL. Towards a national model for managing impaired driving offenders. Addiction. 2011;106(7):1221–7.
Wall MM, Poh E, Cerdá M, Keyes KM, Galea S, Hasin DS. Adolescent marijuana use from 2002 to 2008: higher in states with medical marijuana laws, cause still unclear. Ann Epidemiol. 2011;21(9):714–6.
Walsh JM, Flegel R, Atkins R, Cangianelli LA, Cooper C, Welsh C, et al. Drug and alcohol use among drivers admitted to a Level-1 trauma center. Accid Anal Prev. 2005;37(5):894–901.
Williams AR, Olfson M, Kim JH, Martins SS, Kleber HD. Older, less regulated medical marijuana programs have much greater enrollment rates than newer ‘medicalized’ programs. Health Aff (Millwood). 2016;35(3):480–8.
Acknowledgements
This research was supported in part by the National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (grant 1 R49 CE002096). The contents of the manuscript are solely the responsibility of the authors and do not necessarily reflect the official views of the funding agency.
Authors’ contributions
SC literature review; statistical analysis, drafting of manuscript; critical revision. GL study concept and design, supervision of research plan implementation, interpretation of the results and critical revision. QC statistical analysis and critical revision. All authors read and approved the final manuscript.
Competing interests
The corresponding author for the paper is also the Editor-in-chief of the journal Injury Epidemiology. He was not involved in the review or handling of this manuscript. The authors declare that they have no competing interests.
Declarations
This study was deemed exempt from review under 45 CFR 46 by the Columbia University Medical Center Institutional Review Board (New York, NY).
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Chihuri, S., Li, G. & Chen, Q. Interaction of marijuana and alcohol on fatal motor vehicle crash risk: a case–control study. Inj. Epidemiol. 4, 8 (2017). https://doi.org/10.1186/s40621-017-0105-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40621-017-0105-z