
Abstract
Background
Fitness facilities provide an avenue to engage in physical activity, which is widely encouraged to improve health. However, there is risk of injury. This study aimed to identify the specific causes of injuries sustained at fitness facilities and the activity being participated in, to aid in the development of injury prevention strategies.
Methods
Analysis of routinely collected emergency department case-series data were obtained from July 1999 to June 2013. Fitness activity-related injury cases were identified from narratives of injury events, with narrative information recoded into cause of injury and activity at time of injury categories. Recoded data were then analysed.
Results
Overall, 2,873 cases were identified that specified the exact cause of injury associated with injuries that occurred at fitness facilities. Injuries due to overexertion were most common overall (36.2% of all cases), as well as the main cause of injuries related to general free weight activities (52.6% of this activity) and group exercise classes (35.9%). Crush injuries due to falling weights were common for all free weight activities. Falls and awkward landings were common causes of injuries during group exercise classes (28.5% and 25.8%, respectively). Trips and falls were common throughout facilities, as well as from cardiovascular equipment more specifically.
Conclusions
Detailed information on the causes of injuries allows the development of injury prevention strategies for fitness facilities and fitness activities. Facilities should implement risk management strategies to reduce the risk of injuries in their clientele, based on the identified major causes of injury in this study.
Similar content being viewed by others


Background
It is widely accepted that physical activity can enhance overall health and prevent chronic illness (Bull et al. 2004). The fitness industry provides an avenue for people to be physically active and is increasing in popularity, particularly through the provision of fitness facilities (Fitness Australia 2012). According to the Australian 2010 Exercise Recreation and Sport Survey, fitness activities are the second most common sport or recreation activity undertaken by people aged 15+ years over the previous 12-month period (Australian Sports Commission 2010). In America, over 60% of those aged 6+ years participated in fitness sports (e.g. treadmill, free weights, boot camp, group exercise classes) in the previous 12 months and this is considered the most popular physical activity, according to the Physical Activity Council’s 2014 Participation Report (Physical Activity Council 2014).
Unfortunately, however, with all forms of physical activity, there is a risk of injury. Fitness activities performed in fitness facilities can have the potential to cause harm and injuries sustained by fitness activity participants can result in interruptions to their daily life, loss of income, temporary or permanent disability, or in severe cases, death (Andrew et al. 2014, Gray and Finch 2015). As the popularity of fitness facilities increases, so too does the risk of injury on a pure exposure basis.
Very few studies exist that investigate the injuries sustained during fitness activities, and most focus only on describing the types of injuries sustained (Thompson et al. 2001, Hayes 1985, Quatman et al. 2009, Salmon et al. 2000) or the rate/frequency with which they occur (Garrick et al. 1986, Jones et al. 2000, Kerr et al. 2010). Even fewer studies have given attention to understanding the specific causes of such injuries in the fitness centre context. The causes of injuries must first be identified to enable development and implementation of targeted prevention measures to reduce the future risk of such injuries.
Emergency department data which contains narrative details on the incidents and causal factors leading to injury is a potentially useful source of injury data (Gray and Finch 2015). Databases of this nature describe cases where the person injured has deemed the injury severe (or acute) enough for them to seek treatment at a hospital emergency department. This study aimed to examine the narrative text descriptions of emergency department presentations in Victoria, Australia, to identify the reported factors associated with the causes and/or mechanisms of injuries sustained at fitness facilities.
Methods
Data were obtained from the Victorian Emergency Minimum Dataset (VEMD) through the Victorian Injury Surveillance Unit (VISU). Individual participant consent was not required as VISU has approval from the Human Research Ethics Committee at the Victorian Department of Health to provide summary data for this research. The VEMD, as managed by VISU, was queried to identify all injury-related emergency department presentations where the injury had occurred as a result of fitness-related activities over the entirety of the database (July 1999 to June 2013, inclusive).
The VEMD routinely collects data on injury presentations to all 39 Victorian public hospitals that have a 24-h emergency department, however not all of these contributed to the VEMD over the whole reporting period. Case selection from this database was based on targeted keyword text searching of 250-character narratives provided with each case. The purpose of the 250-character narrative is to provide more information about the specific circumstances surrounding the injury than is contained in the coded data. A keyword query for words/phrases relating to typical activities and equipment commonly used in fitness facilities was performed. This included terms such as treadmill, elliptical trainer, rowing machine, aerobics, weight training, barbell, dumbbell and cross training. Selected cases were restricted to people aged 15+ years, given that most fitness facilities enforce a minimum age requirement.
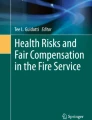
The extracted data required cleaning to remove irrelevant cases that were mistakenly selected by the keyword search (see Figure 1). Figure 1 shows the steps that were performed to condense and refine the dataset and includes examples of exclusions, so that only injuries that occurred within fitness facilities were included in the dataset to be analysed.

The number of emergency department presentations retained after each associated data cleaning process.
Using the information given in the narrative, each of the 3,880 extracted cases was manually reviewed and assigned 1 of 19 specific causes as shown in Table 1:
Each of the n = 3,880 narratives was then manually reviewed and categorised into 1 of 29 specific activity groups that were subsequently collapsed into seven broad activity groups. These activity groups were determined by the information provided in the narrative about what fitness activity was being participated in at the time of injury and are shown in Table 2.
Cases that did not specify the exact cause of injury were excluded for the purposes of this study, therefore the final total number of cases analysed was 2,873. Cases were retained if it was clear that they were associated with fitness activities even when the specific fitness activity was not mentioned in the narrative.
Descriptive frequencies and cross-tabulations were performed in SPSS Version 21 to determine the leading fitness activities and causes that resulted in hospital ED treatment.
Results
Over the 14 years of the VEMD, there were at least 2,873 cases associated with injuries that occurred at fitness facilities that specified the exact cause of the injury.
There were 807 cases (28.1%) where the narrative reported that an injury had occurred during exercise at a fitness facility but did not state the specific exercise being participated in at the time of injury. Similarly, there were 210 cases (7.3%) that stated an injury occurred when using, or due to, a piece of fitness equipment but did not further specify the exact type. For the purposes of Table 3, to determine the most common fitness activities associated with fitness injury-related ED presentations, the cases that did not specify the fitness activity or equipment were removed (n = 1,017, 35.4% of cases).
Of the broad fitness activities that presented to EDs, resistance/weight training injuries accounted for 55.6% of specified activities, the highest of all activities. Of the specific fitness activities that presented to EDs, general free weights were the most common (42.2%). However when all free weight activities were combined (general free weights, dumbbell, squats, lunges and deadlifts, bench press, barbell), these accounted for 55.2% of all specified activity cases (see Table 3).
Amongst the specific causes, overexertion/strenuous/unnatural movements were associated with the highest number of fitness injury-related ED presentations (36.2%) followed by crushed by falling/dropped weights (16.3%), trip/fall throughout facility (12.5%) and awkward landing or twist during exercise (12.0%).
The six most common fitness activities and specific causes resulting in an ED presentation are summarised in Table 4. Over half of all fitness injury-related ED presentations were associated with the six most common fitness activities (53.1%). When the cases with unknown activities and equipment use at the time of injury were removed, however, 83.0% of the fitness injury-related ED presentations were associated with these top six activities. The majority of all fitness injury-related ED presentations were associated with the six most common causes (91.7%).
Table 4 shows that for both general free weights and exercise group classes, overexertion/strenuous/unnatural movements accounted for the highest proportion of injuries for each activity (52.6% and 35.9% of each activity, respectively). Hit/contact with equipment/wall was common for boxing-related activities (47.4%), and falls from motorised equipment were associated with the majority of treadmill injuries (70.7%). Dumbbell injuries were most commonly due to weights falling or dropping on the individual (78.4%).
Injuries due to overexertion/strenuous/unnatural movements most commonly occurred during general free weight activities (39.7% of injuries associated with this cause), and that was also the activity most often associated with crushed by falling/dropped weights (58.1% of injuries associated with this cause). When all free weight activities were combined, they accounted for 84.4% of crush injuries due to falling or dropped weights. More than half of trips/falls throughout the facility were during an unspecified activity (and provided no further information other than ‘trip/fall at facility’) (60.6%).
Eight percent of all presentations to EDs were considered severe enough to be subsequently hospitalised. The three most common causes that led to hospital admission, following ED presentation, were crushed by falling/dropped weights, overexertion/strenuous/unnatural movement and trip/fall throughout facility; however, these only accounted for 11.5%, 5.0% and 12.8% respectively of all cases associated with each of these causes. All free weight activities combined were the most common activities that led to hospitalisation (35.7% of hospitalisations), followed by treadmill and exercise group class (10% each).
Discussion
The risk of injury from physical activity can interfere with the enjoyment of participation and reduce the long-term health benefits that physical activity can provide. Injuries can result in negative changes to daily activities, lost work time, poor quality of life, disability or in extreme cases death. To our knowledge, this study is the first to provide detailed information about the causes of fitness-related injuries on a large case series. Preventing injuries is therefore very important, but knowledge of how these injuries are occurring is required prior to designing and implementing injury prevention strategies. The findings from this study provide evidence for injury prevention strategy design and development and form a basis for risk management procedures that can lead to a reduction in incidents at fitness facilities.
Only three previous published studies have explored the causes of injuries associated with fitness activities (Gray and Finch 2015, Salmon et al. 2000, Kerr et al. 2010). One of these studies also used VEMD data and found that the majority of injuries associated with aerobics (or group exercise classes) were due to falls (Salmon et al. 2000). Assuming that the falls throughout the facility and awkward landings or twisting motions during exercise (which would likely then result in a fall) categories were combined, falls accounted for the majority of injuries associated with group exercise classes and is consistent with this VEMD study. Limitations of the VEMD aerobics study (Salmon et al. 2000) are that it was published more than 10 years ago and used only pre-coded data and so did not provide the same level of detailed cause information as in this study. Another study used both VEMD and Victorian Admitted Episodes Dataset (all hospital admissions in Victoria, Australia) data to determine the epidemiology of fitness-related injuries, provided an overview of the types and causes of such injuries (Gray and Finch 2015) and found that falls were most common during aerobics and when using other equipment; and the majority of resistance training injuries were associated with being hit or struck by weights or fellow exercisers.
A weight training study that used an American dataset similar to the VEMD found that injuries associated with free weights were more common than those associated with weight machines (Kerr et al. 2010). That study also found that crush injuries (by or between weights) was the most common, with overexertion as the second most common cause of injury. In our study, overexertion injuries were the most common; however, both were the main mechanisms of injury, which was very similar to this study. Whilst the study by Kerr et al (2010) reported injuries up to the year 2007, it used only pre-coded data, and the data is therefore less detailed than this study.
Haddon’s ten injury countermeasures is a good framework on which to base injury prevention strategies (McClure et al. 2004). Table 5 shows Haddon’s ten countermeasure strategies and how they could be used to reduce the likelihood or severity of injuries that occur in fitness facilities. This framework is used to make the recommendations for prevention outlined in Table 5 below.
Resistance/weight training injuries accounted for more than half of the presentations. Injuries associated with the use of a weight could often result from those unable to handle the amount of weight they are choosing or are required to lift (if weights were left by a previous user that required moving before the equipment could be used). Resistance/weight training activities are also technique orientated. Those who engage in such activities with incorrect technique are more vulnerable to both overexertion injuries and crush injuries, because incorrect technique can cause them to lose strength and a weight is dropped (Kerr et al. 2010, Hooper et al. 2014). Due to the nature of the activity and the equipment used, any injuries sustained during resistance/weight training activities would likely be acute and traumatic (Kerr et al. 2010), which could explain the high number of cases in our study of ED presentations. Acute, traumatic injuries are known to be more likely to require hospital treatment, rather than by allied health professionals or general practitioners (NSW Government 2014).
Injuries due to overexertion/unnatural/strenuous movements were common across many activities. This cause group included cases with narratives that mentioned ‘something gave way,’ they felt ‘something pop’ or something was strained or sprained. Injuries due to this category could be less preventable by facility design factors than other causes due to a person’s predisposition to injury (for example, body composition, tendinopathies and previous injury) (Taimela et al. 1990, Flynn et al. 2005) or if the individual was overexerting themselves or using incorrect technique (Hooper et al. 2014). It is recommended that facilities provide education regarding healthy amounts of exercise and how to perform each exercise with the correct technique. Facilities should also be supervised at all times by qualified staff to ensure members are using the correct technique, feeling supported and not engaging in dangerous behaviour (Fitness First Group 2014, American College of Sports Medicine 2012, Dietrich et al. 2014).
Injuries due to awkward landings or twisting motions may be difficult to prevent. In order to do this, fitness facilities should encourage proper footwear to ensure it provides the correct level of support and functionality (Haddon countermeasure 8), de-clutter or remove any trip hazards and, to a lesser extent, educate users to improve their technique.
Fitness facilities should provide proper storage for all loose equipment to ensure they remain tidy without equipment on the floor, which will help to prevent trips and falls throughout their facility (Haddon countermeasure 3). By appropriately highlighting changes in floor elevation (steps, ramps and edges) and providing adequate space around equipment so that others may navigate around it without interference when in use could also prevent trips and falls (Haddon countermeasures 7 and 4, respectively). Signs instructing users to wipe down equipment or the floor where sweat could cause a user to slip, as well as to put all equipment back in storage once finished, should also be displayed.
Trip and fall injuries from cardiovascular equipment could be prevented by instructing users to turn equipment off after use and ensure equipment is at a complete stop prior to getting on. Encouraging the attachment of the emergency brake cord when using particular equipment could reduce the severity of injury following a fall (such as a friction burn from a treadmill belt) (Haddon countermeasure 8).
Whilst Australia has no nationwide standards and guidelines for the fitness industry (Dietrich et al. 2014), the American College of Sports Medicine publishes and regularly updates their Health/Fitness Facility Standards and Guidelines. This book covers pre-activity screening, orientation, education, supervision, risk management and signage (American College of Sports Medicine 2012) and can be used as a good guide for Australian facilities to identify suitable strategies for removing injury causing risks and hazards.
Injury surveillance is crucial to the development of effective injury prevention strategies; however there is currently no comprehensive injury surveillance system for the fitness industry in Australia. Whilst it is possible that fitness facilities could maintain their own injury surveillance system, this data is not publically available and cannot be used to generate a cross-fitness industry profile. Therefore, the VEMD was queried as it is the only known publically available source of injuries associated with fitness facilities in Australia (Gray and Finch 2015).
A limitation of this study is that the VEMD may not be a representative sample of all fitness facility injury cases. Nevertheless, it has the potential to yield useful information about the causes of fitness-related injuries that cannot be obtained elsewhere and on a large number of cases. As the aim of this study was to identify the patterns of causes of fitness industry-related injuries, it did not matter that the coverage of the VEMD across all years varied. This study aimed to identify the main causes of injuries associated with particular fitness activities, rather than to determine the rate or frequency of injuries due to these. Case selection was based on targeted keyword searching of the 250 character narrative. Whilst every effort was made to allow for misspellings and variations (searched for ‘treadmill’ and ‘tredmill,’ for example), cases may not have been selected if a keyword was misspelt in the narrative and not accounted for during case selection. This could have possibly altered results; however, it is assumed that if any cases were not selected, it would likely have been a very small proportion of all fitness-related cases. Another limitation was that the VEMD was not set up for injury surveillance at fitness facilities nor was it set up to record the specific activity at the time of injury or the specific cause. Whilst the VEMD has its limitations, it can still provide useful information beyond the coded injury data regarding the circumstances of the injury.
Conclusions
To our knowledge, this is the first study to report the specific causes of injuries across all major fitness activities. It provides relevant information from a large case series of injuries sustained by participants of fitness activities. In doing so, it describes the most common causes of injury and this information can be used to identify suitable prevention measures. Injuries occur to participants of all fitness activities, but the pattern of injury differs across activity types. Injuries due to overexertion were the most common overall as well as the main cause of injuries related to general free weight activities and group exercise classes. Crush injuries due to falling weights were common for all free weight activities. Falls were common during group exercise classes, throughout facilities and from cardiovascular equipment. This research provides the foundation for fitness activity-related injury prevention strategies to be developed, which should be tailored according to the type of fitness activity being undertaken.
Abbreviations
- ED:
-
emergency department
- VEMD:
-
Victorian Emergency Minimum Dataset
- VISU:
-
Victorian Injury Surveillance Unit
References
Bull F, Bauman A, Bellew B, Brown W. Getting Australia active II: an update of evidence on physical activity for health. http://www.health.vic.gov.au/archive/archive2014/nphp/publications/documents/gaa_2_body_ver1.pdf (2004). Accessed 30 Aug 2012.
Fitness Australia. The Australian fitness industry report 2012. http://skillsalliance.com.au/wp-content/uploads/Australian-Fitness-Industry-Report-2012_media.pdf (2012). Accessed 14 Feb 2013.
Australian Sports Commission. Participation in exercise, recreation and sport. http://www.ausport.gov.au/information/casro/ERASS/erass_past_reports/erass_2010 (2010). Accessed 16 Aug 2014.
Physical Activity Council. 2014 Participation report. http://www.physicalactivitycouncil.com/PDFs/current.pdf (2014). Accessed 6 Nov 2014.
Andrew N, Wolfe R, Cameron P, Richardson M, Page R, Bucknill A, et al. The impact of sport and active recreation injuries on physical activity levels at 12 months post-injury. Scand J Med Sci Sports. 2014;24:377–85.
Gray SE, Finch CF. Epidemiology of hospital-treated injuries sustained by fitness participants. Res Q Exerc Sport. 2015;86:81–7.
Thompson SH, Case AJ, Sargent RG. Factors influencing performance-related injuries among group exercise instructors. WSPAJ. 2001;10:125–42.
Hayes GW. Injuries arising from aerobic fitness classes. Can Fam Physician. 1985;31:1517–20.
Quatman CE, Myer GD, Khoury J, Wall EJ, Hewett TE. Sex differences in “weightlifting” injuries presenting to united states emergency rooms. J Strength Cond Res. 2009;23:2061–7.
Salmon J, Garnham A, Finch C. In step with aerobic dance prevention – a review of the literature. Research report no. 20001. School of Health Sciences, Faculty of Health and Behavioural Sciences, Burwood: Deakin University. 2000 It is a book/report published by Deakin University (Burwood campus).
Garrick JG, Gillien DM, Whiteside P. The epidemiology of aerobic dance injuries. Am J Sports Med. 1986;14:67–72.
Jones CS, Christensen C, Young M. Weight training injury trends: a 20-year survey. Phys Sportsmed. 2000;28:61–72.
Kerr ZY, Collins CL, Comstock RD. Epidemiology of weight training-related injuries presenting to United States emergency departments, 1990 to 2007. Am J Sports Med. 2010;38:765–71.
McClure R, Stevenson M, McEvoy S. The scientific basis of injury prevention and control. Melbourne: IP Communications. 2004.
Hooper DR, Szivak TK, Comstock BA, Dunn-Lewis C, Apicella JM, Kelly NA, et al. Effects of fatigue from resistance training on barbell back squat biomechanics. J Strength Cond Res. 2014;28:1127–34.
NSW Government. Emergency departments. http://www0.health.nsw.gov.au/hospitals/going_to_hospital/emergency_departments.asp (2014). Accessed 10 Dec 2014.
Taimela S, Kujala U, Osterman K. Intrinsic risk factors and athletic injuries. Sports Med. 1990;9:205–2015.
Flynn RK, Pedersen CL, Birmingham TB, Kirkley A, Jackowski D, Fowler PJ. The familial predisposition toward tearing the anterior cruciate ligament: a case control study. Am J Sports Med. 2005;33:23–8.
Fitness First Group. Under supervision: Lack of staff and expertise in UK gyms not working out. http://www.fitnessfirst.com/news-and-pr/under-supervision-lack-of-staff-and-expertise-in-uk-gyms-not-working-out/ (2014). Accessed 10 Dec 2014.
American College of Sports Medicine. ACSM’s health/fitness facility standards and guidelines. 4th ed. Champaign: Human Kinetics; 2012.
Dietrich J, Eickhoff-Shemek J, Finch CF, Keyzer P, Norton K, Sekendiz B. The Australian fitness industry risk management manual. http://www.fitnessriskmanagement.com.au/pdf/The-Australian-Fitness-Industry-Risk-Management-Manual.pdf (2014). Accessed 10 Dec 2014.
Acknowledgements
The injury data was provided to the authors as de-identified narratives by the Victorian Injury Surveillance Unit, Monash University Research Institute which is funded by the Victorian Department of Health.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SEG was involved in the conception and design of the research, the acquisition, coding, analysis and interpretation of the data and drafting the article. CFF contributed to the conception and design of the research, interpretation of the data and critical revision of drafts. Both authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Gray, S.E., Finch, C.F. The causes of injuries sustained at fitness facilities presenting to Victorian emergency departments - identifying the main culprits. Inj. Epidemiol. 2, 6 (2015). https://doi.org/10.1186/s40621-015-0037-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40621-015-0037-4