
Abstract
Background
Obesity in children is increasing worldwide. Malnutrition has become a double burden challenge of public health concern in developing countries. Childhood obesity increases the risk of chronic disease in childhood as well as adulthood. However, information is very scarce about childhood obesity in developing countries specifically in Ethiopia. Therefore, we aimed to assess childhood overweight, obesity and associated factors among primary school children at Dire Dawa, Eastern Ethiopia.
Methods
A school based cross-sectional study was conducted in Dire Dawa from 1st to 30th March, 2016. Study participants were selected using multistage sampling method. Pre-tested self-administered questionnaire, face to face interview technique and anthropometric measurements were used to collect data by eight well trained data collectors. Data were coded, cleaned and entered into EpiData software version 3.5.1, and exported into SPSS (version 21.0) statistical software, for data analysis. Bivariate and multivariate logistic regression were carried out to identify associated factors with childhood overweight and obesity. Statistical significance was declared using Adjusted Odds Ratio (AOR) at 95% CI and p-value less than 0.05.
Results
The prevalence of overweight and obesity were 14.7% (95% CI: 11.7, 18.0) and 5.8% (95% CI: 3.6, 8.0), respectively. Children who were from private school (AOR = 3.4, 95% CI: 1.4, 8.5), from families belonged to high socioeconomic class (AOR = 16.9, 95% CI: 6.5, 23.9), preferred sweetened foods (AOR = 2.3, 95% CI: 1.1, 5.1), had not engaged in regular physical exercise (AOR = 3.8, 95% CI: 1.5, 9.8), had experienced sedentary life style like spent their free time watching TV (AOR = 3.6, 95% CI: 1.6, 7.9), play computer game (AOR = 4.6, 95% CI:1.4,15.4), and were not having close friends (AOR = 2.9, 95% CI: 1.4, 6.2) were significantly associated with overweight/obesity risk.
Conclusion
Overweight/obesity in children is on alarming stage in the study area. Therefore, more attention should be given to creating awareness about healthy diet and improving life style through school and public media in collaboration with concerned bodies.
Similar content being viewed by others


Background
A combination of obesity and overweight represents a severe public health problem. Globally, the trend of obesity prevalence and its impact has increased in the society, especially in the recent times [1, 2]. It has more than doubled worldwide since 1980. Globalization, improving economic conditions and changing dietary habits in developing countries are responsible risk factor for the rapid increase in obesity. Currently, the estimates shows that overweight in children is increasing in developing countries, and obviously high in developed countries [1, 3]. In the meantime, the intake of energy-dense foods which contain high fat, salt and sugars have been increasing. While, low intake of micronutrients and having sedentary life style have become a risk for overweight and obesity in connection with increase in urbanization [4,5,6].
On the other hand, school based health promotion approaches such as improving children’s physical activity, fruits and vegetables intake, have been found helpful to minimize risk of childhood obesity [7]. Studies have reported that about 50–80% of children who develop obesity early in life, end up becoming obese in later life [8]. Globally, obesity in childhood have been described as double burden of malnutrition which has multiple consequences, and it is known to be associated with adulthood chronic illness. It leads to morbidity such as risk of high blood pressure, diabetes mellitus, respiratory disease, dyslipidemia, tumor and orthopedic disorders [9,10,11,12,13,14,15,16,17,18,19].
Childhood under nutrition and obesity are simultaneous occurrence in many developing countries [19,20,21]. In many Sub-Saharan Africa countries, research and investment in health has been mainly focused on infectious diseases and under nutrition. In the meantime, obesity is a well-recognized risk factor for various chronic health problems, and also predictor of future adulthood health status [22,23,24]. The factors associated with overweight and obesity are mainly entrenched with health behaviors, dietary habits, daily physical activity, broader social, environmental and biological determinants [25, 26].
Though there are few studies conducted in Ethiopia, they revealed that childhood overweight and obesity are emerging and consistently increasing in magnitude particularly in private school children [27,28,29]. The fact that there is a growing demand to prevent non-communicable diseases starting at early ages. Nevertheless, information is very scarce about childhood obesity in developing countries specifically in Ethiopia. Most of the research focused on undernutrition assessment. We could not find a study done in Dire Dawa city during our literature review from September 2015 to March 2016. Therefore, this study was designed to determine the magnitude and associated factors of childhood overweight and obesity. The study will elevate the need for program planners, policy makers, parents or guardians, clinicians and all other stakeholders to give an emphasis for childhood overweight and obesity. Therefore, we aimed to assess childhood overweight, obesity and associated factors among primary school children at Dire Dawa, Eastern Ethiopia.
Methods
Study setting and study design
A school based cross-sectional study design was employed using quantitative method to assess the level of childhood overweight and obesity. The study was conducted in Dire Dawa city administration, from 1st to 30th March, 2016. Dire Dawa is one of the two Federal Administrative Cities in the Federal Democratic Republic of Ethiopia. Dire Dawa city is located about 515 km Eastern direction from Addis Ababa. At the time of the interview, a total of 38,376 school age children were living in the city. In Dire Dawa city, in-school children from 63 primary schools that had 5th to 8th grades were eligible for this study. Children who had any chronic disease, mental illness and physical disability were not included into the study.
Sample size and sampling procedure
Sample size was calculated using single population proportion formula considering proportion of overweight of ten percent in Addis Ababa primary school children [29], 95% Confidence Interval (CI) and five percent margin of error. Ten percent for non-response rate and a design effect of three were considered to obtain representative sample size. Finally, a total of 456 participants were obtained. Multistage sampling methods were used to select the study participants. Henceforward, primary schools were stratified into public and private schools in which we assumed obesity could vary across public and private schools. A total of eight primary schools; five from public and three from private were selected randomly from eligible primary schools. A total of 6,587 children were enumerated from the recruited schools. The sample size was proportionally allocated to size into public and private schools accordingly. Sampling frame was prepared based on students class room register. Then participants were selected using systematic sampling method with every ‘Kth’ interval (k = 14). Finally, 456 school going child-parent pairs were included into the study.
Data collection tools and quality control
Data were collected using both structured and semi-structured questionnaires. The questionnaire was comprised of socio-demographic characteristics, physical activity, sedentary life style factors, and dietary habits related questions. In addition, anthropometric measures (weight and height) were carried out. Most of the questionnaires were adapted, and modified to suite and relate to the study objective and area’s context. Weight was measured by using UNICEF seca digital balance scale and recorded to nearest 0.5 Kg. Children’s height was measured using portal stadiometer. Enumerators strictly followed appropriate height measuring procedures. Height was measured by placing a child in standing position that heels, buttocks, scapula/upper body parts and occiput touching the measuring board. Height measurement values were read and recorded to nearest 0.1 cm. The weight and height of the children were measured with barefoot. The children’s weight was measured using weight measurement balance in wearing only light clothing and barefoot. Children’s bags, books, exercise books and other playing materials were put away by data collectors. Body Mass index (BMI) was calculated using Microsoft Excel 2013, and applying a mathematical formula where weight in kilograms (kg) divided by height in meter square (m2). BMI-for-age percentiles for age were computed separately for male and female using Center for Disease Control (CDC) growth charts developed in 2000 [30]. To assure the quality of data, the data collectors and supervisors were trained for one day. The training addressed the sampling procedures, data collection methods, consent and assent taking, understanding the questionnaire, and purpose of the study. Meanwhile, a pretest of the instrument was carried out in one of the nearby primary school in Harar city. The anthropometric measurement tool calibrations and close supervision of data collection process were carried out. One day orientation was given to eight school teachers about the data collection procedures and instruments. The questionnaire was developed in English, and then translated into the local language (Amharic). The language review was made by experts for consistency of translation.
Data processing and analysis methods
Data were coded, manually checked and entered into EpiData software version 3.5.1, and exported into SPSS (version 21.0) statistical software. Data were cleaned by running frequency to explore the variables one by one. Data anomalies, typos and other errors were corrected by cross-checking against the originally filled hard copy questionnaire. Data were analyzed with SPSS (version 21.0) statistical software. Descriptive statistics was computed to determine the magnitude of the explanatory variables and outcome variable. Binary logistic regression was done to investigate the association between explanatory variables and outcome variable (childhood overweight and obesity). Explanatory variables such as maternal education, occupation, religion, average family income, family size, family car ownership, school type, monthly income, vigorous-sports, spend free time, sleeping habits in the afternoon, having close friends, food preferences (such as sweetened foods, fruits, vegetables, snacks, number of meals per day) were included into the binary regression. Of these, explanatory variables which had crude odds ratio at 95% CI and p-value of less than 0.2 on the bivariate analysis were included into the final multiple logistic regression model to control for confounders. Multiple logistic regression was tested for model fitness by using Hosmer-Lemshow model test. Multicollinearity of the independent variables was checked by standard error, and variables with standard error of greater than two were excluded from the multivariate analysis. Finally, adjusted odds ratio with 95% CI at p-value less than 0.05 was used to declare statistically significant association.
Results
Parental socio-demographic characteristics
A total of 448 children-parent pairs were assessed in this study. The response rate was 98.2%. The mean family monthly income was 3,014 (±1,307.9) Ethiopian Birr. Three hundred twenty (71.4%) of parents were female, and 422 (41.1%) of them attended primary education. One hundred seventy six (39.3%) of mothers were house wives by occupational status. One third (34.8%) of them had involved in private business for the last 12 months preceding this study. Almost one out of ten children’s family had their own car, which they used for transportation. Approximately three quarter (72.8%) of the parents had five and less family size (Table 1). Regarding to maternal history of gestational diabetes mellitus and family history of chronic disease, 11 (2.5%) of mothers had history of gestational diabetes mellitus, and 48 (10.7%) of parents had history of chronic diseases.
Children’s sociodemographic characteristics
Among a total of 448 children, 187 (41.7%) were male and 261 (58.3%) were female. The mean age of the children was 13.1 (±1.4) years. Regarding to children’s grade level, 115 (25.7%), 138 (30.8%), 121 (27.0%) and 74 (16.5%) of the children were 8th, 7th, 6th and 5th grades, respectively. Almost three quarter (72.5%) of children were from government schools.
Magnitudes of overweight and obesity
The overall magnitude of underweight, normal weight, overweight and obesity were 12.1, 67.4, 14.7 and 5.8%, respectively (Fig. 1). The prevalence of overweight and obesity were 14.7 and 5.8%, respectively. Meanwhile, females (16.5%) were more overweight than male children (12.3%). Nevertheless, males (8.6%) were more obese than female children (3.8%). Children attended at government (9.2%) and private schools (29.3%) were overweight. Similarly, 1.8% of government and 16.3% of private schools children had childhood obesity (Table 2).

BMI of primary school children in Dire Dawa City, Eastern Ethiopia, March, 2016 [n = 448]
Dietary habits and food preference
Regarding the dietary habits of children, 176 (39.3%) and 170 (37.9%) of them had not consumed fruits and vegetables, respectively. Of these, majority (96.0%) of them reported having food more than once per day. While more than half (54.9%) of them usually had snack. Children had a habit of buying junk food. Cake, biscuit, ice cream and chocolate were some of the common food items that were bought by children 28.1, 47.1, 17.9, and 22.3%, respectively. Approximately half of the children (49.6%) used the most favorite local foods called “Baklawa”, “Wushebek” or “Halewa”. Note that “Baklawa” or “Wushebek” or “Halewa” are local food items that made up of groundnut, plenty sugar, oil, refined wheat powder and other sweetening agents. Forty eight (10.7%) and 126 (28.1%) of them ate their food while they were watching movies and or TV programs, respectively (Table 3). Nine out of ten children (92.9%) preferred much sweetened food items which are rich in carbohydrate (sugar) (Fig. 2).

Distribution of food preferences of the primary school children in Dire Dawa City, Eastern Ethiopia, March, 2016 [n = 448]
Physical activity and sedentary lifestyle
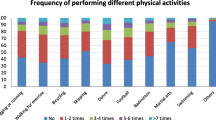
Only a quarter (25.2%) of children did some physical activities besides learning. Of these, and children engaged in vigorous 106 (93.8%), and moderate intensity 111 (98.2%) exercises for at least 10 min every day. Children spent only a few minutes for physical activities. Sixty four (34.9%), 30 (32.6%) and 12 (32.6%) of them spent their time on vigorous exercises for less than 60, 60-120 and greater than 120 min, respectively (Fig. 3).

Distribution of number of day for vigorous and moderate intensity exercises among primary school children in Dire Dawa City, Eastern Ethiopia, March 2016 [n = 448]
More than half (58.3%) of children had habits of walking on foot and also ride bicycle. Of these, more than one third (34.9%) of them had walking or riding bicycle for 1-2 days per week. Eighty three (50.9%) of the children exercised vigorous sport for 1–2 days per week, while 43.6% of them spent 60–120 min exercising. On the other hand, 55.4, 31.0 and 8.9% of children spent their free time in resting or just reading books, watching Television (TV), different videos and playing computer games, respectively (Table 4). In additional, majority of them 396 (88.4%) had no habits of taking short nap in the afternoon. While for average regular sleep duration, 5.4 72.3 and 22.3% of them slept for less than 7 hours, 7 to 8 hours and greater than or equal to nine hours per day, respectively. Only 10.3% of the children felt unhappy most of the time. Nevertheless, around half of the participants (50.9%) had close friends in school or in their neighborhoods.
Factors associated with childhood overweight and obesity
A total of thirteen explanatory variables were assessed, six of them were found to be significantly influence child overweight and obesity. Children who learn in private schools were almost three times more likely to be overweight or obese as compared to those learn in government schools (AOR = 3.4, 95% CI:1.4, 8.5). Children who preferred sweetened foods were almost two times more likely to be overweight or obese as compared to those who did not preferred sweetened foods (AOR = 2.3, 95% CI:1.04, 5.1). Children who did not perform vigorous intensity sports were about four times more likely to be overweight and obese as compared to those who did vigorous intensity sports for at least 10 min per activities (AOR = 3.8, 95% CI:1.5, 9.8). Regarding to children who spent their free time; by watching TV (AOR = 3.6, 95% CI:1.6, 7.9), and playing computer (AOR = 4.6, 95% CI:1.4, 15.4) were almost four times more likely to be overweight and obese compared to those who did not spend time in watching TV and playing computer games (Table 5).
Discussion
The findings of the present study determined the magnitude and associated factors of overweight and obesity among primary school children in Dire Dawa city administration, eastern Ethiopia. Accordingly, the overall prevalence of underweight, normal weight, overweight and obesity were 12.1, 67.4, 14.7 and 5.8%, respectively. The findings of the present study were almost consistent with another study conducted in Ethiopia (2014) which revealed that underweight, normal weight, overweight and obesity are 9.5, 77.8 9.9 and 2.8%, respectively [29]. The frequency of overweight was higher in female (16.5%) than male (12.3%) children, but males (8.6%) were more obese than females (3.8%). The present study findings support findings reported in India which was conducted from 2007 to 2010 [31], and in Ethiopia [4]. Congruence in findings could be explained by similarity in the culture of Indian and Ethiopian societies in which females spent most of their time at home and more boys’ participate in field activities.
The finding of the present study was lower in magnitude of overweight and obesity compared to a study done in Australia [32]. Moreover, the finding of this study was also lower than studies done from 2008-2010 in United Arab Emirates and Bangladesh [20, 33] and in other African countries like in Egypt, South Africa and Kenya, but nearly similar with report from Cameron [3, 5, 34, 35]. This might be explained by the difference in feeding habits and socio-economic status and difference in standard for the cutoff point and sample size of participants. Regarding to school type; government and private schools, the level of childhood overweight and obesity in the present findings were consistent with studies in Kenya and Ethiopia (2014) [4, 23]. Majority of children preferred animal product, food rich in carbohydrate and sweets foods. However, the present findings are more comparable with studies done in Pernambuco (2011), Brazil (2015) and Kenya (2012) [35,36,37]. Conversely, the study done in Ethiopia (2015) revealed that (90%) preferred animal products, (88.6%) preferred rich foods in carbohydrate, and (17.7%) preferred sweetened foods, which was similar to the findings reported in the current study, even though higher preference of sweetened food were found in this study. This higher sweetened food preference might be due to culture of eating locally available sweetened foods in the community.
According to this study, children from private school were three times more likely to be overweight or obese compared to government schools children. The present study finding is consistent with studies in different countries from 2011 to 2015, in Brazil [37], India [38], Kenya [23], Ghana [16], and Ethiopia and [4, 28, 29]. This study also found that children from parental average monthly income above the mean were almost 17 times more likely to be overweight or obese compared to those family who had average monthly income below the mean score. The present study finding is consistent with studies done in China [39], Bangladesh [15], Romania [40], Brazil [15] and Egypt 2013 [5]. Similarly, the study findings also revealed, children, learning in private schools and belonging to parents with high socioeconomic status were strongly associated with overweight and obesity. One possible explanation might be, their higher socioeconomic status of private school children would allow them for higher adoption of unhealthy nutritional habits (fast foods, energy-dense snacks, sweetened foods, more animal products, etc) than other school children.
Likewise children who preferred sweetened foods were more likely to be overweight or obese compared to those who did not prefer sweetened foods. This was similar with different studies done in Europe as reported from a study conducted by World Health Organization (WHO) [41], India [42], Egypt [5], Tamale metropolis of Ghana [16], Kenya [35], and Ethiopia [28, 29] which revealed that sweetened foods preference were found significantly associating with overweight and obesity. This could be explained as sweetened food items are calorie dense foods which result in positive energy balance to their consumers. As per the findings from this study, children who had sleeping habit in the afternoon were 2.5 times more likely overweight and obese than children who did not sleep in the afternoon. Children who had no close friends in school or around their neighborhoods were almost three times more likely to be overweight and obese compared to those who had close friends. This was consistent with studies done in China [39], Ghana and Uganda [22]. In contrary to the findings of this study, a study conducted in China [43] revealed that short sleep duration and sleeping in the afternoon was not associated with obesity. This discrepancy might be due to difference in sleeping habits and age of the participants.
This study revealed that children who spent their free time by watching TV and playing computer were about four times more likely to be overweight and obese compared to those who spent their time reading. This finding confirms the findings from studies conducted in Brazil [44], Germany [45], Ghana [16], and Ghana and Uganda [22] that revealed children who spent their free time in viewing TV, play computer game for three and more hours were more likely to be overweight and obese. This might be explained by advancement in technology which has tremendously changed the life style of children. Watching TV and playing computer game may decrease the amount of time spent on playing outdoor games which might resulted in weight gain.
Likewise this study, revealed that children who did not perform vigorous intensity sports were about four times more likely to be overweight and obese compared to those who did vigorous intensity sports for at least ten minutes. This was similar with study done in Brazil [44], Ghana [16], Ghana and Uganda [22]. Several other studies conducted in Ghana [46], Egypt [5] and Ethiopia [4] found that vigorous intensity sports reduced risk of overweight and obesity. But other studies in Lithuania [47] and Romania [40] reported that any physical activities were not associate with reduction of the risk of increased overweight. This could be explained as physical activity results in energy expenditure thereby decreasing adiposity in the body.
Strength and limitation of the study
This study used a probability sampling procedure to select study participants. We used questionnaire method and anthropometric measurement (height and weight) to assess the level of obesity. Since the study was cross-sectional, it was not possible to strongly to demonstrate cause and effect relationship. It used self-reporting (interview response) which might have social desirability bias. Some questions also required the participants to recall, which could have affected the results as most of them, could have forgotten.
Conclusion
Both under nutrition and over nutrition coexist among primary schools children in Dire Dawa city. This study revealed that one in seven children were overweight. Approximately one in twenty children had obesity. The prevalence of overweight and obesity problem is slightly higher among girls than boys. Learning in private school, high parental socioeconomic class, sweet foods preference, physical inactivity or not engaging in sport exercise, sedentary life style like spent free time in viewing TV and play computer game, sleeping habit in afternoon and not having close friends were significantly associated with childhood overweight and obesity. We suggest integrated nutrition program should be implemented at school, and in the community with existing community based health extension program. Nutritional behavioral change communication should be delivered to parents and in school for children.
Abbreviations
- AOR:
-
Adjusted Odds Ratio
- BMI:
-
Body Mass Index
- CDC:
-
Center for Disease Control
- CI:
-
Confidence Interval
- COR:
-
Crude Odds Ratio
- SPSS:
-
Statistical Packages for Social Sciences
- TV:
-
Television
- UNICEF:
-
United Nations Children’s Fund
- WHO:
-
World Health Organization
References
WHO. World Health Organization; Obesity and overweight fact sheet N°311. 2015. Available from: https://apps.who.int/medial centre/factsheets/fs311/en/ on Nov 18, 2015.
Gee S, Chin D, Ackerson L, Woo D, Howell A. Prevalence of childhood and adolescent overweight and obesity from 2003-2010 in an integrated health care delivery system. J Obes. 2013;417907:1–8.
Pienaar AE. Prevalence of overweight and obesity among primary school children in developing country: Child longitudinal data of 6–9 years old children in South Africa. BMC Obes. 2015;2(2):2–10.
Alemu E, Atnafu A, Yitayal M, Yimam K. Prevalence of overweight and or obesity and associated factors among high school adolescents in arada Sub-city, Addis Ababa, Ethiopia. Nutr Food Sci. 2014;4(2):10–4.
Badawi NE, Barakat AA, Awad S, Sherbini E. Prevalence of overweight and obesity in primary school children in port said city. Egyp Paediatr Assoc. 2013;61(1):31–6.
Karnik S, Kanekar A. Childhood obesity: a global public health crisis. Int J Prev Med. 2012;3(1):1–7.
Langford R, Bonell C, Jones H, Campbell R. Obesity prevention and the health promoting schools framework: essential components and barriers to success. Int J Behav Nutr Phys Act. 2015;12(15):1–17.
Story M, Kaphingst Karen M, French S. The role of child care settings in obesity prevention. Future Child. 2006;16(1):143–68.
Sheila G. In: Dick’s REB, editor. Nelson Textbook of Pediatrics. Overweight and Obesity. Body Mass Index. Nineteenthth ed. Wisconsin: Saunders, an imprint of Elsevier; 2011.
Manyanga T, El-sayed H, Doku DT, Randall JR. The prevalence of underweight, overweight, obesity and associated risk factors among school-going adolescents in seven African countries. BMC Public Health. 2014;14:887.
Wong CY, Zalilah MS, Chua EY, Norhasmah S, Chin YS, Asyura ASN. Double-burden of malnutrition among the indigenous peoples (orang asli) of peninsular Malaysia. BMC Public Health. 2015;15:680.
Pelegrini A, Diego Augusto D, Silva S, Luiz E, Petroski A. Overweight and obesity in seven to nine-year-old Brazilian children: data from the Brazilian sports project. Rev Paul Pediatr. 2010;28(3):290–5.
Gele A, Mbalilaki AJ. Overweight and obesity among African immigrants in Oslo. BMC Res Notes. 2013;6:119.
Lazzeri G, Giacchi MV, Spinelli A, Pammolli A, Dalmasso P, Nardone P, et al. Overweight among children aged 11–15 years and its relationship with breakfast, area of residence and parents’ education: results from the Italian HBSC 2010. A cross-sectional study. Nutr J. 2014;13(69):1–10.
Souza MCC, Tibúrcio JD, Bicalho JMF, Rennó HMS, Dutra JS, Campos LG, Silva ES. Factors associated with obesity and overweight in school-aged children. Florianópolis: Text Context Nursing. 2014;23(3):712–19. http://dx.doi.org/10.1590/0104-07072014001740013.
Amidu N, Owiredu M, Saaka L, Quaye M, Wanwan PD, Kumibea FMZ. Determinants of childhood obesity among basic school children aged 6–12 years in Tamale Metropolis. J Med Biomed Sci. 2013;2(3):26–34.
Rathnayake KM, Satchithananthan A, Mahamithawa S, Jayawardena R. Early life predictors of preschool overweight and obesity: a case-control study in Sri Lanka. BMC Public Health. 2013;13:1.
Niehues JR, Gonzales AI, Lemos RR, Bezerra PP, Haas P. Prevalence of overweight and obesity in children and adolescents from the age range of 2 to 19 years old in Brazil. Int J Pediatr. 2014;583207:1–7.
Wamba PCF, Enyong Oben J, Cianflone K. Prevalence of overweight, obesity, and thinness in cameroon urban children and adolescents. J Obes. 2013;737592:1–9.
Shuhana S, Mc Tigue KM, GJ and PB. Prevalence and risk factor of childhood overweight and obesity in primary school children. Ann Intern Med. 2010;136:857–64.
Tathiah N, Moodley I, Mubaiwa V, Denny L, Taylor M. South Africa’s nutritional transition; overweight, obesity, underweight and stunting in female primary school learners in rural KwaZulu-Natal, south Africa. S Afr Med J. 2013;103(10):718–23.
Peltzer K, Pengpid S. Overweight and obesity and associated factors among school-aged adolescents in Ghana and Uganda. Int J Environ Res Public Health. 2011;8:3859–70.
Kyallo F, Makokha A, Mwangi AM. Overweight and obesity among public and private primary school children in Nairobi, Kenya. Health (Irvine Calif). 2013;5(8):85–90.
Ziraba AK, Fotso JC, Ochako R. Overweight and obesity in urban Africa: a problem of the rich or the poor? BMC Public Health. 2009;9:465.
Roberts KC, Shields M, De Groh M, Aziz A, Gilbert JA. Overweight and obesity in children and adolescents: results from the 2009-2011 Canadian health measures survey. Heal Rep. 2012;23(3):3–7.
Vohra R, Bhardwaj P, Srivastava JP, Srivastava S, Vohra A. Overweight and obesity among school going children of Lucknow city. J Fam Commun Med. 2011;18(2):59–62.
Tesfalem T, Singh PDM. Prevalence and associated factors of overweight and obesity among high school adolescent in urban communities of Hawassa city. Curr Res Nutr Food Sci. 2013;1(1):23–36.
Gebregergs GB, Melkie Endris Yesuf TKB. Obesity and weight loss therapy overweight, obesity and associated factors among high school. J Obes Weight Loss. 2013;3(165):2–6.
Gebremichael B, Chere A. Prevalence of childhood overweight and obesity and its determinants among primary school children in Addis Ababa, Ethiopia: a cross-sectional study. J Nutr Disord Ther. 2015;5:168.
CDC. Centers for Diseases Control and Prevention. Children BMI. 2015. Available at; http://www.cdc.gov/nccdphp/dnpa/bmi/childrens,BMI.htm; Accessed on 4 Dec 2015
Unnithan AG, Syamakumar S. Prevalence of overweight, obesity and underweight among school going children in rural and urban areas of thiruvananthapuram educational district, Kerala state (India). Int J Nutr Wellness. 2007;6(2):1–6.
Schultz R. Prevalences of overweight and obesity among children in remote Aboriginal communities in central Australia. Int Electron J Remote Heal Res Educ Pract Policy. 2012;12(1872):1–7.
Al-Shamsi R, Jackson RT, Lei D, Mehta M, Cheng W-H. The Prevalence and Selected Determinants of Overweight and Obseity among Children and Adolescent in the City of AL-AIN, UAE. 2008;55–56. Dissertation. http://drum.lib.umd.edu/bitstream/handle/1903/7856/umi-umd-5174.pdf;sequence=1.
Navti LK, Ferrari U, Tange E, Parhofer KG, Pozza SB. Height-obesity relationship in school children in Sub-Saharan Africa: results of a cross-sectional study in Cameroon. BMC Res Notes. 2015;8:98.
Jain G, Bharadwaj SK, Joglekar AR. Prevalence of overweight and obesity among school children (13-17 years) in relation to their socioeconomic status and eating habits. Int J Sci Res Publ. 2012;2(6):2–3.
Geremia R, Maria H, Cimadon S, De Souza WB, Pellanda LC. Childhood overweight and obesity in a region of Italian immigration in southern brazil: a cross-sectional study. Ital J Pediatr. 2015;41(28):4–11.
Balaban G, Silva GAP. Overweight and obesity prevalence in children and adolescents from a private school in Recife state of Pernambuco. J Pediatr (Rio J). 2011;77(2):96–100.
Sonya J, Ranjani H, Priya M, Ranjit U. Prevalence of overweight and obesity among school children and adolescents in Chennai. Indian Pediatr. 2014;51(2):543–9.
Guo X, Zheng L, Li Y, Yu S, Sun G, Yang H, et al. Differences in lifestyle behaviors, dietary habits, and familial factors among normal-weight, overweight, and obese Chinese children and adolescents. Int J Behav Nutr Phys Act. 2012;9(120):1–9.
Mocanu V. Prevalence of overweight and obesity in urban primaryschool children in northeastern Romania: its relationship with socioeconomic status and associated dietary and lifestyle factors. Biomed Res Int. 2013;537451:7.
Börnhorst C, Wijnhoven TMA, Kune M, Yngve A, Rito AI, Lissner L. WHO European Childhood Obesity Surveillance Initiative: associations between sleep duration, screen time and food consumption frequencies. 2015;15(442):1–11.
Gohel MC, Raval PB, Patel SS. Prevalence of overweight and obesity in Indian adolescent school going children: its relationship with socioeconomic status and associated lifestyle factors. JAPI. 2010;58:151–8.
Cao M, Zhu Y, He B, Yang W, Chen Y, Ma J, et al. Association between sleep duration and obesity is age and gender dependent in Chinese urban children aged 6–18 years: a cross-sectional study. BMC Public Health. 2015;15:1029.
Neto FA, Eto FN, Sabrina T, Pereira S, Carletti L, Bisi C. Active and sedentary behaviours in children aged 7-10 years old: the urban and rural contexts, Brazil. BMC Public Health. 2014;14:1174.
Beyerlein A, Toschke AM, Rosario AS, Kries RV. Risk factors for obesity: further evidence for stronger effects on overweight children and adolescents compared to normal-weight subjects. PLoS One. 2011;6(1), e15739.
Mogre V, Gaa PK, Nagumsi R, Abukari S. Overweight, obesity, thinness and associated factors among school-children aged (5-14 years) in tamale. Eur Sci J. 2013;9(20):160–75.
Smetanina N, Albaviciute E, Babinska V, Karinauskiene L, Albertsson-wikland K. Prevalence of overweight/obesity in relation to dietary habits and lifestyle among 7–17 years old children and adolescents in Lithuania. BMC Public Health. 2015;15:1001.
Acknowledgment
Would like to thank Addis Ababa University for financial support. We would also like to extend our gratitude to Dire Dawa city Administration Health and Education Bureaus, School Directors and unit leaders for their assistance and cooperativeness. Our gratitude goes to data collectors and study participants for their cooperation. Last but not the least, we would like to thank Mr. Isaac Fwemba and Mr. Gezahegn Tesfaye for their wonderful help by reviewing the English language and scientific content of the manuscript.
Funding
The study was funded by Addis Ababa University, College of Health Sciences, School of Graduate Studies program, Addis Ababa, Ethiopia
Availability of data and materials
Data will be made available upon consortium approval.
Authors’ contributions
AD had substantial contribution to conception and acquisition of data of this research. AD, AM, and AS had substantial contribution to the design, analysis data and interpretation of the findings. All authors revised the paper critically for important intellectual contents. All authors read and approved the final manuscript.
Competing interests
All authors declared that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Ethical approval was obtained from Addis Ababa University, College of Health Science Institutional Research Ethics Review Board. Letters of cooperation were presented at all levels of the respective administrative officials. Informed written consent was obtained from the parents or guardians of study participants. The objective of the study was clearly explained to the study participants, teachers and parents/guardians prior to taking their consent. Informed verbal assent was also obtained from children. All information obtained from the study participants were kept private and confidential anonymously.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Desalew, A., Mandesh, A. & Semahegn, A. Childhood overweight, obesity and associated factors among primary school children in dire dawa, eastern Ethiopia; a cross-sectional study. BMC Obes 4, 20 (2017). https://doi.org/10.1186/s40608-017-0156-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40608-017-0156-2