
Abstract
Background
Obesity in infertile women increases the costs of fertility treatments, reduces their effectiveness and increases significantly the risks of many complications of pregnancy and for the newborn. Studies suggest that even a modest loss of 5–10 % of body weight can restore ovulation. However, there are gaps in knowledge regarding the benefits and cost-effectiveness of a lifestyle modification program targeting obese infertile women and integrated into the fertility clinics. This study will evaluate clinical outcomes and costs of a transferable interdisciplinary lifestyle intervention, before and during pregnancy, in obese infertile women. We hypothesize that the intervention will: 1) improve fertility, efficacy of fertility treatments, and health of mothers and their children; and 2) reduce the cost per live birth, including costs of fertility treatments and pregnancy outcomes.
Methods/Design
Obese infertile women (age: 18–40 years; BMI ≥30 kg/m2 or ≥27 kg/m2 with polycystic ovary syndrome) will be randomised to either a lifestyle intervention followed by standard fertility treatments after 6 months if no conception has been achieved (intervention group) or standard fertility treatments only (control group). The intervention and/or follow-up will last for a maximum of 18 months or up to the end of pregnancy. Evaluation visits will be planned every 6 months where different outcome measures will be assessed. The primary outcome will be live-birth rates at 18 months. The secondary outcomes will be sub-divided into four categories: lifestyle and anthropometric, fertility, pregnancy complications, and neonatal outcomes. Outcomes and costs will be also compared to similar women seen in three fertility clinics across Canada. Qualitative data will also be collected from both professionals and obese infertile women.
Discussion
This study will generate new knowledge about the implementation, impacts and costs of a lifestyle management program in obese infertile women. This information will be relevant for decision-makers and health care professionals, and should be generalizable to North American fertility clinics.
Trial registration
ClinicalTrials.gov NCT01483612. Registered 25 November 2011.
Similar content being viewed by others


Background
Obesity and fertility
Infertility affects approximately 10–15 % of couples [1]. One of the leading causes in women is anovulation caused by the polycystic ovary syndrome (PCOS) [2, 3], which affects 6–10 % of women of childbearing age [4]. PCOS accounts for more than 70 % of anovulatory infertility in women [5]. This syndrome is defined by hyperandrogenism and anovulation/polycystic ovaries [3], and its etiology is related to elevated insulin resistance and obesity in genetically predisposed women [6–9]. Accordingly, 50–75 % of women with PCOS are obese in North America [10]. Obesity increases the risk of PCOS, but it has also been associated with reduced fertility even in ovulatory women [11–13]. As of 2008, 44 % of Canadian women of reproductive age (20 to 44 years) were reported as being overweight (body mass index (BMI) 25.0 to 29.9 kg/m2, 25 %) or obese (BMI ≥30.0 kg/m2, 19 %) [14]. Also, a survey in Scotland found a significantly higher proportion of obesity in infertile women [15].
Obesity increases the costs of fertility treatments and reduces their effectiveness. Indeed, pharmacological induction of ovulation is less effective in obese PCOS women [16], with the ovulatory dose of clomiphene being positively correlated with BMI [17]. Obesity delays time to conception when using intrauterine donor insemination [18] and reduces conception following assisted reproductive technologies (ART) [19], with higher required doses of gonadotropins [20], lower implantation and pregnancy rates [20–22], and higher miscarriage rates [20–23]. In addition to fertility disorders, obesity increases significantly the risks of many complications of pregnancy, such as gestational diabetes, pre-eclampsia, caesarean section, intrauterine death, which are further increased in morbidly obese women [24–26]. During the postpartum period, overweight mothers are more likely to have hypertension and thromboembolism, leading to a higher risk of maternal mortality [27]. Obesity has also been associated with an increased risk of birth defects, such as ventral wall, neural tube, cardiac and multiple congenital defects [28]. Pregnancy and delivery procedures in obese women are therefore more costly, mainly because of increased caesarean section rates, length of hospital stay and admission to neonatal intensive care [29–31]. It was estimated that the overall costs of fertility treatments and pregnancy complications were increased by 44–54 % and 70–100 % in overweight and obese women, respectively, compared to their normal weight counterparts [32]. Moreover, offspring from obese women are more likely to develop obesity, type 2 diabetes (DM2) and cardiovascular diseases in their lifetime, often at a younger age [33]. Studies suggest that maternal obesity, via a pro-inflammatory milieu, insulin resistance, or other hormonal factors [33, 34], modify the in utero environment and might induce fetal epigenetic programming [35] which predisposes to the development of obesity and DM2 early in life, thus perpetuating the vicious circle of obesity and its comorbidities in subsequent generations.
Obesity management in women seeking fertility treatment
Collectively these substantive maternal and fetal risks call for women to lose weight prior to assisted conception in order to improve their fertility and chance of a healthy pregnancy [22, 36]. Indeed, it has been shown that a supervised lifestyle modification program, including support in addition to diet and exercise advice, can reduce weight, increase ovulatory frequency and improve pregnancy rates [37–39]. Even a modest weight loss of 5–10 % of total body weight can restore ovulation [40, 41]. The Fertility Fitness Program founded by Dr Norman in Australia is a 6-month program of weekly group sessions targeting behavioural changes that include exercise and diet. Clark et al. [39] found that in overweight, infertile, anovulatory women, this program resulted in an average weight loss of 6.3 kg, a restoration of ovulation in 12 of the 13 subjects and pregnancy in 11 women. In a follow-up study, 67 anovulatory obese women who completed the program lost an average of 10.2 kg with 90 % of them resuming spontaneous ovulation [38]. Of these participants, 78 % achieved a pregnancy and 67 % a live birth [38]. Recently, a randomized controlled trial (RCT) was completed in Australia with 171 obese infertile women and demonstrated that the program induced greater weight loss than the control intervention (4.7 vs. 1.3 kg, P < 0.001) and increased pregnancy rates at 18 months from 21 to 61 % (P < 0.001) (Clark et al., unpublished).
A study conducted by our group shows that it is possible for obese women with PCOS to achieve clinically significant and sustained weight loss by following simple advice given in a regular clinical care setting [42]. We retrospectively reviewed weight changes of young obese PCOS women and found that 43 % of 74 women lost ≥5 % of their initial weight after 6–12 months of follow-up. Young obese PCOS women seem to be a responsive population to lifestyle modification and it is thus expected that an integrated interdisciplinary lifestyle program will be even more effective in a similarly young population of obese women who are also highly motivated by their desire for a healthy baby.
Effective and acceptable lifestyle-modification strategies have the highest potential to result in a reduction in the socioeconomic burden of the obese pregnant woman. Indeed, the American Society for Reproductive Medicine [43], the American Dietetic Association [44], the American Society for Nutrition [44], the European Society of Human Reproduction and Embryology [45] and the British Fertility Society [46] have recommended that overweight/obese women should be provided with assistance to lose weight prior to conception and maintain a healthy lifestyle to prevent excess weight gain during pregnancy. The “Canadian clinical practice guidelines on the management and prevention of obesity in adults and children” emphasizes the importance of the multidisciplinary health care team for effective weight management [47]. After assessment of co-morbidities and readiness to change, a lifestyle modification program is proposed as the first step with an objective of 5–10 % weight loss. Our group implemented an interdisciplinary approach to obesity management at the Centre hospitalier universitaire de Sherbrooke (CHUS) since 2001. We have demonstrated in the general obese population that this low-cost approach leads to clinically significant weight loss [48–50]. However, access to our specialized programs is limited by a long waiting list with prohibitive delays for obese women seeking fertility treatment. They require rapid access to a lifestyle program tailored to their specific needs. At this time, there is no integrated lifestyle modification program targeting this specific population in the North American public health care systems. There are gaps in knowledge regarding the benefits and cost-effectiveness of such intervention in the North American context that our study will address. The development of a new initiative aiming at increasing efficiency and reducing the costs of fertility treatments, while improving the health of mothers and their offspring is needed.
Hypothesis
We hypothesize that an interdisciplinary lifestyle intervention taking place before and during pregnancy in obese infertile women will: 1) improve fertility, efficacy of fertility treatments, and health of mothers and their children; and 2) reduce the cost per live birth and costs of fertility treatments and rates of adverse pregnancy outcomes. We further propose that our research program will 3) result in generalizable and transferable new knowledge useful for decision-makers of the health care system.
Study objectives
This study protocol aims to design, implement and evaluate a transferable cost-effective program for lifestyle management of obesity in infertile women integrated into the fertility clinics. To achieve this goal, the proposed project will focus on four specific objectives:
-
1)
To design and implement an interdisciplinary program for lifestyle management of obese women, or overweight women with PCOS, who seek fertility treatment at the CHUS, a fertility clinic with provincial coverage of fertility treatments and satellite access to in vitro fertilization (IVF);
-
2)
To evaluate lifestyle benefits of this program and assess its impact on fertility, pregnancy complications and neonatal outcomes, as compared to a randomly assigned control group and to similar women seen in three fertility clinics across Canada with and without public coverage of fertility treatments;
-
3)
To assess cost per live birth, and other measures of cost-effectiveness, of this program compared to the control group and three fertility clinics across Canada with and without public coverage of fertility treatments; and
-
4)
To effectively transfer knowledge obtained through these activities to relevant stakeholders in the health care and public health sectors, including policy-makers, decision-makers, health care professionals and patients.
Methods/Design
Study design and setting
The proposed study relies on a participatory research approach which will combine quantitative and qualitative assessments. The impacts of the lifestyle program that will be developed will be assessed using a randomized controlled trial in one academic center. The study was registered to ClinicalTrials.gov (NCT01483612).
The RCT will be conducted at the CHUS fertility clinic, a fertility clinic with satellite access to IVF. The clinic offers care to patients with a range of reproductive problems including infertility, recurrent pregnancy loss, anovulation, PCOS, hyperprolactinemia, endometriosis, etc. The clinic has a successful ovulation induction and superovulation program including intrauterine insemination and access to donor sperm. Since 2011, it offers an IVF program in collaboration with Procrea Cliniques initially, and subsequently with the assisted reproduction center of the CHU Ste-Justine, where only the egg retrievals and embryo transfers are performed (evaluation of patients, protocol prescription, monitoring and decision making before and during cycles is done in Sherbrooke). Clinical outcomes and costs will be compared to a randomly assigned control group and to similar women seen in three fertility clinics across Canada not offering specific weight loss interdisciplinary lifestyle program: 1) an intra-provincial clinic (Procrea Cliniques, Montreal) with public coverage of fertility treatments; 2) 2 extra-provincial clinics (Centre for Fertility and Reproductive Health and IVF Unit at Mount Sinai Hospital, Toronto; and Fertility Clinic of Royal Alexandra Hospital, Edmonton) without public coverage of fertility treatments. These centers offer the full range of ART on site.
Study participants
Study participants will be recruited among all women consulting at the CHUS fertility clinic. The staff will assist the research team in identifying potential participants. To be included in the study, women must fulfill the following inclusion criteria: 1) infertility; 2) aged between 18 and 40 years; and 3) obesity (BMI ≥30 kg/m2) or overweight if PCOS (BMI ≥27 kg/m2). Women will be excluded if they had bariatric surgery or plan for it and/or if natural conception is impossible or highly unlikely (tubal factor, severe male factor infertility, etc.). Infertility will be defined as: 1) failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse in women who are under 35 years with regular menstrual cycles; 2) women who do not have regular menstrual cycles, or are older than 35 years and have not conceived during a 6-month trial period; or 3) women with a known cause of infertility. Eligible patients will be referred to the research coordinator to obtain their individual informed consent prior to baseline data collection.
Ethical considerations
The proposed research was reviewed and approved by the Institutional Research Ethics Review Boards of the CHUS and other fertility clinics. Both research participants and health professionals will be duly informed and consent will be obtained in writing prior to evaluations or focus groups. This includes the 20 patients who will be randomly selected from other Canadian fertility clinics to be evaluated at the end of the study using the same questionnaires and focus group as patients at the CHUS. The main ethical consideration of the proposed research is confidentiality issues that will be minimized. All data will be coded, archived for at least 5 years and then destroyed.
Randomisation
An independent statistician will use computerised random number generation to allocate each participant to the intervention or control group. Randomisation will be stratified according to the PCOS or non-PCOS status, based on clinical diagnosis in the patient’s record. Sequences will be generated using permuted block randomisation, with block sizes of two, four or six entries. The allocation sequence will be concealed in corresponding sequentially numbered opaque envelopes. After a participant has completed baseline assessments, the research coordinator will open the envelope to reveal the group allocation to the participant. Participants will be informed of their group assignment at that time.
Intervention
Control arm
Participants assigned to the control group will receive standard fertility treatments, which will be initiated as soon as clinically indicated. Standard fertility treatments may include lifestyle counselling by the obstetrician-gynecologist certified in gynecologic reproductive endocrinology and infertility (GREI), reproductive endocrinologist or fertility specialist in charge of the care of the patient.
Intervention arm
Participants allocated to the intervention group will be invited to participate in the interdisciplinary lifestyle intervention and will have to delay other fertility treatments for six months. After 6 months of lifestyle intervention alone, women who are not pregnant will begin pharmacologic fertility treatments, as indicated, in conjunction with the lifestyle intervention that will continue to be offered. The aim of the intervention will be to implement progressive and sustainable lifestyle changes in order to reach a modest weight loss. Women will be invited to individually meet with a dietitian and a kinesiologist (20–30 min each) at 0, 3, 6 weeks and then every 6 weeks over a period of 18 months or until the end of pregnancy. A follow-up phone call/email will also take place once between each meeting for additional support. The dietitian will use 3-day food records to evaluate the women’s food intake throughout the program. To help improve patient’s diet, Canada’s Food Guide and the “Healthy Plate” [51] will be the main tools use for nutritional counselling. The kinesiologist will be responsible for taking anthropometric measures and vital signs and for coaching women to increase their physical activity level. A pedometer will be offered to assist the patient. Patients will be guided by the dietitian and the kinesiologist to formulate S.M.A.R.T goals (specific, measurable, attainable, realistic, and timely) at each meeting. The members of our interdisciplinary team will be trained in motivational interviewing. This training can positively affect the attitude to behaviour change in obese infertile women [52].
Besides individual intervention, women will benefit from a series of 12 educational group sessions (45-minute interactive small group workshops and 45-minute physical activity) covering various topics relevant to obesity management and fertility (Table 1). The workshops will be conducted by either the dietitian or psychologist and the demonstration of physical activity will be performed by the kinesiologist. These group sessions will take place weekly. When a pregnancy is confirmed, the woman will be met to set new objectives specific to her pregnancy, including an optimal gestational weight gain based on Institute of Medicine guidelines [53]. Partners will be invited to join individual meetings and strongly encouraged to assist all group sessions. To our knowledge, this is the first study assessing a lifestyle intervention in obese infertile women that is continued during fertility treatments and pregnancy.
Committees overseeing the study
To facilitate the inclusion of all relevant stakeholders, four committees will be involved throughout program development and implementation, as well as the evaluation process.
Steering committee
This committee will bring together relevant medical experts of various disciplines (endocrinology, obesity, GREI) and health care decision-makers from the CHUS. It will be responsible for supervising the development of the intervention, the planning of the evaluation, and the monitoring of the intervention implementation at the CHUS. It will overlook the work of all subcommittees and the course of implementation, with difficulties and proposed solutions, and will decide the directions for the intervention and the research plan. Steering committee meetings will occur regularly, as needed, and will also serve as knowledge transfer activities where decision-makers and knowledge users will be informed about the implementation and the results of the research.
Advisory committee
This committee will gather experts and decision-makers, who actively collaborate to this research project but are external to our institution, especially colleagues at the three fertility clinics of comparison. This committee will advise the research team on design of the intervention and planning of the evaluation, including evaluations on their sites. The Advisory committee will meet as needed and will be actively involved in revising documents and through informal communications. Post-intervention meetings will also serve as knowledge transfer activities.
Intervention sub-committee
This sub-committee will be in charge of developing the intervention in all its details and to follow-up closely on its implementation. This sub-committee will meet every month before the project begins and then as needed until the end of the intervention.
Evaluation sub-committee
This sub-committee will develop all the evaluation tools and will plan the qualitative evaluations. It will be particularly active before the start of the intervention and at the end of the intervention for the qualitative evaluations on all sites.
Development & implementation of the lifestyle program for obese infertile women (Objective 1)
The Intervention sub-committee will be directly in charge of defining the intervention and planning the implementation. A complete review of the relevant literature will be performed initially and made available to all other committee members. The implementation of the program will be closely monitored by this sub-committee with evaluation of required human, material and other resources; barriers that will be encountered; potential solutions that will be applied; and discussion of difficult cases managed in the program. In addition, a specific qualitative evaluation of the program implementation will take place at the end of the intervention and will be planned by the Evaluation sub-committee. All women included in the CHUS RCT will be evaluated by questionnaires and a sub-group of 20 of these patients will be selected to participate in focus groups. In order to compare health professionals’ and patients’ satisfaction, perceptions and impact of the program on their life to those during usual care in Canada, we recruited three Canadian fertility clinics with different characteristics. In these clinics, 20 patients randomly selected will be evaluated at the end of the study using the same questionnaires and focus group methods. In all four centers, health care providers involved in the fertility clinic and/or the program will also be evaluated by questionnaires and focus groups.
This objective will be under the supervision of our Steering committee and Advisory committee.
Decision-makers from Quebec and Canada who sit on these committees will ensure that our program meets their objectives and is acceptable in terms of required resources and costs. Furthermore, we will validate our program design and evaluation plan with worldwide key experts as well as Canadian obesity experts contacted through the Canadian Obesity Network (CON). We will benefit from the experience of experts involved in the implementation and evaluation of similar programs: the Fertility Fitness program in Australia and the Lausanne Obesity-Fertility clinic in Switzerland.
Evaluation of clinical outcomes of the lifestyle program for obese infertile women (Objective 2)
The primary outcome will be live-birth rates at 18 months. Secondary outcomes will be sub-divided into four categories of clinical outcomes:
-
1)
Lifestyle and anthropometric outcomes: evolution of anthropometric measures, changes in lifestyle habits (diet, exercise, sleep, alcohol, and tobacco), physical fitness level, daily energy expenditure from physical activities, time spent in various physical activity intensities, step count, evolution of readiness for change, quality of life.
-
2)
Fertility outcomes: pregnancy rate (biochemical pregnancy confirmed by a positive beta-human chorionic gonadotropin (β-hCG) level in the serum), spontaneous abortions, multiple pregnancies, spontaneous vs. ART-induced pregnancy, doses of fertility medications, number of treatment or IVF cycles.
-
3)
Pregnancy adverse outcomes: gestational diabetes, hypertension, pre-eclampsia, thromboembolism, caesarean section.
-
4)
Neonatal outcomes: birth weight, hypoglycemic episodes, Apgar score, jaundice, admission to neonatal intensive care, congenital defects, intrauterine death.
The results obtained at the CHUS will also be compared to those of women with the same criteria who will be seen in three fertility clinics across Canada. At the CHUS, primary and secondary outcomes will be determined using patients’ assessments, questionnaires and review of patients’ records. At the comparative clinics, charts of patients seen during the same time period will be retrospectively reviewed, and administrative data will be gathered.
Cost-effectiveness assessment of the lifestyle program for obese infertile women (Objective 3)
Data collected for this objective will trace the operating costs (human and material resources) for each of the patients in the study based on two viewpoints: 1) the costs for the public health system; and 2) the costs for the patients. The two viewpoints will translate into two models of costs for all analyses. The key variable of interest is the total cost per live birth. This variable will be measured in two ways: 1) the total cost per infant alive for all women, which considers costs of unsuccessful interventions; and 2) the total cost per infant alive only for the women who had a live birth. Costs will include:
Costs of the lifestyle program
Health care system viewpoint – Costs for health care providers and staff (medical visits with corresponding billing, number of hours worked by health professionals and administrative staff), interdisciplinary meetings with case discussion, meetings related to the operation of the program, medical testing, consumables. Patients’ viewpoint – Costs for transportation, parking, loss of salary (patient & life partner), daycare.
Costs of fertility treatments
Health care system viewpoint – Costs for health care providers and staff (idem), drugs, medical testing, consumables, and billing of ART-related investigations or treatments to the public system if applicable. Patients’ viewpoint – Costs for transportation, parking, loss of salary, daycare, drugs not covered, and billing of ART-related investigations or treatments to the patient if applicable.
Costs of adverse events or complications
Health care system viewpoint – Costs of hospitalization or drugs for adverse events related to the lifestyle program, fertility treatments, pregnancy or neonatal care. Patients’ viewpoint – Costs for transportation, parking, loss of salary, daycare, drugs not covered, incurred by the patients due to these adverse events or complications.
Data collection will be performed through patients’ charts review, administrative data, questionnaires and interviews with health care providers and staff of fertility clinics for the description of care procedures, as well as questionnaires to patients. At the CHUS fertility clinic, costs will be obtained prospectively and all patients will answer a specific questionnaire; but for the three fertility clinics of comparison, patients’ charts will be retrospectively reviewed. However, as mentioned, a sample of 20 patients will be selected for focus groups: these patients will also answer the same cost questionnaire. Thus, the exact costs from the patients’ viewpoint of the different events will be determined based on these 20 patients and then be extrapolated to the other patients. Departments or directorates of service (billing services at the CHUS, pharmacies, Human Resources, Department of Nursing) will be consulted to match each event to its monetary cost. Where possible, we will use the overhead costs, provided by the administrative services, for a particular treatment and/or complication. When this is not possible, we will conduct interviews with relevant professionals to track the various human resources and materials that were involved.
Since provincial and state pricings for the different outcomes are different, we will only consider a single reference price for each outcome, i.e. pricing in the Quebec health system. In order not to incur double counting in calculating the cost of primary outcome, we will make sure to check the reason for the expense and we will record every cost only once for the primary outcome. Regarding the joint use of equipment or spaces, the cost used will be the unit cost of depreciation for each use or visit. To the extent that the cost measure will be done over a period exceeding one year, we will use a discount rate. The reference discount rate will be 5 % per year. To test the robustness of our results, we also do a sensitivity analysis with rates of 3 and 8 %.
Assessment of quality-adjusted life years (QALYs) and cost-effectiveness of the intervention will be performed using the Short Form-6D (SF-6D). SF-6D is a generic preference-based measure of health derived from the SF-36 Health Survey for use in economic evaluation [54]. It is composed of six dimensions of health: physical functioning, role limitations, social functioning, pain, mental health and vitality. Each dimension has between 4 and 6 levels. The SF-6D defines 18,000 different possible health states, and has a range from 0.3 (worst health state) to 1.0 (best health state) in model 10 [54].
Variables and research tools
Specific research tools for each objective are summarized in Table 2, which includes corresponding variables as well as the sources that will be used to obtain required data and the time of data collection.
Health professionals’ perceptions and satisfaction (Objective 1)
Health professionals’ attitudes, perceptions, self-efficacy toward obesity management, and other characteristics (age, experience in obesity management) will be evaluated with a questionnaire that we have developed and used in previous studies [55]. Self-efficacy is defined as the set of beliefs about one’s capabilities to perform at a designated level. It is particularly important in the context of the implementation of a new program since it may be influenced by the practice environment [56]. For health professionals to engage in weight management with their patients, they must not only accept this as part of their role but also feel that they are competent to accomplish the task. Negative attitudes toward obese individuals and perceptions to the effect that available treatments are ineffective can prevent the engagement of health professionals in weight management. There is also a positive correlation between the feeling of competency and the degree of engagement regarding various aspects of obesity management and improved attitude towards obese individuals [57, 58]. A separate questionnaire will gather detailed information on strengths of the program, difficulties and areas of possible improvement.
A qualitative in-depth analysis of key stakeholder perceptions of the program and fertility clinics will be performed using semi-structured interviews (MDs, nurses, dietitians, kinesiologists, psychologists, clinic administrative personnel and directors), as we have previously done [59, 60]. This will increase our understanding of their personal experience, inter-professional collaboration and satisfaction with the program, and further identify and detail strengths and areas for potential improvement. This will also permit a better understanding of the change process.
Patients’ perceptions and satisfaction (Objective 1)
Patient expectations and perceptions of their personal experience regarding weight management, fertility care and pregnancy follow-up, as well as their satisfaction regarding management by their health professionals will be evaluated with questionnaires based on experience from previous studies. A qualitative in-depth analysis of patients’ perceptions of the program and medical care will also enhance our understanding of their personal experience with the program. After the completion of the quantitative evaluation of impact of the program on patients, a theoretical sample based on the technique of critical incidents will be used to create a sub-sample of the whole group. Twenty patients will be recruited in each of the 4 participating clinics (80 patients). To be recruited those patients will have to show certain characteristics (different levels of satisfaction with their care (at CHUS, based on questionnaires), different fertility or pregnancy outcomes, loss or gain of weight during follow-up, etc.). The patients will be participating in a taped-recorded semi-structured qualitative interview to assess their perceptions of impact of their participation into the program (continuity of care, perceptions of changes, contribution to change, quality of life, perspectives of future changes, explanation of level of satisfaction with the program). An interview guide with open-ended questions adapted from the principal variables of the study, the Diabetic Empowerment Scale (DES) [59], and the Impact of Weight on Quality of Life (IWQOL-lite) questionnaire [61] will be used as done in previous studies from members of our group [49, 62].
Evaluation of anthropometric and lifestyle benefits and impact on fertility, pregnancy and neonatal outcomes (CHUS only) (Objective 2)
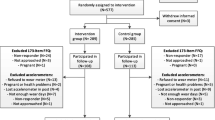
Evaluations of anthropometric measures and lifestyle habits will take place at baseline, prior to randomisation, and then every 6 months for 18 months. Among women who become pregnant, data will be collected, at the beginning of the pregnancy and at 24–28 weeks. If a woman becomes pregnant within a month of a standard evaluation visit, this visit will be considered as the first pregnancy visit. If a miscarriage occurs, the original follow-up will continue until 18 months or the end of another pregnancy. An overview of the study design and data collection is provided in Fig. 1.

Summary of design and data collection of the Obesity-Fertility protocol
Anthropometric measures and vital signs:
Weight will be measured by a standard calibrated scale and height will be measured with a stadiometer. In non-pregnant women, waist circumference will be measured with a measuring tape, as recommended [47, 63]. Fat mass and percent body fat will be measured by standing electric bioimpedance, which was shown to be reliable compared to underwater weighing and supine tetrapolar bioimpedance [64, 65]. Blood pressure and pulse rate will be measured after five minutes of rest, in the sitting position. The average of two measurements will be used for analysis.
Blood sample:
Different metabolic markers related to insulin secretion, androgen and lipid profile will be measured fasting: apolipoprotein B (ApoB), total cholesterol, triglycerides, high-density lipoprotein cholesterol (HDL), low-density lipoprotein cholesterol (LDL), cholesterol ratio, thyroid-stimulating hormone (TSH), prolactin (PRL), cortisol, adrenocorticotropic hormone (ACTH), β-hCG, total and free testosterone, Sex hormone-binding globulin (SHBG), 17-hydroxyprogesterone, dehydroepiandrosterone sulfate (DHEAS), androstenedione, C-peptide, glucose and insulin. A 2-hour oral glucose tolerance test (OGTT) will be also performed with blood sample taken every 30 min. Samples will be stored at each time points for future measurements of adipokines or other analytes pertinent to the objectives of this study, if funding allows it.
Lifestyle:
Physical activity level and eating habits will be measured using a questionnaire adapted from the one used by Statistics Canada for the latest Canadian Health Survey. This questionnaire inquires about the frequency and duration of active travelling, leisure time, and sedentary activities (television watching, video games, computers). We chose this questionnaire since it allows comparison of the characteristics of our patients to those of the general Canadian population. Moreover, women will be asked to wear a tri-axial accelerometer (GT3X+, Actigraph, Pensacola, FL, USA) on their hip for seven consecutive days except during sleep and showering/bathing. The accelerometer will be used to estimate daily energy expenditure from physical activities, time spent in various physical activity intensities and step count. The GT3X+ has been shown to be a valid and reliable measure of physical activity in free living conditions [66].
Fitness level:
The six-minute walk test (6MWT) is a simple test that has been used to estimate functional capacity in obese subjects and is also a predictor of morbidity and mortality [67–69]. The 6MWT will be performed according to the protocol recommended by the American Thoracic Society in a 20-meter hallway marked every 5 m with coloured tapes on the floor, and measures the distance that a patient can quickly walk in a period of 6 min [70]. It has been shown that weight loss increases fitness level early in the weight loss process, making this test a very accurate tool to evaluate the impact of the intervention on obese or overweight patients’ functional capacity [71–73].
Readiness for change:
In the course of previous prospective studies, we have designed a 22-question weight loss readiness tool (WLRT) questionnaire based on Prochaska and DiClemente’s Stages of Change Model [47, 74]. It evaluates the motivational readiness of patients regarding weight management, nutrition and physical activity, and could predict response to an intervention. Our WLRT takes 5–10 min to fill out, making it a clinically applicable tool. It has been useful to identify subjects with greater chances of success for lifestyle modification in a previous pilot study [75]. Its predictive value will be assessed in this study, but it will also serve to explore the mechanisms of potential benefits of our intervention and for stratified analyses.
Quality of life:
The impact of fertility problems and its treatment on quality of life will be measured using the fertility quality of life (FertiQoL) tool, a reliable and sensitive questionnaire to evaluate quality of life in individuals with fertility problems [76].
Evaluation of fertility, pregnancy complications and neonatal outcomes (all sites)
Medical records:
Chart review of the mother will be performed using a standardized evaluation grid, and we will check personal medical and surgical history, medications, weight, and any particular events at each visit. This chart review will also identify information about fertility treatments and pregnancy complications. Information about the newborn will be collected via the obstetric file of the mother.
Administrative data and other databases:
Data from the chart review will be cross-validated with administrative data and any databases used in fertility clinics and/or local hospitals. At the CHUS, all laboratory testing and all information regarding hospitalisations are merged together and kept in the “Centre informatisé de recherche évaluative en services et soins de santé” (CIRESSS) database, which is available for research with appropriate authorizations.
Data analyses and interpretation
For objectives 1–2, all comparisons between randomized groups at the CHUS will follow both the intent-to-treat and/or per-protocol principles, and will consider results at the end of study. For repeated measures, the last-observation-carried-forward method will be used for women who drop out or become pregnant (depending on analyses). Time-to-event analyses will also be performed for fertility outcomes, with censoring for drop out alone, as well as for anthropometric outcomes, with censoring for both drop out and occurrence of pregnancy. Univariate analyses will compare the change in a variable in the intervention group with the change in this variable in the control group, using two-tailed unpaired t tests (for continuous variables) and chi-square or Fisher’s exact tests (for categorical variables). Changes in weight will also be compared for the same follow-up duration with changes for women seen at the other fertility clinics, using ANOVA tests. For the other variables, only end-of-study comparisons will be performed between the two groups in Sherbrooke and the three other fertility clinics, using ANOVA tests (for continuous variables) and logistic regressions (for categorical variables). Bonferroni-corrected p-values will be performed to adjust for the multiplicity of comparisons and an α level of 5 % will be considered significant for all analyses. Continuous variables that are not normally distributed will be log-transformed in order to ascertain normal distribution. Multivariate analyses will also be used in order to adjust for baseline differences and for potential confounders, and to determine independent predictors of outcomes. Triangulation will be performed between quantitative and qualitative data.
Sample size
Our sample size estimation is based upon our primary outcome (see Objective 2), which is live-birth rates between randomized groups at the CHUS. Based on the Fertility Fitness Program, the inclusion of 58 women per group will provide our study a power of 80 % to identify a doubling in live-birth rates with our program (25 to 50 %, α = 5 %). Assuming a dropout rate of 10 % (these women are usually highly motivated), our final estimated sample size will be 128 women. For other objectives and outcomes, it would be difficult to assess power because similar evaluations have not been previously reported.
Knowledge translation and transfer plan (Objective 4)
It is worth mentioning that both our research program and research design are optimal to allow knowledge translation (KT) and application throughout the entire research process. Integrated KT is an important outcome of this research and will take form of regular meetings of the Advisory and Steering committees. Because of the involvement on these committees of representatives of Quebec and Ontario Ministries of Health, fertility clinics and CON, as well as expert clinicians, diffusion of results and exchange of experiences will be facilitated.
However, research by itself does little to induce change (except for participants) and thus, results have to be diffused to interested audiences. Our research is relevant to health professionals, healthcare system decision-makers and policy-makers, patients and Canadian population. We will reach out to these target audiences through linkage and exchange activities, including presentation of study results at local, national and international scientific meetings attended by interested stakeholders in the obesity, reproductive endocrinology, fertility and health services fields and publication in scientific journals, but also by direct reports to healthcare system decision-makers. A clear summary of research results, including key messages targeted for each selected audience and synthesized results, will be available (printed and on a web site). Local and national media will be invited to press conferences and we will schedule private meetings with important decision-makers to whom our findings are relevant.
Discussion
This paper has outlined the protocol of a study assessing clinical outcomes and costs of a transferable interdisciplinary lifestyle intervention, before and during pregnancy, in obese infertile women. We are using a RCT design for proximal clinical outcomes, and mixed design for cost-effectiveness evaluation and qualitative assessment for the purpose of future dissemination and knowledge transfer. To our knowledge, we are the first in the world to conduct such a program with lifestyle intervention continuing throughout fertility treatments and pregnancy. This project is very important as it will generate new knowledge about the implementation, impacts and costs of a lifestyle management program in obese infertile women. The results of this study will provide valuable information on feasibility and transferability of such a program, including identification of barriers and solutions. We expect that our program will improve the lifestyle and fertility of the participants and reduce maternal and fetal complications during pregnancy, as compared with our different control groups. A significant reduction in cost per live birth and cost-effectiveness ratio is also anticipated.
Although this research protocol is innovative and uses a robust methodology, some limitations need to be acknowledged. First, implementation and outcome evaluation of the lifestyle program will take place in a single clinic. However, a RCT at the CHUS will be performed with sufficient power to assess the primary outcome. Results will also be compared to three other clinics, which is an ideal first step for the future development of a multicenter RCT. It is important to appropriately design and evaluate the program in one center before transferring it to other centers. Second, some of the outcome measures will be self-reported and might be biased. However, such bias should be similar in both randomized groups and the results will be triangulated with data from many different sources (administrative data, questionnaires, focus groups, etc.). Third, most of the outcomes will be assessed only retrospectively in the clinics of comparison. This might introduce an evaluation bias although multiple sources of information will be used and compared. A recall bias is also possible for the evaluation of costs for the patients’ viewpoint in these clinics, but the same estimations will be performed in Sherbrooke and compared with real costs, which will allow the determination of the degree of this bias for comparison clinics. Fourth, in Sherbrooke, fertility treatments, including IVF, will be covered by the public health care system. Therefore, some results may not reflect all North American fertility clinics, but the same results will be compared to clinics in other provinces where fertility treatments are not covered.
The outcome measures of this study will be relevant to a number of health systems’ managers and policy-makers. Indeed, new approaches aiming at increasing efficiency and reducing costs of fertility treatments, while improving care, are thus very pertinent for these policy-makers. This research proposal is completely in line with those objectives and is developed in partnership with local, provincial and national decision-makers, which increases the potential impact and use of the findings. Generalizability of our findings is increased by the evaluation of clinics from three different provinces and the involvement of the CON as a partner. Furthermore, experts and decision-makers from various provinces will participate on the Advisory committee to ensure that the developed intervention can be applied in other contexts. Early and active involvement of decision-makers will ensure that the intervention is appropriately designed to be implemented in most North American fertility clinics.
Abbreviations
- 6MWT:
-
Six-minute walk test
- ACTH:
-
Adrenocorticotropic hormone
- ApoB:
-
Apolipoprotein B
- ART:
-
Assisted reproductive technologies
- β-hCG:
-
Beta-human chorionic gonadotropin
- BMI:
-
Body mass index
- CIRESSS:
-
Centre informatisé de recherche évaluative en services et soins de santé
- CHUS:
-
Centre hospitalier universitaire de Sherbrooke
- CON:
-
Canadian Obesity Network
- DES:
-
Diabetic Empowerment Scale
- DHEAS:
-
Dehydroepiandrosterone sulfate
- DM2:
-
Type 2 diabetes
- FertiQol:
-
Fertility quality of life
- GREI:
-
Gynecologic reproductive endocrinology and infertility
- HDL:
-
High-density lipoprotein cholesterol
- IVF:
-
In vitro fertilization
- IWQOL-Lite:
-
Impact of Weight on Quality of Life
- KT:
-
Knowledge translation
- LDL:
-
Low-density lipoprotein cholesterol
- OGTT:
-
Oral glucose tolerance test
- PCOS:
-
Polycystic ovary syndrome
- PRL:
-
Prolactin
- QALYs:
-
Quality-adjusted life years
- RCT:
-
Randomized controlled trial
- SF-6D:
-
Short Form-6D
- SHBG:
-
Sex hormone-binding globulin
- TSH:
-
Thyroid-stimulating hormone
- WLRT:
-
Weight loss readiness tool
References
Practice Committee of the American Society of Reproductive Medicine. Optimal evaluation of the infertile female. Fertil Steril. 2004;82 Suppl 1:S169–72.
Brassard M, AinMelk Y, Baillargeon JP. Basic infertility including polycystic ovary syndrome. Med Clin North Am. 2008;92(5):1163–92. xi.
Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E, Escobar-Morreale HF, Futterweit W, et al. Positions statement: criteria for defining polycystic ovary syndrome as a predominantly hyperandrogenic syndrome: an Androgen Excess Society guideline. J Clin Endocrinol Metab. 2006;91(11):4237–45.
Carmina E, Azziz R. Diagnosis, phenotype, and prevalence of polycystic ovary syndrome. Fertil Steril. 2006;86 Suppl 1:S7–8.
Azziz R, Woods KS, Reyna R, Key TJ, Knochenhauer ES, Yildiz BO. The prevalence and features of the polycystic ovary syndrome in an unselected population. J Clin Endocrinol Metab. 2004;89(6):2745–9.
Baptiste CG, Battista MC, Trottier A, Baillargeon JP. Insulin and hyperandrogenism in women with polycystic ovary syndrome. J Steroid Biochem Mol Biol. 2010;122(1–3):42–52.
Massicotte MH, Langlois F, Baillargeon JP. Current procedures for managing polycystic ovary syndrome. Expert Review of Obstetrics & Gynecology. 2010;5(1):77–91.
Baillargeon JP, Nestler JE. Commentary: polycystic ovary syndrome: a syndrome of ovarian hypersensitivity to insulin? J Clin Endocrinol Metab. 2006;91(1):22–4.
Gambineri A, Pelusi C, Vicennati V, Pagotto U, Pasquali R. Obesity and the polycystic ovary syndrome. Int J Obes Relat Metab Disord. 2002;26(7):883–96.
Yildiz BO, Knochenhauer ES, Azziz R. Impact of obesity on the risk for polycystic ovary syndrome. J Clin Endocrinol Metab. 2008;93(1):162–8.
Bolumar F, Olsen J, Rebagliato M, Saez-Lloret I, Bisanti L. Body mass index and delayed conception: a European Multicenter Study on Infertility and Subfecundity. Am J Epidemiol. 2000;151(11):1072–9.
Gesink Law DC, Maclehose RF, Longnecker MP. Obesity and time to pregnancy. Hum Reprod. 2007;22(2):414–20.
Jensen TK, Scheike T, Keiding N, Schaumburg I, Grandjean P. Fecundability in relation to body mass and menstrual cycle patterns. Epidemiology. 1999;10(4):422–8.
Statistique Canada. Enquête sur la santé dans les collectivités canadiennes (ESCC) 2004–2008; tableau CANSIM 105–0507. 2014.
Bhattacharya S, Porter M, Amalraj E, Templeton A, Hamilton M, Lee AJ, et al. The epidemiology of infertility in the North East of Scotland. Hum Reprod. 2009;24(12):3096–107.
Galtier-Dereure F, Pujol P, Dewailly D, Bringer J. Choice of stimulation in polycystic ovarian syndrome: the influence of obesity. Hum Reprod. 1997;12 Suppl 1:88–96.
Lobo RA, Gysler M, March CM, Goebelsmann U, Mishell Jr DR. Clinical and laboratory predictors of clomiphene response. Fertil Steril. 1982;37(2):168–74.
Zaadstra BM, Seidell JC, Van Noord PA, te Velde ER, Habbema JD, Vrieswijk B, et al. Fat and female fecundity: prospective study of effect of body fat distribution on conception rates. BMJ. 1993;306(6876):484–7.
Pasquali R, Pelusi C, Genghini S, Cacciari M, Gambineri A. Obesity and reproductive disorders in women. Hum Reprod Update. 2003;9(4):359–72.
Fedorcsak P, Dale PO, Storeng R, Ertzeid G, Bjercke S, Oldereid N, et al. Impact of overweight and underweight on assisted reproduction treatment. Hum Reprod. 2004;19(11):2523–8.
Wang JX, Davies M, Norman RJ. Body mass and probability of pregnancy during assisted reproduction treatment: retrospective study. BMJ. 2000;321(7272):1320–1.
Dokras A, Baredziak L, Blaine J, Syrop C, VanVoorhis BJ, Sparks A. Obstetric outcomes after in vitro fertilization in obese and morbidly obese women. Obstet Gynecol. 2006;108(1):61–9.
Wang JX, Davies MJ, Norman RJ. Obesity increases the risk of spontaneous abortion during infertility treatment. Obes Res. 2002;10(6):551–4.
Cedergren MI. Maternal morbid obesity and the risk of adverse pregnancy outcome. Obstet Gynecol. 2004;103(2):219–24.
Cnattingius S, Bergstrom R, Lipworth L, Kramer MS. Prepregnancy weight and the risk of adverse pregnancy outcomes. N Engl J Med. 1998;338(3):147–52.
Weiss JL, Malone FD, Emig D, Ball RH, Nyberg DA, Comstock CH, et al. Obesity, obstetric complications and cesarean delivery rate--a population-based screening study. Am J Obstet Gynecol. 2004;190(4):1091–7.
Lewis G, editor. Why mothers die 2000–2002. London: Confidential Enquiry into Maternal and Child Health; 2004.
Watkins ML, Rasmussen SA, Honein MA, Botto LD, Moore CA. Maternal obesity and risk for birth defects. Pediatrics. 2003;111(5 Part 2):1152–8.
Marchi J, Berg M, Dencker A, Olander EK, Begley C. Risks associated with obesity in pregnancy, for the mother and baby: a systematic review of reviews. Obes Rev. 2015;16(8):621–38.
Chu SY, Bachman DJ, Callaghan WM, Whitlock EP, Dietz PM, Berg CJ, et al. Association between obesity during pregnancy and increased use of health care. N Engl J Med. 2008;358(14):1444–53.
Galtier-Dereure F, Boegner C, Bringer J. Obesity and pregnancy: complications and cost. Am J Clin Nutr. 2000;71(5 Suppl):1242S–8S.
Koning AM, Kuchenbecker WK, Groen H, Hoek A, Land JA, Khan KS, et al. Economic consequences of overweight and obesity in infertility: a framework for evaluating the costs and outcomes of fertility care. Hum Reprod Update. 2010;16(3):246–54.
Huda SS, Brodie LE, Sattar N. Obesity in pregnancy: prevalence and metabolic consequences. Semin Fetal Neonatal Med. 2010;15(2):70–6.
Jarvie E, Hauguel-de-Mouzon S, Nelson SM, Sattar N, Catalano PM, Freeman DJ. Lipotoxicity in obese pregnancy and its potential role in adverse pregnancy outcome and obesity in the offspring. Clin Sci (Lond). 2010;119(3):123–9.
Bouchard L, Thibault S, Guay SP, Santure M, Monpetit A, St-Pierre J, et al. Leptin gene epigenetic adaptation to impaired glucose metabolism during pregnancy. Diabetes Care. 2010;33(11):2436–41.
Crosignani PG, Colombo M, Vegetti W, Somigliana E, Gessati A, Ragni G. Overweight and obese anovulatory patients with polycystic ovaries: parallel improvements in anthropometric indices, ovarian physiology and fertility rate induced by diet. Hum Reprod. 2003;18(9):1928–32.
Guzick DS, Wing R, Smith D, Berga SL, Winters SJ. Endocrine consequences of weight loss in obese, hyperandrogenic, anovulatory women. Fertil Steril. 1994;61(4):598–604.
Clark AM, Thornley B, Tomlinson L, Galletley C, Norman RJ. Weight loss in obese infertile women results in improvement in reproductive outcome for all forms of fertility treatment. Hum Reprod. 1998;13(6):1502–5.
Clark AM, Ledger W, Galletly C, Tomlinson L, Blaney F, Wang X, et al. Weight loss results in significant improvement in pregnancy and ovulation rates in anovulatory obese women. Hum Reprod. 1995;10(10):2705–12.
Huber-Buchholz MM, Carey DG, Norman RJ. Restoration of reproductive potential by lifestyle modification in obese polycystic ovary syndrome: role of insulin sensitivity and luteinizing hormone. J Clin Endocrinol Metab. 1999;84(4):1470–4.
Moran LJ, Noakes M, Clifton PM, Tomlinson L, Galletly C, Norman RJ. Dietary composition in restoring reproductive and metabolic physiology in overweight women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2003;88(2):812–9.
Pelletier L, Baillargeon JP. Clinically significant and sustained weight loss is achievable in obese women with polycystic ovary syndrome followed in a regular medical practice. Fertil Steril. 2010;14(7):2665-9.
Practice Committee of American Society for Reproductive Medicine. Obesity and reproduction: an educational bulletin. Fertil Steril. 2008;90(5 Suppl):S21–29.
Siega-Riz AM, King JC. Position of the american dietetic association and american society for nutrition: obesity, reproduction, and pregnancy outcomes. J Am Diet Assoc. 2009;109(5):918–27.
Dondorp W, de Wert G, Pennings G, Shenfield F, Devroey P, Tarlatzis B, et al. Lifestyle-related factors and access to medically assisted reproduction. Hum Reprod. 2010;25(3):578–83.
Balen AH, Anderson RA. Impact of obesity on female reproductive health: British fertility society, policy and practice guidelines. Hum Fertil (Camb). 2007;10(4):195–206.
Lau DC, Douketis JD, Morrison KM, Hramiak IM, Sharma AM, Ur E. 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children [summary]. CMAJ. 2007;176(8):S1–13.
Kamga-Ngande CN, Carpentier AC, Nadeau-Marcotte F, Ardilouze JL, Baillargeon JP, Bellabarba D, et al. Effectiveness of a multidisciplinary program for management of obesity: the Unité d’enseignement, de traitement et de recherche en obésité (UETRO) database study. Metab Syndr Relat Disord. 2009;7(4):297–304.
Kamga CN, Carpentier A, Baillargeon JP, Dionne I, Ardilouze JL, Langlois MF. Treatment of the Metabolic Syndrome in an interdisciplinary obesity clinic: a randomized controlled study. North American Association for the Study of Obesity’s 2005 Annual Scientific Meeting. Obes Res. 2005;13(Abstract Suppl):A1–218.
Gagnon C, Brown C, Couture C, Kamga-Ngande CN, Hivert MF, Baillargeon JP, Carpentier AC, Langlois MF. A cost-effective moderate-intensity interdisciplinary weight-management programme for individuals with prediabetes. Diabetes Metab. 2011;37(5):410-8.
Ministère de la santé et des services sociaux du Québec, Diabète Québec. Meal planning for people with diabetes at a glance. Direction des communications du Ministère de la santé et des services sociaux; Montréal: Diabète Québec. 2014.
Armstrong MJ, Mottershead TA, Ronksley PE, Sigal RJ, Campbell TS, Hemmelgarn BR. Motivational interviewing to improve weight loss in overweight and/or obese patients: a systematic review and meta-analysis of randomized controlled trials. Obes Rev. 2011;12(9):709–23.
Rasmussen KM, Yaktine AL. Weight gain during pregnancy: Reexamining the guidelines. Washington: National Academies Press; 2009.
Brazier J, Roberts J, Deverill M. The estimation of a preference-based measure of health from the SF-36. J Health Econ. 2002;21(2):271–92.
Baillargeon JP, Carpentier A, Donovan D, Fortin M, Grant A, Simoneau-Roy J, et al. Integrated obesity care management system -implementation and research protocol. BMC Health Serv Res. 2007;7:163.
Bandura A. Self-efficacy. In: Ramachaudran VS, editor. Encyclopedia of human behavior. Orlando: Academic; 1994.
Baillargeon JP, St-Cyr-Tribble D, Xhignesse M, Grant A, Carpentier A, Donovan D, et al. Obesity preceptorship and virtual community result in changes of primary care practice. 2008 Annual scientific meeting NAASO, Phoenix AZ. Obesity. 2008;16(Suppl):S152.
Baillargeon JP, Xhignesse M, Carpentier A, Donovan D, Grant A, Fortin M, et al. Preceptorship and virtual community improve health care professionals perceptions toward obesity care and reported management of obesity after one year. San Francisco: The Endocrine Society’s 90th Annual meeting; 2008.
St-Cyr-Tribble D, Gallagher F, Vanasse A, Doré C, Archambault J, Fortin M. Programme d’intervention fondé sur un modèle de collaboration interprofessionnelle et de promotion de l’autosoin auprès des diabétiques de type 2. Rapport de recherche, FCRSS & Aventis Canada. 2007.
Langlois MF, et al. Integrated obesity care management system: executive summary. 2008.
Kolotkin RL, Head S, Hamilton M, Tse CK. Assessing impact of weight on quality of life. Obes Res. 1995;3(1):49–56.
Levasseur M, Tribble DS, Desrosiers J. Analysis of quality of life concept in the context of older adults with physical disabilities. Can J Occup Ther. 2006;73(3):163–77.
Poirier P, Despres JP. Waist circumference, visceral obesity, and cardiovascular risk. J Cardiopulm Rehabil. 2003;23(3):161–9.
Cable A, Nieman DC, Austin M, Hogen E, Utter AC. Validity of leg-to-leg bioelectrical impedance measurement in males. J Sports Med Phys Fitness. 2001;41(3):411–4.
Gagnon C, Menard J, Bourbonnais A, Ardilouze JL, Baillargeon JP, Carpentier AC, et al. Comparison of foot-to-foot and hand-to-foot bioelectrical impedance methods in a population with a wide range of body mass indices. Metab Syndr Relat Disord. 2010;8(5):437–41.
Santos-Lozano A, Santin-Medeiros F, Cardon G, Torres-Luque G, Bailon R, Bergmeir C, et al. Actigraph GT3X: validation and determination of physical activity intensity cut points. Int J Sports Med. 2013;34(11):975–82.
Hulens M, Vansant G, Claessens AL, Lysens R, Muls E. Predictors of 6-minute walk test results in lean, obese and morbidly obese women. Scand J Med Sci Sports. 2003;13(2):98–105.
Hulens M, Vansant G, Lysens R, Claessens AL, Muls E. Exercise capacity in lean versus obese women. Scand J Med Sci Sports. 2001;11(5):305–9.
Solway S, Brooks D, Lacasse Y, Thomas S. A qualitative systematic overview of the measurement properties of functional walk tests used in the cardiorespiratory domain. Chest. 2001;119(1):256–70.
ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–7.
Maniscalco M, Zedda A, Giardiello C, Faraone S, Cerbone MR, Cristiano S, et al. Effect of bariatric surgery on the six-minute walk test in severe uncomplicated obesity. Obes Surg. 2006;16(7):836–41.
Lemoine S, Rossell N, Drapeau V, Poulain M, Garnier S, Sanguignol F, et al. Effect of weight reduction on quality of life and eating behaviors in obese women. Menopause. 2007;14(3 Pt 1):432–40.
Beriault K, Carpentier AC, Gagnon C, Menard J, Baillargeon JP, Ardilouze JL, et al. Reproducibility of the 6-minute walk test in obese adults. Int J Sports Med. 2009;30(10):725–7.
Norcross JC, Prochaska JO. Using the stages of change. Harv Ment Health Lett. 2002;18(11):5–7.
Kong W, Langlois MF, Kamga-Ngande C, Gagnon C, Brown C, Baillargeon JP. Predictors of success to weight-loss intervention program in individuals at high risk for type 2 diabetes. Diabetes Res Clin Pract. 2010;90(2):147–53.
Boivin J, Takefman J, Braverman A. The fertility quality of life (FertiQoL) tool: development and general psychometric properties. Hum Reprod. 2011;26(8):2084–91.
Acknowledgements
This work was supported by the Canadian Institutes for Health Research (CIHR; FRN-114125) and the Ministère de la santé et des services sociaux of Québec (MSSS, Programme québécois de contrepartie au Programme de partenariats pour l’amélioration du système de santé des IRSC). JPB is a Senior Clinical Investigator of the FRQS. MFL is a National Investigator of the FRQS.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
JPB, MFL, BCM, MHP, MFH, HBL contributed significantly to the study design; TGP for cost-effectiveness evaluation and DSCT for qualitative assessments. All other authors (KD, YA, SL, EG, MS, GW, SB, DR, FJD, MB) discussed and commented the study design. KD and JPB wrote the first draft of the manuscript and all authors (KD, MFL, BCM, MHP, MFH, TGP, HBL, YA, DSCT, SL, EG, MS, GW, SB, DR, FJD, MB, JPB) read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Duval, K., Langlois, MF., Carranza-Mamane, B. et al. The Obesity-Fertility Protocol: a randomized controlled trial assessing clinical outcomes and costs of a transferable interdisciplinary lifestyle intervention, before and during pregnancy, in obese infertile women. BMC Obes 2, 47 (2015). https://doi.org/10.1186/s40608-015-0077-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40608-015-0077-x