
Abstract
Background
This systematic review and meta-analysis of randomized clinical trials aimed to investigate the efficacy of early mobilization among critically ill adult patients.
Methods
We searched CENTRAL, MEDLINE, and Igaku-Chuo-Zasshi (a Japanese bibliographic database) databases until April 2019 and included randomized control trials to compare early mobilization started within 1 week of intensive care unit (ICU) admission and earlier-than-usual care with the usual care or mobilization initiated later than the intervention. Two authors independently extracted the data of the included studies and assessed their quality. The primary outcomes were in-hospital mortality, length of ICU/hospital stay, and health-related quality of life (QOL).
Results
Among 1085 titles/abstracts screened, 11 studies (including 1322 patients) were included in the meta-analysis, which was conducted using the random-effects model. The pooled relative risk for in-hospital mortality comparing early mobilization to usual care (control) was 1.12 (95% CI [confidence interval]: 0.80 to 1.58, I2 = 0%). The pooled mean differences for duration of ICU and hospital stay were -1.54 (95% CI: -3.33 to 0.25, I2 = 90%) and -2.86 (95% CI: -5.51 to -0.21, I2 = 85%), respectively. The pooled mean differences at 6 months post-discharge, as measured by the Short Form 36-Item Health Survey and Euro-QOL EQ-5D, were 4.65 (95% CI: -16.13 to 25.43, I2 = 86%) for physical functioning and 0.29 (95% CI: -11.19 to 11.78, I2 = 66%) for the visual analog scale.
Conclusions
Our study indicated no apparent differences between early mobilization and usual care in terms of in-hospital mortality and health-related QOL. Detailed larger studies are warranted to evaluate the impact of early mobilization on in-hospital mortality and health-related QOL in critically ill patients.
Trial registration
PROSPERO (identifier CRD42019139265)
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Early mobilization and physiotherapy have been used to prevent post-intensive care syndrome and ICU-acquired weakness (ICU-AW) in critically ill adult patients in the intensive care unit (ICU) [1, 2]. Two systematic reviews with meta-analysis have demonstrated that these interventions may help improve short-term physical function and decrease the duration of mechanical ventilation or ICU stay; this has also been advocated in clinical practice guidelines [1,2,3,4]. However, previous studies do not indicate whether these interventions improved more relevant outcomes such as mortality and health-related quality of life (QOL) [1,2,3,4,5]. Therefore, it is necessary to focus on these outcomes when examining the effects of early mobilization in ICU patients. This systematic review and meta-analysis aimed to investigate the efficacy on the mortality and health-related QOL of early mobilization among critically ill adult patients.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol for randomized clinical trials (RCTs) [6]. This review protocol was submitted to the International Prospective Register of Systematic Reviews (PROSPERO) on June 18, 2019, before the initiation of data extraction and was approved for registration on August 15, 2019 (PROSPERO identifier: CRD 42019139265). The protocol is described in the Additional file 1.
Data sources and searches
We searched for eligible trials in the Cochrane Central Register of Controlled Trials (CENTRAL) via the Cochrane Library (on April 24, 2019), in MEDLINE via PubMed (on April 28, 2019), and in Igaku-Chuo-Zasshi (Ichu-shi) (on April 26, 2019). Ichu-shi is a Japanese bibliographic database managed by the Japan Medical Abstracts Society. Our search strategies are described in the Additional file 1. We also performed a manual search to retrieve all potentially relevant articles on June 21, 2019. Searches were restricted to articles written and published in English or Japanese.
Eligibility criteria
We set the following eligibility criteria: study design was RCT, and the target populations were critically ill adult patients (aged≥18 years) admitted to the ICU. The intervention was early mobilization defined as (1) physical and/or occupational therapy, (2) started within 1 week of ICU admission, and (3) initiated earlier than usual care or control, based on the previous literature [4]. The control was defined as usual care or mobilization started later than the intervention.
Selection of studies
Two authors (YO and YM) independently screened the titles and abstracts of the studies identified by the search strategy for inclusion eligibility and performed a hand search to identify relevant studies. Differences were resolved by discussion with other authors (TU and YE). We retrieved the full text of all possible eligible studies for further evaluation for inclusion. Two authors (YO and YE) independently assessed the full-text studies identified in the primary screening, and the eligible studies were finally identified. We provide the number of records assessed and excluded at each stage and the reasons for excluding full-text studies in the PRISMA flowchart [6].
Data extraction and management
The authors independently extracted data from identified eligible trials using a specifically pre-designed sheet. We compared the extracted data for differences, and disagreements were resolved by discussion among authors.
Outcomes
The primary outcomes were in-hospital mortality, length of ICU/hospital stay, and health-related QOL. Health-related QOL is defined as QOL assessed by the Short Form Health Survey 36-Item (SF-36) or EuroQol 5 dimension (EQ-5D), the two most widely accepted standardized instruments for assessing health-related QOL [7, 8]. The secondary outcomes were physical function, cognitive function, mental disorder such as depression or anxiety, and all adverse events. Physical function was assessed by grip strength, Medical Research Council (MRC) Scale for Muscle Strength score, or the Physical Function in ICU Test (PFIT) [9, 10]. Cognitive function after discharge was measured by the Mini-Mental State Examination (MMSE) [11]. For dichotomous outcomes, the total number of events and number of events within each randomization group were pooled to calculate risk ratios (RRs) with 95% confidence intervals (CIs) using random-effects models. For continuous outcomes, the median and standard deviation in each group were pooled to estimate the mean difference (MD) with 95% CI. Statistical significance was defined as the absence of overlap of a 95% CI with the null effect value (risk ratio [RR]=1).
Assessment of risk of bias
We used the Cochrane Collaboration risk of bias tool to assess the methodological quality and the extent of potential bias of the included studies [12]. The authors independently assessed the risk of bias as “low,” “high,” or “unclear” for all domains and presented our assessment in a risk of bias table within the review. Any disagreements were resolved by discussion among authors.
Patient and public involvement
As the study was a systematic review of the publication data, patients and/or the public were not involved.
Statistical analysis
We used Cochrane Statistical Package Review Manager 5.3 (Cochrane Collaboration, London, UK) for data synthesis and analysis. Because we anticipated heterogeneity among studies, we conducted the meta-analysis using the random-effects model. Heterogeneity was assessed using Chi2 and I2 statistics. Because more than ten studies were included, we examined a funnel plot to assess the potential for publication bias for our primary outcomes [12].
Results
Search results
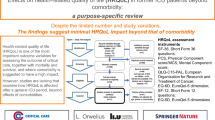
We found 492 studies in MEDLINE via PubMed, 808 in CENTRAL, 103 in Ichu-shi, and 2 in the hand search of the pre-existing systematic review [4]. After excluding duplicate studies, we screened 1085 titles/abstracts. Of these, 34 studies were eligible for a full-text review. After excluding 22 articles, we identified 12 full-text articles that met the eligibility criteria for qualitative synthesis. We excluded one article [13] owing to the lack of information on primary and secondary outcomes for meta-analysis. Finally, we performed a meta-analysis on 11 studies [14,15,16,17,18,19,20,21,22,23,24] (Fig. 1).

Prisma flowchart
Included studies
The patient characteristics and the description of intervention and control of the included 11 studies are summarized in Tables 1 and 2. Among 1322 included patients, 662 (50.1%) were assigned to early mobilization (intervention). All studies compared early mobilization versus usual care or delayed mobilization.
Risk of bias assessment
Figures 2, 3, 4, and 5 summarize the risk of bias assessments [green (+): low risk, red (-): high risk, and yellow (?): unclear]. The details of risk assessments are described in the Additional file 1. We addressed the following domains in our evaluation of bias for this trial: random sequence generation, allocation concealment, selective reporting, and other bias. We assessed the risk of bias in each outcome, particularly regarding the blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), and incomplete outcome (attrition bias).

Summary of meta-analysis and risk of bias for in-hospital mortality. CI: confidence interval, M–H: Mantel–Haenszel method. Risk of bias legend: (A) random sequence generation (selection bias), (B) allocation concealment (selection bias), (C) blinding of participants and personnel (performance bias), (D) blinding of outcome assessment (detection bias), (E) incomplete outcome data (attrition bias), (F) selective reporting (reporting bias, (G) other bias

Summary of meta-analysis and risk of bias for length of stay. a Length of ICU stay, b length of hospital stay. CI confidence interval, M–H Mantel–Haenszel method, ICU intensive care unit. Risk of bias legend: (A) random sequence generation (selection bias), (B) allocation concealment (selection bias), (C) blinding of participants and personnel (performance bias), (D) blinding of outcome assessment (detection bias), (E) incomplete outcome data (attrition bias), (F) selective reporting (reporting bias), (G) other bias

Summary of meta-analysis and risk of bias for health-related QOL (SF-36PF, EQ-5D VAS). a SF-36 PF at 6 months after randomization or hospital discharge. b EQ-5D VAS after hospital discharge. CI confidence interval, M–H Mantel–Haenszel method, QOL quality of life, EQ-5D EuroQol 5 Dimension, SF-36 PF Short Form Health Survey 36-Item, VAS visual analog scale. Risk of bias legend: (A) random sequence generation (selection bias), (B) allocation concealment (selection bias), (C) blinding of participants and personnel (performance bias), (D) blinding of outcome assessment (detection bias), (E) incomplete outcome data (attrition bias), (F) selective reporting (reporting bias), (G) other bias

Summary of meta-analysis and risk of bias for secondary outcomes: a MRC, b PFIT, c hand grip, and d adverse events. MRC Medical Research Council Scale for Muscle Strength, PFIT Physical Function in ICU Test, CI confidence interval, M–H Mantel–Haenszel method. Risk of bias legend: (A) random sequence generation (selection bias), (B) allocation concealment (selection bias), (C) blinding of participants and personnel (performance bias), (D) blinding of outcome assessment (detection bias), (E) incomplete outcome data (attrition bias), (F) selective reporting (reporting bias), (G) other bias
Some studies did not present sufficient information for the assessment of random sequence generation and allocation concealment; therefore, these studies were consequently categorized as “unclear ”[14, 16, 18, 19, 21,22,23,24]. With regard to blinding participants and personnel (performance bias), we evaluated the primary outcome of mortality as “low” risk because it was not likely to be influenced by a lack of blinding. For all other primary outcomes, we assessed all studies as “high” risk because it was largely impossible to perform physiotherapy blinded to patients and clinicians. With respect to blinding outcome assessment (detection bias), we scored subjective outcomes such as health-related QOL as “high” risk because the outcome assessor was not blinded to the allocation. For other objective outcomes such as physical function, if the outcome assessor was appropriately blinded, we scored the outcome as “low” risk. For incomplete outcome, we assessed the outcome as “low” risk if the proportion of missing outcome data was small enough or if the reasons for missing outcome data were unlikely to be related to true outcome. Otherwise, we evaluated the risk as “high.” Furthermore, for selective reporting, we scored two studies [14, 21] as “high” risk because we could not find their prespecified study protocols. For other biases, one study was evaluated as “high” risk, and another was assessed as “unclear.” The former study was an unblinded trial using blocked randomization and was held at a single institution, and the latter study did not indicate a funding source. (The detail of the risk of bias was described in Additional file 2).
Meta-analysis of the results
We synthesized the primary outcomes as follows: in-hospital mortality, duration of ICU and in-hospital stay, SF-36 physical function (PF) 6 months after randomization or hospital discharge, and EQ-5D visual analog scale (VAS) after discharge. In the primary outcomes, the pooled RR of early mobilization versus control for in-hospital mortality was 1.12 (95% CI 0.80-1.58, I2 = 0%) (Fig. 2). The pooled MD for duration of ICU stay was -1.54 (95% CI -3.33 to 0.25, I2 = 90%) (Fig. 3). The pooled MD for duration of hospital stay was -2.86 (95% CI -5.51 to -0.21, I2 = 85%) (Fig. 3). The pooled MD for SF-36 PF 6 months after discharge was 4.65 (95% CI -16.13 to 25.43, I2 = 86%) (Fig. 4). The pooled MD for EQ-5D VAS after discharge was 0.29 (95% CI -11.19 to 11.78, I2 = 66%) (Fig. 4). According to these data, the effect of early mobilization on primary outcomes was only favorable for the length of hospital stay.
The results of the meta-analysis for secondary outcomes are summarized in Fig. 5. As previous studies have reported, the MRC score in the early mobilization group was superior to that in the control group [pooled MD 4.84 (95% CI: 0.36-9.31)]. In other secondary outcomes, there was no significant difference, suggesting the superiority of early mobilization over control (Fig. 5). We could not perform a meta-analysis for cognitive function (MMSE) and mental disorder because the number of trials available to report these outcomes was less than two.
For assessment of publication bias, we described a funnel plot among the outcomes, which were reported in more than ten trials (the length of ICU and hospital stay). This plot indicated a symmetric distribution of the effect (Additional file 2), and there was no publication bias.
Discussion
Summary of the main results
Our systematic review and meta-analysis indicated that there were no apparent differences between early mobilization and control in terms of in-hospital mortality and health-related QOL (SF-36PF and EQ-5D VAS). Early mobilization was favorable in terms of the length of hospital stay; however, there may have been bias due to the lack of blinding or clinical heterogeneity. These results demonstrate that the currently available data are inadequate in establishing the superiority of early mobilization in improving relevant patient outcomes. A larger study is needed to evaluate the effects of early mobilization on in-hospital mortality and health-related QOL in critically ill patients.
Strengths in relation to other reviews
Compared to previous studies, our systematic review and meta-analysis has two strengths. First, our review updated the best research evidence for the efficacy of early mobilization in ICU patients. Systematic reviews and meta-analyses [4, 5] have already been published in this regard. However, additional RCTs were performed [23, 24] after those studies; it is therefore necessary to update the current literature. These recent trials were included in the 11 trials evaluated in this study; it therefore provides the best updated evidence.
Second, our review focused on patient-relevant outcomes such as mortality and health-related QOL. The previous review [4] did not include mortality as an outcome during meta-analysis. Another recently published review [3] did not perform meta-analysis for health-related QOL outcomes. Conversely, our review provides results for both, mortality and health-related QOL; these results are therefore more clinically relevant than those from previous reviews.
Interpretation and implications for practice and further research
No apparent differences in in-hospital mortality were noted between the intervention and control groups in our analysis. This may be attributed to the lack of statistical power in detecting the difference, as mortality was relatively low among the eligible patients in the included trials [early mobilization group: 13.7 (64/466) vs. control group: 12.2% (56/458)]. Future research will therefore require considerably larger cohorts to investigate any difference. Our analysis showed early mobilization to be a favorable factor for the length of in-hospital stay and MRC. These findings may provide sufficient evidence to recommend early mobilization in clinical practice. However, the results should be interpreted with caution, as they may be influenced by performance bias owing to a lack of blinding among clinicians. The statistical heterogeneity of in-hospital length of stay in this cohort was substantially high (I2 = 85%). Despite the lack of apparent baseline imbalances in physiological severity, our study population was clinically heterogeneous (i.e., variable settings and medical conditions); this may have influenced the outcome. Heterogeneity was also high for the health-related QOL outcomes (SF-36 PF: I2 = 86%, EQ-5D VAS: I2 = 55%); these may be influenced by a high risk of bias related to performance, detection, and attrition. The risk of performance and detection bias is invariably high in trials of this design; however, the influence of incomplete outcomes can and should be reduced in future research.
Limitations
This study had several limitations. First, we did not include studies written in languages other than English or Japanese. Thus, trials that were otherwise eligible for inclusion may have been overlooked. Second, some of the trials were pilot or feasibility studies; therefore, the individual sample sizes were limited. Further, the number of included trials was limited in terms of the health-related QOL outcomes. This may have led to a lack of power in detecting any differences in effect. Third, the definition of the intervention was clinically heterogeneous. These limitations should be considered while interpreting the study results.
Conclusions
This systematic review and meta-analysis demonstrated no apparent differences between early mobilization and usual care regarding in-hospital mortality and health-related QOL (SF-36PF and EQ-5D VAS) among critically ill patients in the ICU. This suggests that currently available data are inadequate for evaluating the effect of early mobilization on relevant patient outcomes. Larger studies are warranted in the future for detailed evaluation of the effects of early mobilization on in-hospital mortality and health-related QOL in critically ill patients.
Availability of data and materials
Not applicable
Abbreviations
- CI:
-
confidence interval
- EQ-5D:
-
EuroQol 5 Dimension
- ICU:
-
intensive care unit
- ICU-AW:
-
ICU-acquired weakness
- MD:
-
mean difference
- M–H:
-
Mantel–Haenszel method
- MRC:
-
Medical Research Council Scale for Muscle Strength score
- PFIT:
-
the Physical Function in ICU Test
- QOL:
-
quality of life
- RCT:
-
randomized clinical trial
- RR:
-
risk ratio
- SF-36 PF:
-
Short Form Health Survey 36-Item
- SF-36:
-
the Short Form Health Survey 36-Item
- VAS:
-
visual analog scale
References
Devlin JW, Skrobik Y, Gélinas C, Needham DM, Slooter AJC, Pandharipande PP, Watson PL, Weinhouse GL, Nunnally ME, Rochwerg B, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825–73.
Nishida O, Ogura H, Egi M, Fujishima S, Hayashi Y, Iba T, Imaizumi H, Inoue S, Kakihana Y, Kotani J, et al. The Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock 2016 (J-SSCG 2016). J Intensive Care. 2018;6:7.
Zang K, Chen B, Wang M, Chen D, Hui L, Guo S, Ji T, Shang F. The effect of early mobilization in critically ill patients: A meta-analysis. Nurs Crit Care. 0(0).
Fuke R, Hifumi T, Kondo Y, Hatakeyama J, Takei T, Yamakawa K, Inoue S, Nishida O. Early rehabilitation to prevent postintensive care syndrome in patients with critical illness: a systematic review and meta-analysis. BMJ Open. 2018;8(5):e019998.
Tipping CJ, Harrold M, Holland A, Romero L, Nisbet T, Hodgson CL. The effects of active mobilisation and rehabilitation in ICU on mortality and function: a systematic review. In: Intensive Care Med. Volume 43 ed. United States; 2017. p. 171–83.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group atP. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA StatementThe PRISMA Statement. Ann Internal Med. 2009;151(4):264–9.
Jenkinson C, Coulter A, Wright L. Short form 36 (SF36) health survey questionnaire: normative data for adults of working age. Brit Med J. 1993;306(6890):1437–40.
Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, Bonsel G, Badia X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727–36.
van der Ploeg RJO, Oosterhuis HJGH, Reuvekamp J. Measuring muscle strength. J Neurol. 1984;231(4):200–3.
Denehy L, de Morton NA, Skinner EH, Edbrooke L, Haines K, Warrillow S, Berney S. A Physical Function Test for Use in the Intensive Care Unit: Validity, Responsiveness, and Predictive Utility of the Physical Function ICU Test (Scored). Phys Ther. 2013;93(12):1636–45.
Folstein MF, Folstein SE, PR MH. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–98.
Higgins JP. Cochrane handbook for systematic reviews of interventions. Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. wwwcochrane-handbookorg 2011.
Tariq MI, Khan AA, Khalid Z, Farheen H, Siddiqi FA, Amjad I. Effect of Early </= 3 Mets (Metabolic Equivalent of Tasks) of Physical Activity on Patient’s Outcome after Cardiac Surgery. In: J Coll Physicians Surg Pak. Volume 27. Pakistan; 2017. p. 490–4.
Patman S, Sanderson D, Blackmore M. Physiotherapy following cardiac surgery: is it necessary during the intubation period? In: Aust J Physiother. Volume 47. Australia; 2001. p. 7–16.
Pohlman MC, Schweickert WD, Pohlman AS, Nigos C, Pawlik AJ, Esbrook CL, Spears L, Miller M, Franczyk M, Deprizio D, et al. Feasibility of physical and occupational therapy beginning from initiation of mechanical ventilation. Crit Care Med. 2010;38(11):2089–94.
Brummel NE, Girard TD, Ely EW, Pandharipande PP, Morandi A, Hughes CG, Graves AJ, Shintani A, Murphy E, Work B, et al. Feasibility and safety of early combined cognitive and physical therapy for critically ill medical and surgical patients: the Activity and Cognitive Therapy in ICU (ACT-ICU) trial. Intensive Care Med. 2014;40(3):370–9.
Kayambu G, Boots R, Paratz J. Early physical rehabilitation in intensive care patients with sepsis syndromes: a pilot randomised controlled trial. Intensive Care Med. 2015;41(5):865–74.
Morris PE, Berry MJ, Files DC, Thompson JC, Hauser J, Flores L, Dhar S, Chmelo E, Lovato J, Case LD, et al. Standardized Rehabilitation and Hospital Length of Stay Among Patients With Acute Respiratory Failure: A Randomized Clinical Trial. JAMA. 2016;315(24):2694–702.
Moss M, Nordon-Craft A, Malone D, Van Pelt D, Frankel SK, Warner ML, Kriekels W, McNulty M, Fairclough DL, Schenkman M. A Randomized Trial of an Intensive Physical Therapy Program for Patients with Acute Respiratory Failure. Am J Respir Crit Care Med. 2016;193(10):1101–10.
Schaller SJ, Anstey M, Blobner M, Edrich T, Grabitz SD, Gradwohl-Matis I, Heim M, Houle T, Kurth T, Latronico N, et al. Early, goal-directed mobilisation in the surgical intensive care unit: a randomised controlled trial. Lancet. 2016;388(10052):1377–88.
Dong Z, Yu B, Zhang Q, Pei H, Xing J, Fang W, Sun Y, Song Z. Early rehabilitation therapy is beneficial for patients with prolonged mechanical ventilation after coronary artery bypass surgery. Int Heart J. 2016;57(2):241–6.
Hodgson CL, Bailey M, Bellomo R, Berney S, Buhr H, Denehy L, Gabbe B, Harrold M, Higgins A, Iwashyna TJ, et al. A binational multicenter pilot feasibility randomized controlled trial of early goal-directed mobilization in the ICU. Crit Care Med. 2016;44(6):1145–52.
Maffei P, Wiramus S, Bensoussan L, Bienvenu L, Haddad E, Morange S, Fathallah M, Hardwigsen J, Viton JM, Le Treut YP, et al. Intensive early rehabilitation in the intensive care unit for liver transplant recipients: a randomized controlled trial. Arch Phys Med Rehabil. 2017;98(8):1518–25.
Moradian ST, Najafloo M, Mahmoudi H, Ghiasi MS. Early mobilization reduces the atelectasis and pleural effusion in patients undergoing coronary artery bypass graft surgery: a randomized clinical trial. J Vasc Nurs. 2017;35(3):141–5.
Acknowledgements
Not applicable.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
TU, KH, and SI contributed to the conception and design of the review. YO and YM screened the title and abstract for eligible criteria. YO and YE performed the full-text review. YO, YM, YE, and TU extracted the data and assessed the risk of bias. TU managed and integrated the whole review and assessment. TU, KH, and SI supervised the statistical methods. YO prepared the draft of the manuscript. All authors revised the draft critically; approved the contents of the manuscript; and agreed to be accountable for all aspects of the work, including ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The need for ethical approval and consent was waived for this systematic review.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Study protocol
Additional file 2.
Detail of the risk of bias
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Okada, Y., Unoki, T., Matsuishi, Y. et al. Early versus delayed mobilization for in-hospital mortality and health-related quality of life among critically ill patients: a systematic review and meta-analysis. j intensive care 7, 57 (2019). https://doi.org/10.1186/s40560-019-0413-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40560-019-0413-1