
Abstract
Currently, there is a need for diagnostic markers in Lewy body disorders (LBD). α-synuclein (αSyn) RT-QuIC has emerged as a promising assay to detect misfolded αSyn in clinically or neuropathologically established patients with various synucleinopathies. In this study, αSyn RT-QuIC was used to analyze lumbar CSF in a clinical cohort from the Swedish BioFINDER study and postmortem ventricular CSF in a neuropathological cohort from the Arizona Study of Aging and Neurodegenerative Disorders/Brain and Body Donation Program (AZSAND/BBDP). The BioFINDER cohort included 64 PD/PDD, 15 MSA, 15 PSP, 47 controls and two controls who later converted to PD/DLB. The neuropathological cohort included 101 cases with different brain disorders, including LBD and controls. In the BioFINDER cohort αSyn RT-QuIC identified LBD (i.e. PD, PDD and converters) vs. controls with a sensitivity of 95% and a specificity of 83%. The two controls that converted to LBD were αSyn RT-QuIC positive. Within the AZSAND/BBDP cohort, αSyn RT-QuIC identified neuropathologically verified "standard LBD" (i.e. PD, PD with AD and DLB; n = 25) vs. no LB pathology (n = 53) with high sensitivity (100%) and specificity (94%). Only 57% were αSyn RT-QuIC positive in the subgroup with "non-standard" LBD (i.e., AD with Lewy Bodies not meeting criteria for DLB or PD, and incidental LBD, n = 23). Furthermore, αSyn RT-QuIC reliably identified cases with LB pathology in the cortex (97% sensitivity) vs. cases with no LBs or LBs present only in the olfactory bulb (93% specificity). However, the sensitivity was low, only 50%, for cases with LB pathology restricted to the brainstem or amygdala, not affecting the allocortex or neocortex. In conclusion, αSyn RT-QuIC of CSF samples is highly sensitive and specific for identifying cases with clinicopathologically-defined Lewy body disorders and shows a lower sensitivity for non-standard LBD or asymptomatic LBD or in cases with modest LB pathology not affecting the cortex.
Similar content being viewed by others


Introduction
The clinical diagnosis of Parkinson’s disease (PD) can be difficult due to its heterogenous presentation and clinical overlap with atypical parkinsonian disorders, especially early in the disease course. Indeed, the diagnostic accuracy for PD has been found to be as low as 73.8% (67.8–79.6) by non-experts but only slightly better by movement disorders specialist with an accuracy of 79.6% (46–95.1) at the initial assessment, particularly when disease duration is less than 5 years [2, 3, 7, 58]. The differential diagnosis of the atypical parkinsonian disorders, multiple system atrophy (MSA), progressive nuclear palsy (PSP), and corticobasal degeneration (CBD) are even more difficult, with generally acceptable specificity but low sensitivity [38, 45].
There are to date no disease-modifying therapies available in PD. New disease-modifying therapies are likely to be most efficient early on in the disease process, before neuronal damage is irreversible [64]. The lack of clear and reliable biomarkers that can identify individuals with PD has been considered a great barrier to the development of disease-modifying treatments [19]. There is thus an urgent need for early and accurate biomarkers for Parkinson’s disease.
Although results consistently have shown decreased levels of CSF unmodified α-synuclein (α-syn) in PD, but also PD with dementia (PDD), dementia with Lewy bodies (DLB), and MSA compared with controls, the reduction is modest, with a broad overlap with controls, and subsequently has failed to adequately discriminate between PD and controls [33, 51, 53], hampering its usefulness in clinical trials and practice.
Ultrasensitive seed amplification assays are methods originally developed for the detection of misfolded prion proteins and prion-like proteins. Over the last several years αSyn RT-QuIC and related α-syn seed amplification assays have emerged as possible methods for detecting misfolded forms of synuclein in CSF, exploiting the prion-like propagation mechanism of pathological α-syn aggregates. Previous studies have shown a high sensitivity of > 92% for clinicopathologically verified Lewy body disorders (LBD), i.e. PD, PDD and DLB, compared to controls/non-synucleinopathies, and a specificity of > 95% [5, 14, 27, 61]. The diagnostic accuracy has predictably been somewhat lower in clinical cohorts with sensitivity > 93% and specificity > 82% [14, 32, 44, 52, 62]. Among αSyn RT-QuIC assays, there are those with particularly short overall assay times of ~ 1–2 days, without compromising diagnostic performance [18, 32, 52, 57, 60,61,62, 71].
In this study we use a rapid αSyn RT-QuIC assay to test CSF samples from participants with clinically diagnosed PD, PDD, MSA, PSP and controls in the longitudinal Swedish BioFINDER study [34] and participants from a well characterized cohort of neuropathologically-verified cases with different brain disorders including LBD cases and controls from the Arizona Study of Aging and Neurodegenerative Disorders/Brain and Body Donation Program (AZSAND/BBDP) [9]. Previous neuropathological studies have mainly compared "ideal" groups of cases, i.e. controls with no LB disease versus neuropathologically verified and clinically-manifest LBD (“standard LBD”: PD, PDD with Alzheimer’s disease, PDD without AD, and DLB). In this study, we investigated not only individuals with standard LBD and controls, but also those with non-standard LBD (i.e., the cases with Lewy bodies at autopsy but not meeting clinicopathological consensus criteria for DLB or PD), including cases with Alzheimer’s disease with Lewy bodies (ADLB) not meeting criteria for DLB or PD and cases with incidental Lewy body disease (ILBD). Additionally, we investigated CSF αSyn RT-QuIC results in relation to (i) the LB stage, (ii) the LB density and (iii) the LB distribution in ten selected brain regions irrespective of the clinical and neuropathological diagnosis.
Methods
Participants in the BioFINDER cohort
The study was performed at the Clinic of Neurology, Skåne University hospital, Sweden as part of the Swedish BioFINDER Study (www.biofinder.se) [34]. The study participants are primarily recruited from the southern region of Sweden. Patients with PD (n = 50) met the NINDS Diagnostic Criteria for PD [29]. Patients with PDD (n = 14) also met criteria for PDD at baseline [25]. Patients with MSA (n = 15) met the consensus statement by Gilman et al. [30]. Patients with PSP (n = 15) met the criteria according to the report of the National Institute of Neurological Disorders and Stroke–Society for Progressive Supranuclear Palsy International Workshop [47]. All controls (n = 47) underwent cognitive testing and neurologic examination by a medical doctor and individuals with objective cognitive or parkinsonian symptoms were not included. Two individuals initially included as controls converted to clinical LBD during follow-up. One was diagnosed with PD after 5.5 years follow-up and one was diagnosed with DLB after 3.5 years follow-up. Exclusion criteria were i) age above 85 years, ii) presence of generalized malignancy, iii) ongoing or earlier advanced abuse of alcohol or illicit drugs, iv) presence of clinically-diagnosed Alzheimer’s dementia, vascular dementia, frontotemporal lobe dementia, v) presence of severe psychiatric disorders, vi) presence of other severe neurological disease, vii) participation in clinical drug trial within the last 30 days.
All participants gave written informed consent before entering the study. The study procedure was approved by the local ethics committee at Lund University Sweden and conducted according to the Helsinki Declaration.
A thorough medical history was taken and the participants underwent extensive testing. Participants were examined by a physician experienced in movement disorders and a registered research nurse using, among other scales, the Unified Parkinson’s Disease Rating Scale (UPDRS) -3, the Hoehn & Yahr scale and the Mini Mental State Examination (MMSE) [26, 28, 37].
CSF samples were obtained by lumbar puncture in the L3/L4 or L4/L5 interspace with patient non-fasting. The samples were collected in polypropylene tubes and gently mixed to avoid gradient effects.
All samples were centrifuged within 30 min at + 4 °C at 2000 g for 10 min to remove cells and debris, and then stored in aliquots at − 80 °C pending biochemical analysis. The procedure followed the Alzheimer’s Association Flow Chart for CSF biomarkers [13].
Participants in AZSAND/BBDP cohort
The neuropathology cohort consisted of neuropathologically classified participants (n = 101) from the Arizona Study of Aging and Neurodegenerative Disorders (AZSAND), an antemortem-postmortem donor cohort with dates of enrollment from 2007 to 2019. Autopsies were performed by the Banner Sun Health Research Institute Brain and Body Donation program (BBDP) [9, 11].
Neuropathological diagnosis of PD was based on a combination of established neuropathologic criteria [8, 11, 24] and a clinical diagnosis of parkinsonism. DLB diagnosis was defined as a clinical diagnosis of dementia with an intermediate or high likelihood of DLB by the third meeting of the Dementia with Lewy Bodies Consortium [49].
Cases were classified using the Unified Staging System for Lewy Body Disorders (USSLBD) i.e., cases with LBs present were classified into LB stages: I. Olfactory Bulb Only; IIa Brainstem Predominant; IIb Limbic Predominant; III Brainstem and Limbic; IV Neocortical [8]. Lewy Body (LB) density score was assessed in all cases. LB density score is a semi quantitative score of 0–4 in 10 different brain regions (olfactory bulb and tract, medulla at the level of the 9th and 10th cranial nerve nuclei, pons at the level of the locus ceruleus, amygdala, substantia nigra, transentorhinal area, cingulate gyrus at level just posterior to genu of corpus callosum, middle temporal gyrus, middle frontal gyrus, inferior parietal lobule) yielding a maximum score of 40. Neuronal perikaryal cytoplasmic staining, neurites and puncta were considered together, using the templates provided by the Dementia with Lewy Bodies Consortium [49]. The immunohistochemical method used an antibody against phosphorylated synuclein, as previously described[8].
Cases were classified as having PD or DLB, or ILBD (incidental Lewy body disease) in the case of controls without parkinsonism or dementia, when Lewy bodies were present on neuropathological examination but cases did not meet clinicopathological diagnostic criteria for either PD or DLB.
PSP, CBD and MSA were diagnosed according to previously published criteria [22, 23, 31, 36]. Neuropathological diagnosis of AD was based on National Institute on Aging–Reagan Institute (NIA-RI) criteria [1] which are dependent on the Consortium to Establish a Registry for Alzheimer disease (CERAD) neuritic plaque and Braak (neurofibrillary tau-tangle) stage [15]. National Institute on Aging-Alzheimer’s Association criteria[39] were not used due to many cases who had autopsy prior to these newer criteria. The major difference between the two sets of criteria is the addition of Thal amyloid phase to the newer criteria but this may not improve clinicopathological correlations[65]. Controls were cases without dementia or parkinsonism during life and without a major neuropathological diagnosis.
Histopathological scoring was performed blinded to clinical and neuropathological diagnosis. Amyloid plaque and neurofibrillary tangle density were both graded and staged at standard sites in frontal, temporal and parietal lobes and hippocampal CA1 region and entorhinal region using a semi-quantitative score of 0–3 based on the CERAD templates, yielding a total score of 15 [9, 50]. Immunohistochemical staining for phosphorylated TDP-43 was performed in 38 of the 101 cases as previously described [4, 9].
Post mortem CSF was drawn from the lateral ventricles through the corpus callosum prior to removing the brain with precautions taken to minimize contamination. The CSF was then ejected into 15 mL disposable polyethylene tubes. CSF was centrifuged at 2,000 g for 10 min at 24 C and supernatants were aliquoted into 0.5 mL polyethylene microcentrifuge tubes and stored frozen at − 80 °C [9]. Mean post mortem interval was 3.9 (ranging from 2.9–4.9) hours.
Whereas the BioFINDER CSFs were collected from living patients by lumbar puncture, the AZSAND/BBDP CSFs were collected on autopsy from the brain ventricles. Overall comparisons of BioFINDER and AZSAND/BBDP CSFs from PD cases where all replicate reactions were positive indicated that the post-mortem CSFs had slightly higher (22%) mean total protein concentrations, (measured by Pierce Rapid Gold BCA Protein Assay Kit following manufacturer recommendations; ThermoFisher), slightly lower (17%) mean RT-QuIC fluorescence maxima, and slightly longer (15%) mean times to threshold (Additional File 1: Supplemental Fig. 1). However, although these differences in the means are statistically significant, they are small, with large overlaps of the two groups for each of these parameters.
All participants had signed written informed consent. Ethical approval was given by Banner Health-designated Institutional Review Boards; currently the Western Institutional Review Board of Puyallup, Washington.
αSyn RT-QuIC analyses
αSyn RT-QuIC analyses were performed blinded to clinical and neuropathological status and diagnosis of the patient. The preparation of the K23Q recombinant α‐synuclein was done as previously described [63]. The αSyn RT-QuIC analyses was done as previously described [52]. Briefly, reactions were performed in black 96‐well plates with a clear bottom (Nalgene Nunc International). Each well was preloaded with six glass beads (0.8 mm in diameter, OPS Diagnostics). Quadruplicate reactions were seeded with 15 μL of CSF. Prior to the addition of CSF, each RT‐QuIC reaction mix was 85 μL of solution [32] with final reaction concentrations of 40 mM sodium phosphate buffer, 170 mM NaCl, 0.1 mg/mL K23Q recombinant αSyn (filtered through a 100 kD MWCO filter immediately prior to use), 10 μM thioflavin T (ThT) and 0.0015% SDS. The plates were closed with a plate sealer film (Nalgene Nunc International) and incubated at 42 °C in a BMG FLUOstar Omega plate reader for at least 48 h and subjected to cycles of 1 min shaking (400 rpm double orbital) and 1 min rest for at least 48 h. ThT fluorescence measurements (450 ± 10 nm excitation and 480 ± 10 nm emission; bottom read) were taken every 45 min with fluorimeter gain settings adjusted to maintain fluorescence responses within an unsaturated range (in most cases). The fluorescence threshold was calculated individually for each 96‐well plate to account for differences between plate readers. Positive reactions were those exceeding 10% of the maximum value obtained on the same plate from any individual positive reaction. All samples were subjected to a first round of blinded RT-QuIC testing in quadruplicate: samples with 0 positive reactions within 48 h were deemed negative; samples giving 3 or 4 positive wells were considered positive. If samples initially gave 1 or 2 positive wells, most were retested, and, if the number of cumulative positive wells out of the now 8 total replicates was > 25% we called that sample positive; if not, it was deemed negative. However, two CSF samples giving 1 of 4 positive wells in the initial test were not retested due to technical reasons and were deemed negative for the purposes of this study.
Statistical analyses
Mann–Whitney U test was used for comparison of continuous and ordinal variables between groups and chi-square test for dichotomous variables. p < 0.05 (two-sided) was considered statistically significant. Sensitivity and specificity of the αSyn RT-QuIC results were calculated for diagnoses in the clinical BioFINDER cohort and between the presence/absence of any LB pathology, LB stage, LB density score, LB distribution and clinicopathological diagnosis in the AZSAND/BBDP cohort. Univariate associations between two continuous or ordinal variables were analyzed using Spearman ρ. SPSS (version 27; SPSS Inc., Chicago, Illinois) was used for statistical analyses and figures.
Results
Clinical BioFINDER cohort
There were no sex differences between the diagnostic groups and no significant difference between men and women in αSyn RT-QuIC results (Table 1). There was no significant difference in age between αSyn RT-QuIC positive and negative individuals.
CSF αSyn RT-QuIC vs clinical diagnosis
In the clinically diagnosed BioFINDER study, 94% of PD patients and 100% of PDD patients were αSyn RT-QuIC positive compared with 17% (8/47) of controls (not including those who later converted to LBD) and 33% (5/15) of PSP patients. Further, 33% of those with clinically diagnosed MSA (5/15) were αSyn RT-QuIC positive. Interestingly, both individuals who were included as controls but subsequently developed clinically diagnosed LBD (PD and DLB respectively) during follow up had positive αSyn RT-QuIC results.
In this clinical cohort, αSyn RT-QuIC could discriminate between controls and non-demented PD with a sensitivity of 94% (47/50) and specificity of 83%. When including PD, PDD and individuals who later converted to PD, the sensitivity was slightly higher (95%). However, the three αSyn RT-QuIC negative cases had disease duration of ≤ 5 years yielding a sensitivity of 90% for cases with early PD (≤ 5 years), including those who later developed LBD, and 100% in cases with advanced PD, including PDD (> 5) years. Furthermore, αSyn RT-QuIC discriminated between LBD vs. MSA and PSP with a sensitivity of 95% and a specificity of 67%.
AZSAND/BBDP cohort
There was no significant difference between men and women regarding CSF αSyn RT-QuIC results in this neuropathology-based cohort (Table 2). As expected, there was a strong correlation between LB stage and LB density total score (Rs = 0.990, p < 0.001).
CSF αSyn RT-QuIC status by LB stage, AZSAND/BBDP cohort
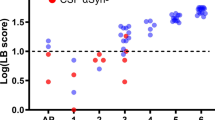
The frequency of αSyn RT-QuIC positive cases in each LB stage are given in Fig. 1. Of the αSyn RT-QuIC positive cases, 93% (38 out of 41) were LB positive (LB stage I-IV) compared to 17% (10 out of 60) cases in the αSyn RT-QuIC negative group (Table 2). Virtually all of those in LB stage III-IV were αSyn RT-QuIC positive (28 out of 29) and in LB stage 0–1 most were negative (52 out of 56); yielding a sensitivity of 97% and specificity of 93% when comparing LB stage III-IV vs LB stage 0–1 (Table 2; Fig. 1). 2/3 with olfactory bulb only (LB stage I) were αSyn RT-QuIC negative and including LB stage 0 only, the specificity was 94%. However, the sensitivity for detecting LB pathology in stage IIa-IIb was only 56% (9 out of 16). None of the cases with stage IIa-IIb had a clinicopathological diagnosis of PD or DLB. None of the 9 αSyn RT-QuIC positive cases had a parkinsonian clinical diagnosis and although the 16 cases with LB stage IIa-IIb had a mean UPDRS motor score of 16.4 (SD 21.9) there was no significant difference between αSyn RT-QuIC positive and negative cases. Of note is that the single LB stage III case that was αSyn RT-QuIC negative had a relatively low LB density score of 9 compared to a mean of 23.5 (SD 5.1) in all cases with LB stage III.

Stacked bar chart depicting αSyn RT-QuIC status by LB stage in the neuropathology-based AZSAND/BBDP cohort. 97% of the cases with LB stage III-IV were αSyn RT-QuIC positive and 93% of the cases in LB stage 0–1 were αSyn RT-QuIC negative. However, only 56% of cases with LB pathology in stage IIa-IIb were αSyn RT-QuIC positive
CSF αSyn RT-QuIC status by LB distribution, AZSAND/BBDP cohort
When comparing the CSF αSyn RT-QuIC results more directly to the distribution of LB pathology in the brain we found that 30/31 (97%) of cases with LB pathology in the cortex (allocortex and/or neocortex) were αSyn RT-QuIC positive (Fig. 2). The one αSyn RT-QuIC-negative case with cortical LBs was at the LB stage IIb and had a LB density score of only 1 in the cingulum (due to one single LB) and no other cortical involvement. Of the 14 cases with LB pathology in the brainstem and/or amygdala, but with no cortical involvement, 50% were αSyn RT-QuIC positive. (Fig. 2). We next subdivided these 14 cases further into brainstem only (n = 2), amygdala only (n = 7) or those with LB pathology restricted to both brain stem and amygdala (n = 5). We found that 2 out of 2 "brainstem only" were negative, 2 out of 7 "amygdala only" were negative, and 3 out of 5 with "LB pathology restricted to both amygdala and brainstem" were negative.

Stacked bar chart depicting αSyn RT-QuIC status by LB distribution in the neuropathology-based AZSAND/BBDP cohort. 97% of cases with LB pathology in the cortex (allocortex and/or neocortex) were αSyn RT-QuIC positive whereas 93% of cases with no LBs or LB restricted to the olfactory bulb only were αSyn RT-QuIC negative. Of the cases with LB pathology in the brainstem and/or amygdala, but with no cortical involvement, 50% were αSyn RT-QuIC positive
CSF αSyn RT-QuIC status by LB density, AZSAND/BBDP cohort
When using the total LB density score (established by summing the regional density scores from the ten predefined regions), the αSyn RT-QuIC negative cases had significantly lower LB density compared with αSyn RT-QuIC positive cases (p < 0.001) (Table 2). αSyn RT-QuIC identified cases with total LB density score > 10 with a sensitivity of 97% (29 out of 30 were positive) and cases with total LB density score 0–4 with a specificity of 93% (55 out of 59 were negative). Of the cases with an intermediate LB density score of 5–10, however, only 64% (7 out of 11) were αSyn RT-QuIC positive (Fig. 3).

Stacked bar chart depicting αSyn RT-QuIC status by LB density in the neuropathology-based AZSAND/BBDP cohort. 97% of cases with total LB density score > 10 score (established by summing the regional density scores from the ten predefined regions yielding a maximum score of 40) were αSyn RT-QuIC positive. 93% of cases with total LB density score of 0–4 were αSyn RT-QuIC negative. Only 64% of cases with an intermediate LB density score of 5–10 were αSyn RT-QuIC positive
CSF αSyn RT-QuIC by clinicopathological diagnosis, AZSAND/BBDP cohort
CSF αSyn RT-QuIC identified neuropathologically verified "standard LBD" (i.e. PD, PDAD and DLB with AD; n = 25) vs. no LB pathology (n = 53) with high sensitivity (100%) and specificity (94%). αSyn RT-QuIC thus correctly identified all clinicopathologically confirmed cases with standard LBD. It is worth noting that all 4 cases with DLB also met criteria for AD. In cases with atypical parkinsonian syndromes, i.e. PSP (n = 5), CBS (n = 1) and MSA (n = 1), 6 out 7 were negative. The one αSyn RT-QuIC positive individual with an atypical parkinsonian syndrome had clinicopathological PSP with no evident LBs. It is also worth noting that the one case with neuropathologically confirmed MSA did not have any LB pathology and was αSyn RT-QuIC negative (Table 3).
Of cases with "non-standard LBD" (i.e., AD with Lewy Bodies not meeting criteria for DLB or PD, and ILBD, n = 23), only 57% cases were αSyn RT-QuIC positive (Table 3). αSyn RT-QuIC positive cases with non-standard LBD did not have significantly higher LB stage (p = 0.174) (Table 4) or higher LB density (p = 0.152) compared to αSyn RT-QuIC negative cases. There was no significant difference in LB density in any of the 10 measured brain regions between αSyn RT-QuIC positive and negative cases with "non-standard LBD". Further, there was no difference in UPDRS motor score or MMSE between αSyn RT-QuIC positive and negative cases with "non-standard LBD" (p = 0.755, p = 0.686 respectively).
CSF αSyn RT-QuIC versus amyloid-β, tau and TDP-43 pathological changes, AZSAND/BBDP cohort
There were no significant differences in total amyloid-β plaque density score or total neurofibrillary tangle density score between αSyn RT-QuIC positive and negative cases. Further, there was no significant difference between the presence/absence of TDP-43 pathology between to αSyn RT-QuIC positive and negative cases (Table 2).
Discussion
In this study we describe αSyn RT-QuIC testing of CSF from both a clinical cohort and a neuropathological cohort from a longitudinal clinicopathological study. Previous neuropathological studies with αSyn RT-QuIC of CSF have mainly investigated verified clinicopathological diagnoses with LBD vs. cases with no LBD, finding a high diagnostic accuracy in this setting [5, 14, 61], which we can confirm. In the present study we also investigated cases with “non-standard LBD”, i.e. those cases with neuropathological findings of LBD but not meeting criteria for PD or DLB. We found that CSF αSyn RT-QuIC reliably identified cases with LB stage III-IV (Fig. 1), cases with LB disease with cortical involvement (Fig. 2) and cases with high LB brain loads (Fig. 3) and distinguished these from cases with low LB density and no LBs with a high accuracy. However, the sensitivity was less robust when investigating cases with modest LB pathology, defined either as i) low LB stage (IIa-IIb), or ii) limited spread of LBs restricted to the brainstem or amygdala, or iii) intermediate LB brain loads (56%, 50% and 64% respectively), but the number of cases were relatively small.
The diagnostic accuracy was very high for neuropathologically verified cases with standard LB disease vs. cases with no LBs at all with a sensitivity of 100% and a specificity of 94%, which is consistent with previous results [5, 14, 27, 61]. However, in parallel to the results with lower diagnostic accuracy for cases with intermediate LB density or limited spread of LBs, the diagnostic accuracy was also lower in cases with "non-standard LBD", with 57% being αSyn RT-QuIC positive. This is partially in line with the exploratory results by Fairfoul et al. who found up to 31% αSyn RT-QuIC positivity in AD cases with incidental LB, however the number (n = 13) with non-standard LBD in that study was low [27]. In the present study, the αSyn RT-QuIC positive cases with "non-standard LBD" did not have significantly higher LB stage or LB density compared to the αSyn RT-QuIC negative cases with "non-standard LBD". Further, there was no significant difference in LB density in any of the 10 different brain regions in αSyn RT-QuIC positive cases vs. αSyn RT-QuIC negative cases in the "non-standard LBD group". It is therefore not possible to speculate, in this cohort, whether the αSyn RT-QuIC positive cases with "non-standard LBD" would have been at higher risk of developing clinical Lewy body disease. However, there might be a threshold effect, where these cases are close to the threshold of αSyn RT-QuIC detection, yielding a higher variability in the result. This is likely a result of lower total brain (and CSF) load of a-syn seeds in this group of cases with less widespread LB pathology seldom affecting the cortex. Further, the semiquantitative method of obtaining LB regional density score allows for some variability in density scoring. An alternative, but less likely and speculative, explanation is that the α-syn seeds present in the cortex are more prone to induce aggregation of monomeric α-syn.
The presence of more than one pathology is prevalent in neurodegenerative disorders [10, 41, 59] and Aβ and tau pathologies may act synergistically with αSyn pathology influencing the clinical presentation and prognosis in LBD [43]. Further, misfolded αSyn might potentiate aggregation of tau [6, 56]. However, the CSF αSyn RT-QuIC assay could in the present study specifically identify LB pathology without any associations to the load of Aβ, tau or TDP-43 pathology changes, although the number of cases investigated for TDP-43 pathology was low.
In the clinical BioFINDER cohort, we found a high sensitivity (95%) for αSyn RT-QuIC in LBD. However, the specificity in the present study was 83%, which is lower compared to previous results [32, 61]. One can speculate that the lower specificity in the clinical cohort reflects the fact that some of the individuals included as controls could have ILBD, although the present rate would be higher than expected. Supporting the possibility that at least some of these αSyn RT-QuIC positive controls were ILBD is the documented later clinical conversion of two αSyn RT-QuIC positive controls to PD or DLB. The high rate of αSyn RT-QuIC positive controls could also be due to a high sensitivity of the analyses for ILBD; this is, however, at odds with results in the neuropathological AZSAND/BBDP cohort with a low specificity for individuals with ILBD. An alternative explanation could be an increased proclivity for ILBD than expected in the clinical BioFINDER cohort. The controls in the present study were mainly spouses or in some cases 1st degree relatives of individuals with PD (mostly) or atypical parkinsonian disorders. There were, however, no significant differences in the proportions of αSyn RT-QuIC-positive and negative BioFINDER controls that had spouses or 1st degree relatives with LBD. None of the αSyn RT-QuIC positive controls had 1st degree relatives with LBD but one of the αSyn RT-QuIC positive controls that converted to LBD had a sibling with PD.
In our study, 33% of clinical MSA were αSyn RT-QuIC positive and 0/1 of the neuropathologically confirmed cases with verified MSA was αSyn RT-QuIC positive. This is in line with previous studies [61, 70]. It has been proposed that this is due to a different strain of α-syn in MSA [54, 55, 69], yielding a different kinetic profile [66], or no aggregation at all [61], in different αSyn seed amplification assays. Our assay was developed for the detection of seeds of Lewy body disorders rather than MSA, and others have shown better detection of MSA-associated seeds using alternative amplification conditions [48, 62]. The low specificity could also be attributed to clinical misdiagnosis or concomitant LB pathology in MSA[46].
Perhaps more surprising is our low specificity in PSP cases (67%) in the clinical BioFINDER cohort. In our hands, one of the positive PSP samples from the clinical cohort gave 4/4 and one 3/4 positive replicate wells and the others gave 3/8 positive replicate wells. In the 47 positive PD cases, 41 gave 4/4 positive replicate wells, four gave 3/4, one gave 3/8 and one 6/8. All 14 PDD gave 4/4 positive replicate wells. We did not observe any significant difference in the fluorescence intensity in PSP compared to the PD CSF samples. Clinical diagnoses are difficult and inherently uncertain, especially for atypical parkinsonian syndromes and it is possible that the low specificity in the present study may be due to clinical misdiagnoses. However, there were was no significant differences in disease duration, UPDRS motor score, Hoehn & Yahr score, age or sex (data not shown) between the αSyn RT-QuIC positive and negative PSP patients. The presence of multiple pathologies is relatively common in neurodegenerative disorders [42, 59] and the high positivity rate in the clinically diagnosed PSP participants could possibly in part be due to LBD-copathology. This makes the inclusion of a cohort of neuropathologically confirmed cases in the present study all the more important. In clinicopathological cases with PSP, CBD, or MSA we found all but one case to be αSyn RT-QuIC negative; however, the total case number was small.
Given the results in the present study with a very low diagnostic accuracy in cases with relatively low LB load in the neuropathological AZSAND/BBDP cohort (defined as either “non-standard LBD”, intermediate LB density or limited spread of LB pathology), one could speculate that αSyn RT-QuIC analysis of post mortem ventricular CSF has a lower sensitivity for detecting LBD compared with in vivo lumbar CSF with a high sensitivity for clinical LBD. It has been stated that lumbar CSF has significant differences from ventricular CSF but this has been refuted in several articles [16, 17, 35, 67]. It is worth noting that none of the cases with limited spread of LB pathology (stage IIa-IIb) had a clinicopathological diagnosis of PD or DLB, and all clinicopathological PD and DLB cases had LB stage III-IV with at least some cortical LBs. One previous study investigating the neuropathological findings by PD subtype found that 85% of the total cases and 89% of cases with mild-motor predominant PD reached the neocortical stage [20]. It is thus reasonable to assume that most of the clinical, symptomatic LBD cases in the clinical BioFINDER study have LB pathology spread beyond the brainstem and those results are thus not comparable to the results from post mortem ILBD [20, 21]. However, the three αSyn RT-QuIC negative PD cases in the clinical BioFINDER study all had disease duration of ≤ 5 years and it is possible that these had less spread disease, although this is at odds with the αSyn RT-QuIC positive result in the two asymptomatic individuals who converted to LBD. Therefore, based on the results of the present study, it is not possible to say that ventricular CSF is less sensitive compared to lumbar CSF to detect ILBD or cases with relatively low LB load or disease restricted to the brainstem.
Overall, CSF αSyn RT-QuIC has become a promising biomarker assay for the diagnosis of PD and DLB that may vastly improve the diagnostic work up in these patients, but may not greatly improve the detection of individuals at the very earliest stages of the disease. Still, several studies have shown a high sensitivity for αSyn seed amplification assays in prodromal cases [40, 60, 61, 68]. Isolated rapid-eye-movement sleep behavior disorder (iRBD) is a common non-motor symptom in LBD and also a common prodromal symptom of LBD [12]. In a recent longitudinal study on patients with iRBD, 62% converted to PD or DLB during follow-up, of whom 97% were CSF αSyn RT-QuIC positive [40]. In the present study, αSyn RT-QuIC positivity was seen up to 5.5 years prior to diagnosis of the two individuals who later developed LBD in the clinical cohort. However, further longitudinal studies are needed to clarify how early in the pre-symptomatic and prodromal phases individuals with early LBD convert to αSyn RT-QuIC positivity in CSF.
The possibility of accurate pre-symptomatic or prodromal diagnosis is especially relevant in coming trials on disease modifying therapies, as these are most likely to be effective if initiated early on in the disease course. αSyn RT-QuIC may be a useful test for at risk iRBD individuals in clinical drug trials to monitor the effect of disease modifying therapies initiated at an early stage.
A limitation to the present study is the lack of neuropathological data in the clinical cohort. However, we also studied αSyn RT-QuIC in a neuropathological cohort which strengthens the results. Further, participants in the clinical cohort are followed over time to ascertain as certain a diagnosis as possible. Indeed, the three αSyn RT-QuIC negative individuals clinical PD diagnosis were followed for 2–5 years in the study, showing typical features for PD including Levo-dopa response but were nonetheless early PD with a disease duration of ≤ 5 years.
In conclusion, the present study confirms that αSyn RT-QuIC has excellent sensitivity and specificity for cases with clinicopathologically verified LB disorders vs those with no LB pathological changes. However, the diagnostic accuracy was poor for cases with LB pathology restricted to non-cortical areas and having an overall low-to-intermediate LB brain load. Further studies are needed to investigate what factors influence αSyn RT-QuIC results in these cases with more limited LB pathological changes and determine at what timepoint in the pre-symptomatic or prodromal stages of LBD that the αSyn RT-QuIC result converts from sub-threshold to clear positivity.
Availability of data materials
Anonymized data will be shared by request from a qualified academic investigator for the sole purpose of replicating procedures and results presented in the article and as long as data transfer is in agreement with legislation on the general data protection regulation and decisions by the respective Ethical Review Boards, which should be regulated in a material transfer agreement.
References
(1997) Consensus recommendations for the postmortem diagnosis of Alzheimer's disease. The National Institute on Aging, and Reagan Institute Working Group on Diagnostic Criteria for the Neuropathological Assessment of Alzheimer's Disease. Neurobiol Aging 18: S1–2
Adler CH, Beach TG, Hentz JG, Shill HA, Caviness JN, Driver-Dunckley E et al (2014) Low clinical diagnostic accuracy of early vs advanced Parkinson disease: clinicopathologic study. Neurology 83:406–412. https://doi.org/10.1212/WNL.0000000000000641
Adler CH, Beach TG, Zhang N, Shill HA, Driver-Dunckley E, Mehta SH et al (2021) Clinical diagnostic accuracy of early/advanced parkinson disease: an updated clinicopathologic study. Neurol Clin Pract 11:e414–e421. https://doi.org/10.1212/CPJ.0000000000001016
Arnold SJ, Dugger BN, Beach TG (2013) TDP-43 deposition in prospectively followed, cognitively normal elderly individuals: correlation with argyrophilic grains but not other concomitant pathologies. Acta Neuropathol 126:51–57. https://doi.org/10.1007/s00401-013-1110-0
Bargar C, Wang W, Gunzler SA, LeFevre A, Wang Z, Lerner AJ et al (2021) Streamlined alpha-synuclein RT-QuIC assay for various biospecimens in Parkinson’s disease and dementia with Lewy bodies. Acta Neuropathol Commun 9:62. https://doi.org/10.1186/s40478-021-01175-w
Bassil F, Meymand ES, Brown HJ, Xu H, Cox TO, Pattabhiraman S et al (2021) alpha-Synuclein modulates tau spreading in mouse brains. J Exp Med. https://doi.org/10.1084/jem.20192193
Beach TG, Adler CH (2018) Importance of low diagnostic Accuracy for early Parkinson’s disease. Mov Disord 33:1551–1554. https://doi.org/10.1002/mds.27485
Beach TG, Adler CH, Lue L, Sue LI, Bachalakuri J, Henry-Watson J et al (2009) Unified staging system for Lewy body disorders: correlation with nigrostriatal degeneration, cognitive impairment and motor dysfunction. Acta Neuropathol 117:613–634. https://doi.org/10.1007/s00401-009-0538-8
Beach TG, Adler CH, Sue LI, Serrano G, Shill HA, Walker DG et al (2015) Arizona study of aging and neurodegenerative disorders and brain and body donation program. Neuropathology 35:354–389. https://doi.org/10.1111/neup.12189
Beach TG, Malek-Ahmadi M (2021) Alzheimer’s Disease neuropathological comorbidities are common in the younger-old. J Alzheimers Dis 79:389–400. https://doi.org/10.3233/JAD-201213
Beach TG, Sue LI, Walker DG, Roher AE, Lue L, Vedders L et al (2008) The sun health research institute brain donation program: description and experience, 1987–2007. Cell Tissue Bank 9:229–245. https://doi.org/10.1007/s10561-008-9067-2
Berg D, Postuma RB, Adler CH, Bloem BR, Chan P, Dubois B et al (2015) MDS research criteria for prodromal Parkinson’s disease. Mov Disord 30:1600–1611. https://doi.org/10.1002/mds.26431
Blennow K, Hampel H, Weiner M, Zetterberg H (2010) Cerebrospinal fluid and plasma biomarkers in Alzheimer disease. Nat Rev Neurol 6:131–144. https://doi.org/10.1038/nrneurol.2010.4
Bongianni M, Ladogana A, Capaldi S, Klotz S, Baiardi S, Cagnin A et al (2019) alpha-Synuclein RT-QuIC assay in cerebrospinal fluid of patients with dementia with Lewy bodies. Ann Clin Transl Neurol 6:2120–2126. https://doi.org/10.1002/acn3.50897
Braak H, Braak E (1991) Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol 82:239–259. https://doi.org/10.1007/BF00308809
Brandner S, Thaler C, Lelental N, Buchfelder M, Kleindienst A, Maler JM et al (2014) Ventricular and lumbar cerebrospinal fluid concentrations of Alzheimer’s disease biomarkers in patients with normal pressure hydrocephalus and posttraumatic hydrocephalus. J Alzheimers Dis 41:1057–1062. https://doi.org/10.3233/JAD-132708
Brandner S, Thaler C, Lewczuk P, Lelental N, Buchfelder M, Kleindienst A (2013) Neuroprotein dynamics in the cerebrospinal fluid: intraindividual concomitant ventricular and lumbar measurements. Eur Neurol 70:189–194. https://doi.org/10.1159/000352032
Brockmann K, Quadalti C, Lerche S, Rossi M, Wurster I, Baiardi S et al (2021) Association between CSF alpha-synuclein seeding activity and genetic status in Parkinson’s disease and dementia with Lewy bodies. Acta Neuropathol Commun 9:175. https://doi.org/10.1186/s40478-021-01276-6
Chen-Plotkin AS, Albin R, Alcalay R, Babcock D, Bajaj V, Bowman D et al (2018) Finding useful biomarkers for Parkinson’s disease. Sci Transl Med. https://doi.org/10.1126/scitranslmed.aam6003
De Pablo-Fernandez E, Lees AJ, Holton JL, Warner TT (2019) Prognosis and neuropathologic correlation of clinical subtypes of parkinson disease. JAMA Neurol 76:470–479. https://doi.org/10.1001/jamaneurol.2018.4377
Dickson DW (2018) Neuropathology of Parkinson disease. Parkinsonism Relat Disord 46(Suppl 1):S30–S33. https://doi.org/10.1016/j.parkreldis.2017.07.033
Dickson DW (2012) Parkinson’s disease and parkinsonism: neuropathology. Cold Spring Harb Perspect Med. https://doi.org/10.1101/cshperspect.a009258
Dickson DW, Bergeron C, Chin SS, Duyckaerts C, Horoupian D, Ikeda K et al (2002) Office of rare diseases neuropathologic criteria for corticobasal degeneration. J Neuropathol Exp Neurol 61:935–946. https://doi.org/10.1093/jnen/61.11.935
Dickson DW, Braak H, Duda JE, Duyckaerts C, Gasser T, Halliday GM et al (2009) Neuropathological assessment of Parkinson’s disease: refining the diagnostic criteria. Lancet Neurol 8:1150–1157. https://doi.org/10.1016/S1474-4422(09)70238-8
Emre M, Aarsland D, Brown R, Burn DJ, Duyckaerts C, Mizuno Y et al (2007) Clinical diagnostic criteria for dementia associated with Parkinson's disease. Movement Disorders: official journal of the Movement Disorder Society 22: 1689–1707; quiz 1837 Doi https://doi.org/10.1002/mds.21507
Fahn S ER (1987) UPDRS Program Members. Unified Parkinson's disease rating scale. In: Fahn S, Marsden CD, Goldstein M, Calne DB (ed) Recent Developments in Parkinson's Disease. Florham Park, NJ: Macmillan Healthcare Information, pp 153–163
Fairfoul G, McGuire LI, Pal S, Ironside JW, Neumann J, Christie S et al (2016) Alpha-synuclein RT-QuIC in the CSF of patients with alpha-synucleinopathies. Ann Clin Transl Neurol 3:812–818. https://doi.org/10.1002/acn3.338
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198
Gelb DJ, Oliver E, Gilman S (1999) Diagnostic criteria for Parkinson disease. Arch Neurol 56:33–39
Gilman S, Low PA, Quinn N, Albanese A, Ben-Shlomo Y, Fowler CJ et al (1999) Consensus statement on the diagnosis of multiple system atrophy. J Neurol Sci 163:94–98
Gilman S, Wenning GK, Low PA, Brooks DJ, Mathias CJ, Trojanowski JQ et al (2008) Second consensus statement on the diagnosis of multiple system atrophy. Neurology 71:670–676. https://doi.org/10.1212/01.wnl.0000324625.00404.15
Groveman BR, Orru CD, Hughson AG, Raymond LD, Zanusso G, Ghetti B et al (2018) Rapid and ultra-sensitive quantitation of disease-associated alpha-synuclein seeds in brain and cerebrospinal fluid by alphaSyn RT-QuIC. Acta Neuropathol Commun 6:7. https://doi.org/10.1186/s40478-018-0508-2
Hall S, Ohrfelt A, Constantinescu R, Andreasson U, Surova Y, Bostrom F et al (2012) Accuracy of a panel of 5 cerebrospinal fluid biomarkers in the differential diagnosis of patients with dementia and/or parkinsonian disorders. Arch Neurol 69:1445–1452. https://doi.org/10.1001/archneurol.2012.1654
Hall S, Surova Y, Ohrfelt A, Zetterberg H, Lindqvist D, Hansson O (2015) CSF biomarkers and clinical progression of Parkinson disease. Neurology 84:57–63. https://doi.org/10.1212/WNL.0000000000001098
Hansson O, Mikulskis A, Fagan AM, Teunissen C, Zetterberg H, Vanderstichele H et al (2018) The impact of preanalytical variables on measuring cerebrospinal fluid biomarkers for Alzheimer’s disease diagnosis: a review. Alzheimers Dement 14:1313–1333. https://doi.org/10.1016/j.jalz.2018.05.008
Hauw JJ, Daniel SE, Dickson D, Horoupian DS, Jellinger K, Lantos PL et al (1994) Preliminary NINDS neuropathologic criteria for Steele-Richardson-Olszewski syndrome (progressive supranuclear palsy). Neurology 44:2015–2019. https://doi.org/10.1212/wnl.44.11.2015
Hoehn MM, Yahr MD (1967) Parkinsonism: onset, progression and mortality. Neurology 17:427–442
Hoglinger GU, Respondek G, Stamelou M, Kurz C, Josephs KA, Lang AE et al (2017) Clinical diagnosis of progressive supranuclear palsy: the movement disorder society criteria. Mov Disord 32:853–864. https://doi.org/10.1002/mds.26987
Hyman BT, Phelps CH, Beach TG, Bigio EH, Cairns NJ, Carrillo MC et al (2012) National Institute on Aging-Alzheimer’s Association guidelines for the neuropathologic assessment of Alzheimer’s disease. Alzheimers Dement 8:1–13. https://doi.org/10.1016/j.jalz.2011.10.007
Iranzo A, Fairfoul G, Ayudhaya ACN, Serradell M, Gelpi E, Vilaseca I et al (2021) Detection of alpha-synuclein in CSF by RT-QuIC in patients with isolated rapid-eye-movement sleep behaviour disorder: a longitudinal observational study. Lancet Neurol 20:203–212. https://doi.org/10.1016/S1474-4422(20)30449-X
Irwin DJ, Grossman M, Weintraub D, Hurtig HI, Duda JE, Xie SX et al (2017) Neuropathological and genetic correlates of survival and dementia onset in synucleinopathies: a retrospective analysis. Lancet Neurol 16:55–65. https://doi.org/10.1016/S1474-4422(16)30291-5
Jecmenica Lukic M, Kurz C, Respondek G, Grau-Rivera O, Compta Y, Gelpi E et al (2020) Copathology in progressive supranuclear palsy: does it matter? Mov Disord 35:984–993. https://doi.org/10.1002/mds.28011
Jellinger KA (2018) Dementia with Lewy bodies and Parkinson’s disease-dementia: current concepts and controversies. J Neural Transm (Vienna) 125:615–650. https://doi.org/10.1007/s00702-017-1821-9
Kang UJ, Boehme AK, Fairfoul G, Shahnawaz M, Ma TC, Hutten SJ et al (2019) Comparative study of cerebrospinal fluid alpha-synuclein seeding aggregation assays for diagnosis of Parkinson’s disease. Mov Disord 34:536–544. https://doi.org/10.1002/mds.27646
Koga S, Aoki N, Uitti RJ, van Gerpen JA, Cheshire WP, Josephs KA et al (2015) When DLB, PD, and PSP masquerade as MSA: an autopsy study of 134 patients. Neurology 85:404–412. https://doi.org/10.1212/WNL.0000000000001807
Koga S, Li F, Zhao N, Roemer SF, Ferman TJ, Wernick AI et al (2020) Clinicopathologic and genetic features of multiple system atrophy with Lewy body disease. Brain Pathol 30:766–778. https://doi.org/10.1111/bpa.12839
Litvan I, Agid Y, Calne D, Campbell G, Dubois B, Duvoisin RC et al (1996) Clinical research criteria for the diagnosis of progressive supranuclear palsy (Steele-Richardson-Olszewski syndrome): report of the NINDS-SPSP international workshop. Neurology 47:1–9
Martinez-Valbuena I, Visanji NP, Kim A, Lau HHC, So RWL, Alshimemeri S et al (2022) Alpha-synuclein seeding shows a wide heterogeneity in multiple system atrophy. Transl Neurodegener 11:7. https://doi.org/10.1186/s40035-022-00283-4
McKeith IG, Dickson DW, Lowe J, Emre M, O’Brien JT, Feldman H et al (2005) Diagnosis and management of dementia with Lewy bodies: third report of the DLB Consortium. Neurology 65:1863–1872. https://doi.org/10.1212/01.wnl.0000187889.17253.b1
Mirra SS, Heyman A, McKeel D, Sumi SM, Crain BJ, Brownlee LM et al (1991) The consortium to establish a registry for alzheimer’s disease (CERAD). Part II. Standardization of the neuropathologic assessment of Alzheimer’s disease. Neurology 41:479–486. https://doi.org/10.1212/wnl.41.4.479
Mollenhauer B, Locascio JJ, Schulz-Schaeffer W, Sixel-Doring F, Trenkwalder C, Schlossmacher MG (2011) alpha-Synuclein and tau concentrations in cerebrospinal fluid of patients presenting with parkinsonism: a cohort study. Lancet Neurol 10:230–240. https://doi.org/10.1016/S1474-4422(11)70014-X
Orru CD, Ma TC, Hughson AG, Groveman BR, Srivastava A, Galasko D et al (2021) A rapid alpha-synuclein seed assay of Parkinson’s disease CSF panel shows high diagnostic accuracy. Ann Clin Transl Neurol 8:374–384. https://doi.org/10.1002/acn3.51280
Parnetti L, Gaetani L, Eusebi P, Paciotti S, Hansson O, El-Agnaf O et al (2019) CSF and blood biomarkers for Parkinson’s disease. Lancet Neurol 18:573–586. https://doi.org/10.1016/S1474-4422(19)30024-9
Peelaerts W, Bousset L, Baekelandt V, Melki R (2018) a-Synuclein strains and seeding in Parkinson’s disease, incidental Lewy body disease, dementia with Lewy bodies and multiple system atrophy: similarities and differences. Cell Tissue Res 373:195–212. https://doi.org/10.1007/s00441-018-2839-5
Peng C, Gathagan RJ, Covell DJ, Medellin C, Stieber A, Robinson JL et al (2018) Cellular milieu imparts distinct pathological alpha-synuclein strains in alpha-synucleinopathies. Nature 557:558–563. https://doi.org/10.1038/s41586-018-0104-4
Peng C, Trojanowski JQ, Lee VM (2020) Protein transmission in neurodegenerative disease. Nat Rev Neurol 16:199–212. https://doi.org/10.1038/s41582-020-0333-7
Perra D, Bongianni M, Novi G, Janes F, Bessi V, Capaldi S et al (2021) Alpha-synuclein seeds in olfactory mucosa and cerebrospinal fluid of patients with dementia with Lewy bodies. Brain Commun 3: fcab045, https://doi.org/10.1093/braincomms/fcab045
Rizzo G, Copetti M, Arcuti S, Martino D, Fontana A, Logroscino G (2016) Accuracy of clinical diagnosis of Parkinson disease: a systematic review and meta-analysis. Neurology 86:566–576. https://doi.org/10.1212/WNL.0000000000002350
Robinson JL, Lee EB, Xie SX, Rennert L, Suh E, Bredenberg C et al (2018) Neurodegenerative disease concomitant proteinopathies are prevalent, age-related and APOE4-associated. Brain 141:2181–2193. https://doi.org/10.1093/brain/awy146
Rossi M, Baiardi S, Teunissen CE, Quadalti C, van de Beek M, Mammana A et al (2021) Diagnostic value of the CSF alpha-synuclein real-time quaking-induced conversion assay at the prodromal MCI stage of dementia with lewy bodies. Neurology 97:e930–e940. https://doi.org/10.1212/WNL.0000000000012438
Rossi M, Candelise N, Baiardi S, Capellari S, Giannini G, Orru CD et al (2020) Ultrasensitive RT-QuIC assay with high sensitivity and specificity for Lewy body-associated synucleinopathies. Acta Neuropathol 140:49–62. https://doi.org/10.1007/s00401-020-02160-8
Russo MJ, Orru CD, Concha-Marambio L, Giaisi S, Groveman BR, Farris CM et al (2021) High diagnostic performance of independent alpha-synuclein seed amplification assays for detection of early Parkinson’s disease. Acta Neuropathol Commun 9:179. https://doi.org/10.1186/s40478-021-01282-8
Saijo E, Groveman BR, Kraus A, Metrick M, Orru CD, Hughson AG et al (2019) Ultrasensitive RT-QuIC seed amplification assays for disease-associated tau, alpha-synuclein, and prion aggregates. Methods Mol Biol 1873:19–37. https://doi.org/10.1007/978-1-4939-8820-4_2
Schapira AH (2009) Molecular and clinical pathways to neuroprotection of dopaminergic drugs in Parkinson disease. Neurology 72:S44-50. https://doi.org/10.1212/WNL.0b013e3181990438
Serrano-Pozo A, Qian J, Muzikansky A, Monsell SE, Montine TJ, Frosch MP et al (2016) Thal amyloid stages do not significantly impact the correlation between neuropathological change and cognition in the alzheimer disease continuum. J Neuropathol Exp Neurol 75:516–526. https://doi.org/10.1093/jnen/nlw026
Shahnawaz M, Mukherjee A, Pritzkow S, Mendez N, Rabadia P, Liu X et al (2020) Discriminating alpha-synuclein strains in Parkinson’s disease and multiple system atrophy. Nature 578:273–277. https://doi.org/10.1038/s41586-020-1984-7
Simonsen AH, Bech S, Laursen I, Salvesen L, Winge K, Waldemar G et al (2010) Proteomic investigations of the ventriculo-lumbar gradient in human CSF. J Neurosci Methods 191:244–248. https://doi.org/10.1016/j.jneumeth.2010.06.017
Singer W, Schmeichel AM, Shahnawaz M, Schmelzer JD, Sletten DM, Gehrking TL et al (2021) Alpha-synuclein oligomers and neurofilament light chain predict phenoconversion of pure autonomic failure. Ann Neurol 89:1212–1220. https://doi.org/10.1002/ana.26089
Van der Perren A, Gelders G, Fenyi A, Bousset L, Brito F, Peelaerts W et al (2020) The structural differences between patient-derived alpha-synuclein strains dictate characteristics of Parkinson’s disease, multiple system atrophy and dementia with Lewy bodies. Acta Neuropathol 139:977–1000. https://doi.org/10.1007/s00401-020-02157-3
van Rumund A, Green AJE, Fairfoul G, Esselink RAJ, Bloem BR, Verbeek MM (2019) alpha-Synuclein real-time quaking-induced conversion in the cerebrospinal fluid of uncertain cases of parkinsonism. Ann Neurol 85:777–781. https://doi.org/10.1002/ana.25447
Wang Z, Becker K, Donadio V, Siedlak S, Yuan J, Rezaee M et al (2020) Skin alpha-Synuclein Aggregation Seeding Activity as a Novel Biomarker for Parkinson Disease. JAMA Neurol, https://doi.org/10.1001/jamaneurol.2020.3311
Acknowledgements
Work at the authors’ research centres was supported by the Swedish Research Council (2016-00906), the Knut and Alice Wallenberg foundation (2017-0383), the Marianne and Marcus Wallenberg foundation (2015.0125), the Strategic Research Area MultiPark (Multidisciplinary Research in Parkinson’s disease) at Lund University, the Swedish Alzheimer Foundation (AF-939932), the Swedish Brain Foundation (FO2021-0293), The Parkinson foundation of Sweden (1280/20), the Konung Gustaf V:s och Drottning Victorias Frimurarestiftelse, the Skåne University Hospital Foundation (2020-O000028), Regionalt Forskningsstöd (2020-0314) and the Swedish federal government under the ALF agreement (2018-Projekt0279). This work was supported in part by the Intramural Research Program of the NIAID, NIH. We are grateful to the Banner Sun Health Research Institute Brain and Body Donation Program of Sun City, Arizona for the provision of human biological materials. The Brain and Body Donation Program has been supported by the National Institute of Neurological Disorders and Stroke (U24 NS072026 National Brain and Tissue Resource for Parkinson’s Disease and Related Disorders), the National Institute on Aging (P30 AG19610 and P30AG072980, Arizona Alzheimer’s Disease Core Center), the Arizona Department of Health Services (contract 211002, Arizona Alzheimer’s Research Center), the Arizona Biomedical Research Commission (contracts 4001, 0011, 05-901 and 1001 to the Arizona Parkinson's Disease Consortium) and the Michael J. Fox Foundation for Parkinson’s Research. The authors thank the study participants and their families. Without their invaluable contribution, this study would not have been possible.
Funding
Open access funding provided by Lund University. The funding sources had no role in the design and conduct of the study; in the collection, analysis, interpretation of the data; or in the preparation, review, or approval of the manuscript.
Author information
Authors and Affiliations
Contributions
SH: Execution of the research project. Design and execution of the statistical analysis. Writing the manuscript draft. CO: Execution of the research project and performing the αSyn RT-QuIC analyses. Co-writing the manuscript. Review and critique of statistical analysis. GES: Execution of the research project. Review and critique of the statistical analysis. Review and critique of the manuscript. DG: Organization of the research project. Review and critique of statistical analysis and manuscript. AGH: Execution of the research project. Review and critique of statistical analysis and manuscript. BRG: Execution of the research project. Data analyses and presentation. CHA: Organization of the research project. Review and critique of statistical analysis and manuscript. TGB: Organization of the research project. Provision of biospecimens. Review and critique of statistical analysis and manuscript. BC: Conception and organization of the research project. Review and critique of the manuscript. OH: Initiation and design of the study. Conception and organization of the research project. Design and review and critique of statistical analysis. Review and critique of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Disclosures
SH has no COIs. OH has acquired research support (for the institution) from AVID Radiopharmaceuticals, Biogen, Eli Lilly, Eisai, Fujirebio, GE Healthcare, Pfizer, and Roche. In the past 2 years, he has received consultancy/speaker fees from Amylyx, Alzpath, Biogen, Cerveau, Fujirebio, Genentech, Roche, and Siemens. BC, CDO, BRG, and AGH have patents pending that relate to various RT-QuIC assays. TGB has received consultancy fees from Vivid Genomics and Acadia Pharmaceuticals and TGB and GES have had research support from AVID Radiopharmaceuticals. CHA has received research support from the NIH, Michael J. Fox Foundation, and Arizona Biomedical Research Commission as well as consulting fees from Amneal, Avion, Cionic, CND Life Science, Eisai, Jazz, Neurocrine, and Precon Health. DG is supported by funding to the Shiley-Marcos ADRC at UC San Diego (NIH/NIA P30-AG062429). DG has served as a consultant for Biogen, Roche, General Electric Healthcare, Fujirebio, Amprion, Generian and Cognition Therapeutics.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplemental Fig. 1.
Comparisons of BioFINDER and AZSAND/BBDP CSFs from PD cases where all replicate reactions were positive.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hall, S., Orrù, C.D., Serrano, G.E. et al. Performance of αSynuclein RT-QuIC in relation to neuropathological staging of Lewy body disease. acta neuropathol commun 10, 90 (2022). https://doi.org/10.1186/s40478-022-01388-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40478-022-01388-7