
Abstract
The diagnosis of Parkinson’s disease (PD) is challenging at all stages due to variable symptomatology, comorbidities, and mimicking conditions. Postmortem assessment remains the gold standard for a definitive diagnosis. While it is well recognized that PD manifests pathologically in the central nervous system with aggregation of α-synuclein as Lewy bodies and neurites, similar Lewy-type synucleinopathy (LTS) is additionally found in the peripheral nervous system that may be useful as an antemortem biomarker. We have previously found that detection of LTS in submandibular gland (SMG) biopsies is sensitive and specific for advanced PD; however, the sensitivity is suboptimal especially for early-stage disease. Further, visual microscopic assessment of biopsies by a neuropathologist to identify LTS is impractical for large-scale adoption. Here, we trained and validated a convolutional neural network (CNN) for detection of LTS on 283 digital whole slide images (WSI) from 95 unique SMG biopsies. A total of 8,450 LTS and 35,066 background objects were annotated following an inter-rater reliability study with Fleiss Kappa = 0.72. We used transfer learning to train a CNN model to classify image patches (151 × 151 pixels at 20× magnification) with and without the presence of LTS objects. The trained CNN model showed the following performance on image patches: sensitivity: 0.99, specificity: 0.99, precision: 0.81, accuracy: 0.99, and F-1 score: 0.89. We further tested the trained network on 1230 naïve WSI from the same cohort of research subjects comprising 42 PD patients and 14 controls. Logistic regression models trained on features engineered from the CNN predictions on the WSI resulted in sensitivity: 0.71, specificity: 0.65, precision: 0.86, accuracy: 0.69, and F-1 score: 0.76 in predicting clinical PD status, and 0.64 accuracy in predicting PD stage, outperforming expert neuropathologist LTS density scoring in terms of sensitivity but not specificity. These findings demonstrate the practical utility of a CNN detector in screening for LTS, which can translate into a computational tool to facilitate the antemortem tissue-based diagnosis of PD in clinical settings.
Similar content being viewed by others


Introduction
Parkinson’s disease (PD), dementia with Lewy bodies, and multiple system atrophy, which are all characterized histologically by intracellular aggregates of misprocessed α-synuclein, are the most common among the spectrum of synucleinopathies, and are the second most common neurodegenerative conditions after Alzheimer disease (AD), with PD being the most common in this group [23]. It is widely accepted that accurate and early diagnosis of PD is needed for meaningful therapeutic approaches for disease modification [30]. Postmortem assessment of brain tissue by an expert neuropathologist remains the only option and gold standard for a definitive diagnosis of PD [39]. The antemortem diagnosis is challenging due to a variable clinical presentation and several mimicking conditions, exemplified most commonly by dementia with Lewy bodies, multiple system atrophy, and progressive supranuclear palsy, obscuring the clinical picture, and delaying treatment [2, 44]. Many clinical trials in PD have failed to identify disease-modifying therapies [8]. Robust and accurate PD biomarkers are crucial to enable early diagnosis, test for target engagement, and serve as surrogate measures of disease in clinical trials.
While PD is diagnosed based on identification of misprocessed α-synuclein in Lewy bodies and Lewy neurites in the central nervous system (CNS), these pathological changes can be also found in peripheral nerves [1, 4, 7, 9, 11, 36, 42, 46]. The reports on occurrence of pathologic α-synuclein in peripheral tissue in PD are often conflicting [3, 4, 7, 15, 21, 22, 28, 32, 40, 42, 43, 50], which could be attributed to a range of methodological factors including specimen acquisition/processing, α-synuclein staining methods, uncertainty of clinical diagnosis, neuropathologist expertise, and blinding [32]. The diagnostic and prognostic value of peripheral biopsy in PD has gained recognition, including in the gastrointestinal tract, salivary glands, olfactory mucosa, and skin [36]. The submandibular gland has particular potential due to the high density of nerves containing pathological α-synuclein as well as its accessibility to biopsy [5, 13, 37, 38, 46]. Lewy-type pathology in the submandibular gland has been detected and characterized in earlier PD stages [3, 15, 21, 50], and its high specificity and good sensitivity has been shown [13, 36]. It has also been observed through systemic peripheral sampling that Lewy-type pathology generally follows a rostro-caudal distribution [3, 43]. The highest densities of Lewy type α-synucleinopathy (LTS) are in the lower esophagus and submandibular gland and lowest in the colon and rectum [3, 10, 43]. More recently, there has been increasing interest in using skin biopsies as a screening and prognostication tool in PD but the density of synuclein pathology-containing nerves is much lower, reducing diagnostic sensitivity [7, 18,19,20,21,22]. Such assessment is subject to inter- and intra-observer variability and represents a laborious and time-consuming process, which limits its practical applications.
Artificial intelligence (AI) in the context of computer vision could be employed to the improve diagnostic utility of peripheral biopsies in PD. AI has been shown to be promising in cancer pathology in screening, detection, and predictive modeling [25]. Its potential in medical imaging of the central nervous system, such as magnetic resonance imaging (MRI) and positron emission tomography (PET), has been explored by many groups [6, 24, 29, 31, 33, 34, 41]. However, the application of AI to histological preparations in neuropathology to date is limited. Our group developed and published the first neurofibrillary tangle classifier applicable to Alzheimer disease (AD), primary age-related tauopathy (PART), and other primary tauopathies [47]. Wurts et al. [53] have presented a report on pathological histomorphological forms of tau in whole slide images (WSI) of AD brain samples. Similarly, Tang et al. [49] have demonstrated that neuritic amyloid plaques and cerebral amyloid angiopathy can be detected with a high degree of precision and recall. This has been validated by Vizcarra et al. [52] in a multicenter study. Together, these studies reinforce the assertion that computer vision and machine learning will have broad applications in the histological assessment of tissues from patients with neurodegenerative diseases.
Here, we applied deep-learning based classification to a collection of WSIs from the Systemic Synuclein Sampling Study (S4), a large multicenter study initiated with the goal of assessing key gaps in knowledge by comparing inter- and intra-individual total α-synuclein in central and peripheral fluid compartments (i.e., cerebrospinal fluid, blood, saliva), and the occurrence of immunohistochemically-defined α-synuclein pathology in three peripheral tissues (i.e., colon, skin, and submandibular gland) at different PD stages compared to controls [1, 11, 13, 14, 51]. Our previous results indicate that peripheral Lewy-type synucleinopathy (LTS) is present in early PD, suggesting its utility as a diagnostic and prognostic biomarker. The expert neuropathologist semi-quantitative assessment of LTS in peripheral biopsies was shown to have nearly perfect specificity in predicting clinical diagnosis and stages of PD; however, the sensitivity was moderate [11, 13]. We applied a trained convolutional neural network (CNN) to minimize barriers to wider application of LTS assessment for early diagnosis of PD. This approach provides robust and reliable quantitative measurements of an array of AI-based features representing LTS burden and distribution on the digitized peripheral biopsy WSI, with potential to be further used as diagnostic, prognostic, and monitoring markers of PD.
Materials and methods
Case materials
The Systemic Synuclein Sampling Study (S4) was a cross-sectional, observational six-site study. Methodology has previously been described, including cohort inclusion/exclusion criteria [13, 51]. Briefly, the study included 60 individuals with idiopathic Parkinson’s disease and 20 controls with specimens of submandibular gland (SMG), skin, colon, CSF, and blood. The PD group consisted of individuals with a clinical diagnosis of PD and abnormal dopamine transporter SPECT imaging, with either early (2 or less years duration, untreated with dopaminergic medication), moderate (2–5 years duration, without motor fluctuations), or advanced (more than 5 years duration with motor fluctuations) disease. Controls consisted of individuals with normal dopamine transporter imaging. Both groups had to be free of dementia and medical conditions that precluded study procedures. All participants underwent Movement Disorders Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) assessment, as previously described (Table 1) [13, 27]. Cerebrospinal fluid (CSF) was obtained via lumbar puncture and total α-synuclein was measured using ELISA as described [14, 51]. Dopamine transporter SPECT scans were obtained and striatal specific binding ratio (SBR) was calculated as mean SBR for right and left putamen and caudate. Biopsies of SMG were obtained and stained as described [1, 11, 14, 51]. Briefly, up to 5 unilateral biopsies per participant were fixed in 10% formalin, embedded in paraffin and cut into 4 μm sections that were then mounted on glass slides [1]. Up to 13 slides from each paraffin block were then treated with a protease and stained with the 5C12 mouse monoclonal antibody. The 42 PD participants and 14 controls whose SMG biopsies yielded adequate tissue were included in the present analysis.
Slide digitization and image management
The stained glass slides were digitalized at 20× magnification using Aperio scanners (Aperio, Leica Biosystems, Kassel, Germany) and the whole slide image (WSI) files were saved in.svs format. A total of 1513 WSIs were used in this study, with 283 used for the development of LTS detector (training and testing of the neural networks) and 1230 for the feature generation and the development of PD status/stage prediction models. The WSI were then converted into a GeoTIFF format. Images were stored on a HIPAA-compliant server behind the hospital firewall for interactive display and annotation over the intranet using the Precise Informatics Platform (PIP), developed by the Center for Computational and Systems Pathology at Mount Sinai (MP, JK, JZ, and GF), which allows for the management of thousands of images with pathologist annotations.
Expert neuropathologist scoring
Digitized images were previously scored by three independent neuropathologists blinded to diagnostic group as described [1, 11, 13]. Briefly, each WSI was classified as positive or negative for α-synuclein pathology and assigned an LTS score ranging from 0 to 3 (Fig. 1), where 0 refers to being negative for α-synuclein, and scores 1–3 refer to scoring density of sparse (1) moderate (2), and frequent (3). A final determination regarding IHC positivity for α-synuclein was made for each slide based on consensus rating of at least 2/3 pathologists; each study subject was assigned derivative score metrics, reflecting cumulative α-synuclein positivity (Additional file 1: Table S2) [11, 13, 14].

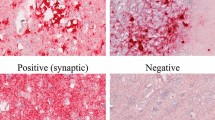
LTS object scoring and confidence ranking. Illustration of scoring density of sparse (A) moderate (B), and frequent (C). Submandibular gland biopsies immunohistochemically stained for α-synuclein with examples of sparse (D) moderate (E) and frequent (F). Examples of confidence ranking examples of definite (G), probable (H), and possible (I). LTS can be visualized and single or multiple immunopositive normal or misshapen axonal profiles in the submandibular gland parenchyma, nerve fascicles, or adjacent to blood vessels. LTS Lewy-type synucleinopathy
Pathological annotations
Ground truth annotations were generated using the Precise Informatics Platform collaborative web-based user interface. We delineated operational morphological definitions of the LTS based our previous studies (Fig. 1A–F) with modifications [1, 11]. Briefly, LTS was operationalized as an IHC α-synuclein-positive object, i.e. “foreground”, with a neurite-like morphology in an appropriate histological context (e.g., periacinar/gland parenchyma, perivascular, or within a nerve bundle). Given high histomorphological variability of LTS and their planes of section, each LTS object was assigned a confidence rank (i.e., definite, probable, and possible) reflecting an annotator’s confidence for further inclusion in weighted computational modeling (Fig. 1D–I). Objects showing IHC α-synuclein-positive linear neurites in an appropriate histological context were scored as “definite”. Single or multiple dot-like objects possibly representing a cross-section of α-synuclein-positive neurites were classified as “possible” reflecting the lower annotator’s confidence. The “probable” rank was used for intermediate confidence. Other α-synuclein immunopositive structures including granules/grains, macrophages, and artifacts were categorized as “background”. This approach increased the number of classifiable objects for training. To assess the annotated ground truth, we conducted annotator training and a concordance study to measure the inter-rater reliability, using a custom interface within the PIP platform, and compared them using a Fleiss’ kappa statistic and percentage agreement.
Neural network training
We used a convolutional neural network (CNN) architecture (InceptionV4 [48]) to train the LTS detector (Fig. 2). The CNN was trained using a system with five NVIDIA Titan Xp GPUs and Intel(R) Xeon(R) CPU E5-2660 v4 @ 2.00 GHz. The convolutional layers in the CNN were initialized with imagenet [16] pre-trained weights. We also modified the first convolutional layer in the InceptionV4 architecture and set the stride equal to 1, which allowed us to use a smaller image size (151 × 151) than the original imagenet model (299 × 299). We used the PyTorch platform for training and creating the prediction masks. When training, various image augmentation methods were applied, including smoothing, sharpening, rotations, flips, jpeg compression, as well as contrast and brightness adjustments. An AdamW optimizer with a learning rate of 0.00001 and weight decay of 0.001 was used for training the final CNN detector [35]. The mini-batch size was 32 per GPU and the network was trained 80 epochs. Definite, probable and possible LTS patches were assigned loss weights equal to 5, 4, and 3, respectively. False positive patches from earlier rounds of training were given a loss weight equal to 2. Artifacts, background and patches with no LTS objects were given a loss weight equal to 1. Higher weights corresponded to larger misclassification penalty. After the training of the CNN detector, we created the prediction masks on the whole slide images by performing the inference on overlapping patches with 40 pixels strides.

Schematic overview of data annotation and deep learning pipeline. LTS are annotated using WSI. The CNN was trained to classify image patches containing LTS from other image patches including tissue, artifacts and background. Different weights were used for the annotated objects while training using the cross entropy loss function for the final network. Image patches are extracted for network training that generates pixel-wise segmentations for LTS and background. Performance is determined using a separate novel set of images (test set) by comparing expert annotation with the trained network. The resulting trained network is further deployed on the naive WSI dataset for assessment of the predictive power of clinical outcomes. LTS Lewy-type synucleinopathy, WSI whole slide image, CNN convolutional neural network
Derivation of image features
To assess the relationship between the detected Lewy-type synucleinopathy objects in the whole slide images and the disease status and progression, we used 60 different image features based on not only the total detected LTS burden, but also their spatial distribution and staining variations to identify patterns similar to what experts consider when producing their assessment score (Additional file 1: Table S3). The PreciseDx features describe the organization of the detected Lewy neurite objects in the whole slide. It includes the local relationship of each object to its neighbors, based on measures of the node degree property in a graph constructed from the objects. These measures provide summary descriptions on the patterns of Lewy neurites in tissue. It also includes descriptions on the separation of the detected objects, measuring the homogeneity of their distributions in tissue. The collection of features can characterize the whole slide in regards to Lewy neurites and we investigate their clinical utility with disease burden. Number of detected LTS patches and the fraction of the detected LTS patches within the overall tissue region represent the LTS load for each slide. To assess the stain variations within the detected LTS patches, we separated the IHC/DAB staining (brown) from the hematoxylin counterstaining (blue) using color deconvolution [45]. After color deconvolution, we computed the sum, mean, median and standard deviation of the hematoxylin and DAB within the detected LTS patches for each slide.
To identify the spatially connected and coherent regions and their distribution patterns, we used affinity propagation to find clusters of the detected LTS patches within the WSI [12, 26]. From the resulting clusters, measures such as simple cluster counts as well as more complex characteristics showing cluster patterns and distributions were computed. The computed features include the mean and standard deviations of cluster size, within cluster dispersion, cluster extent and between cluster scatter [17]. We also computed the clustering indices such as Ball Hall, Banfeld-Raftery, LogSSRatio, Davies-Bouldin, Calinski-Harabasz, and C Index [17]. Moreover, we utilized proprietary graph features, which were constructed by analyzing the spatial relationships between the detected objects (PreciseDx, New York, NY).
Statistical analysis
We trained and validated machine learning-derived image features using logistic regression to predict the disease status and stage and compared to expert assessments. There were 13 WSI per subject available for most cases, however, a few had more than 20 WSI. Each WSI was previously scored by three expert neuropathologists; the derivative scores were generated for each research subject [11, 13]. To generate one single feature vector for each subject, we used the maximum of each feature among all available slides, which performed better than the mean, median, and minimum.
We used a two-step process for selecting predictive features among all 60 engineered features and then trained a predictive model. To avoid overfitting, we split the subjects into train (80%) and test (20%) samples; then, used a logistic regression model with least absolute shrinkage and selection operator (LASSO) regularization to train a prediction model and select the most predictive features from the model. Since the number of subjects was limited (42 patients and 14 controls), the selected features would highly depend on the subjects in the training set. Hence, we repeated the random train/test split 1000 times and recorded the selected features and their importance weights for each split. The most frequently selected features with the largest importance weights were used to train and validate prediction models. We trained and validated 1000 Logistic Regression models using random train and test splits. We used an Elastic-Net penalty with l1_ratio = 0.01 (the Elastic-Net mixing parameter). Additional statistical analyses were performed using IBM SPSS Statistics version 26 and subscription for windows (IBM Corp., Armonk, NY, USA), which included Pearson and Spearman’s correlation analyses between AI features, expert scoring, and clinical characteristics; also Wilcoxon-Mann–Whitney rank-sum and Kruskal–Wallis analyses.
Results
Ground truth generation
First, to ensure reproducibility in our ground truth dataset used for training the neural network, we asked whether Lewy-type synucleinopathy (LTS) objects could be annotated in a consistent fashion and a minimal inter-observer variability bias. We performed a concordance study among five neuropathologists, using independent blinded assessments on 600 patches containing a range of LTS objects derived from a subset of the whole slide images (WSIs) of immunohistochemically stained submandibular gland biopsies from the Systemic Synuclein Sampling Study (S4) [1]. This balanced dataset was derived from prescreening and AI-detected false-positives from pilot studies (data not shown). Overall, we found a high degree of agreement between raters (5-way Fleiss’ kappa of 0.70, range 0.60–0.89 between pairs of raters; Additional file 1: Table S1). When ambiguous objects (“possible” LTS) were excluded, there was improvement in concordance of calls (Fleiss’ kappa of 0.73, range 0.84–0.90). This analysis prompted us to introduce a weighted ranking system allowing us delineate more concise operational definitions that included possible (1), probable (2), and definite (3) LTS ranked categories. These definitions were then deployed to generate the ground truth training dataset of annotated LTS objects from the training 283 WSI group from 56 research subjects, in which each LTS object was additionally ranked. WSI were then randomly divided into 80% for training and validation (i.e., model selection), with 20% reserved as a test set for performance evaluation (Additional file 1: Table S4). In total, we annotated 8450 positive foreground LTS objects and assigned each a confidence rank alongside a total of 35,066 background objects (Additional file 1: Table S5), which straightened the specificity of the detection.
Convolutional neural network (CNN) training and validation
For CNN training and validation, we conducted three rounds of annotation/training iterative cycles, triaging out false positives and triaging in false negatives, thus improving the ground truth and the accuracy of detection. The LTS detection time for a single WSI ranged from 10 to 40 min (averaging 18 min) with performance depending on the area of the tissue within the WSI. Examples of an annotated WSI with CNN inference, the 40 × 40-pixel overlapping inference patch indication, and examples of overlapping and true/false positive CNN detection inferences are shown (Fig. 3).

Examples of CNN deployment on SMG biopsy WSI. A An example of annotated objects (blue) and CNN inference (grey shading). A 40 × 40 pixel inference patch is shown. B An example of true positive CNN classification. C An example of false positive CNN classification. CNN, convolutional neural network; SMG, submandibular gland; LTS, Lewy-type synucleinopathy, WSI, whole slide image
Weighted CNN shows improved performance metrics
Each LTS object was assigned a confidence rank for weighted modeling to allow tunable penalties to improve network performance. This permitted us to train and compare weighted and unweighted CNNs (Table 2). We found that while both had excellent sensitivity/recall (0.99), the specificity was lower in the non-weighted version (0.92) compared to the weighted version (0.99). When the non-weighted and weighted network precision was compared there was a marked increase (0.41 vs. 0.81 respectively), which was also seen in F1 scores (0.59 vs. 0.89). Accuracy and area under the curve (AUC) receiver operating characteristics (ROC) were also higher in the weighted network. Thus, given the superior performance of the weighted CNN, it was used for further studies.
Comparison of the CNN with expert scores
We next compared annotation ground truth and the CNN LTS object detection with the expert scoring performed in our previous study [13]. Ground truth annotation follows the same trend and expert scoring with good distinction between scored groups (Fig. 4A). These expert scores represent the subjective assessment from the neuropathologist evaluators, integrating rater confidence of object identity alongside other features such as cellular context. In the set of WSI used for network training that were scored as negative, on average 1.6 LTS objects were identified and included in our annotations, and 17 CNN detected LTS-positive patches (Fig. 4B, Additional file 1: Table S6). Overall, we found a highly significant correlation between expert scores and annotated ground truth as well as the CNN LTS detection (4.3 × 10−69, Rho = 0.82 and 9.9 × 10−12, 0.76 respectively). There was a highly significant difference in ground truth annotated objects count and CNN-detected LTS-positive patches count between expert scored groups (p = 4.7 × 10−7, Kruskal–Wallis). The strong correlation between our ground truth object annotations and the expert LTS burden scores gave us further confidence in the quality of our ground truth. The strong correlation between both these measures and the CNN scores gave us further confidence in our network (Fig. 5).

Comparison of ground truth annotations and CNN detection with expert scoring. A Expert annotation distribution boxplot in test WSI cohort (n = 56), Mann–Whitney two-tailed U test between score groups p values; Kruskal–Wallis H test of annotated LTS between expert score groups, and Spearman correlation between LTS burden and expert scores. B CNN, 40 × 40 patches positive for LTS distribution boxplot in test WSI cohort (n = 56), Mann–Whitney two-tailed U test between score groups p values; Kruskal–Wallis H test of 40 × 40 patches between expert score groups, and Spearman correlation between 40 × 40 patches positive for LTS burden and a score in test cohort. Scoring was performed as follows: each WSI was classified as positive or negative for α-synuclein pathology and assigned an LTS score ranging from 0 to 3 (Fig. 1), where 0 refers to being negative for α-synuclein, and scores 1–3 refer to scoring density of sparse (1) moderate (2), and frequent (3). CNN convolutional neural network, SMG submandibular gland, LTS Lewy-type synucleinopathy

Examples of CNN deployment on SMG biopsy WSI. A An Example of a WSI. B, C LTS patch detection and features generation (e.g., patches clustering, in color). CNN convolutional neural network, SMG submandibular gland, LTS Lewy-type synucleinopathy
CNN-derived features improve prediction of clinical PD status
In order to comprehensively evaluate the LTS CNN, it was necessary to test it on a set of naïve images. We used WSI (n = 1230) of additional sections from the SMG tissue blocks also stained using α-synuclein immunohistochemistry derived from the cohort of PD patients (n = 42) and controls (n = 14). We used our CNN-derived LTS-positive patches to generate a set of features that could be used for correlation analyses with clinical outcomes and neuropathological assessments, and improve the predictive power of our model. We selected 13 high-ranking features for PD status prediction out of the initial set of 60 AI features using a logistic regression model and a least absolute shrinkage and selection operator (LASSO) shrinkage method for pruning. The expert slide level score specificity prediction of disease status is the same as reported previously [13] and higher than AI specificity in our series (Table 3). The logistic regression analysis showed that the prediction of PD status was slightly more accurate with AI features compared to the expert scoring and its derivatives. The mean and standard deviation of AI features performance metrics in predicting the PD status are compared to those of the models based on the expert assessment scores and derivative features (Table 3).
AI-derived object features improve accuracy of PD stage prediction
In order to improve PD staging prediction modeling, we selected 5 high-ranking features for PD stage out of the initial set of 60 AI features using the same logistic regression model and a LASSO shrinkage method for pruning (Additional file 1: Table S3). The accuracy of prediction of PD stage also increased with the use of AI compared to the models using expert scoring. This improvement was more prominent while assessing the difference between PD stages only (0.64 v. 0.59), whereas the difference in accuracy is lower (0.48 v. 0.45) when controls were taken into the analysis. Accuracy is based on both sensitivity and specificity, however, while AI had higher sensitivity, expert scoring has higher specificity, when distinction of PD from controls is the criterion (Table 4). To determine how well the selected 15 AI features, which are predictive of PD status and stage, correlate with expert scoring we applied Spearman’s correlation analysis. It showed that 14 out 15 selected AI features were in significant (p < 0.001) correlation with expert scoring on individual slides and 13 out of 15 were in significant (p < 0.001) correlation a summarized synuclein score per patient (Table 5).
AI-derived object features distinguish between PD status and PD stages
To confirm that the 13 high-ranking AI features, derived with mathematical modeling, are capable of reliably distinguishing between PD and controls, we applied Wilcoxon–Mann–Whitney analysis, in which 8 of 13 selected features have shown statistically significant differences between PD patients and controls in selected ranked measures. Of note, all the most significant AI features correlates are reflecting the LTS clustering characteristics. Other features, unrelated to LTS objects clustering, that show the difference between PD and controls, are reflecting the LTS burden: the standard deviation of the DAB channel and the standard deviation of the hematoxylin channel (Table 6). We also applied the Kruskal–Wallis analysis to verify that those selected features are capable of reliably distinguishing among PD stages (early [1], moderate [2], and advanced [3]), in which 4 of 5 selected features, all reflecting the LTS clustering characteristics, have shown statistically significant differences among the PD stages (Table 6).
AI-derived features correlation with UPDRS, CSF α-synuclein, and neuroimaging markers
We also explored the relationship between the set of 15 selected AI features and clinical and biomarker measures of PD disease severity namely MDS-UPDRS total and part III scores (where higher values indicate more severe disease), CSF total α-synuclein, and dopamine transporter binding in striatum measured with SPECT (DAT-SBR; where lower values indicate lower (worse) DAT binding). Pearson correlation showed statistically significant, although moderate, inverse relationships between some AI features and median bilateral striatal DAT-SBR in PD patients. Lower correlations were observed between AI features and MDS-UPDRS scores and CSF α-synuclein biochemical values (Table 7).
Discussion
It is well established that while Parkinson’s disease pathologically manifests in the CNS with aggregation of α-synuclein as Lewy bodies and Lewy neurites, this pathology can also be found in the peripheral nervous system. Peripheral Lewy-type synucleinopathy objects (LTS) are present in PD, suggesting its utility as a diagnostic and prognostic biomarker [11]. Previous studies have shown that the expert neuropathologist semi-quantitative scoring of immunohistochemically stained WSI from PD patients, based on LTS density in the submandibular gland has high specificity in diagnosing PD, but suboptimal sensitivity. In this study, we present a novel machine learning-based method using a total LTS burden as well as clustering characteristics reflecting LTS density and distribution on digitized IHC-stained preparations. Our study demonstrates that deep machine learning represents a feasible way to augment routine histological examination, and trained neural networks could be deployed in detecting the peripheral LTS and improving accuracy for further confirmatory assessment by a neuropathologist.
A critical step for training a neural network is to minimize the inter-observer variation to develop the most robust ground truth. We designed an inter-rater reliability study and conducted consensus conferences among raters to improve the operational definitions for ground truth objects. We have achieved a high degree of agreement among raters and went through iterative rounds of discussions about ambiguous and challenging objects. We trained a CNN to identify image patches that contain LTS objects. We also conducted three rounds of annotation/training iterative cycles triaging out false positive and triaging in a false negative, which resulted in the high-quality ground truth and further translated into high accuracy of LTS detection (Table 2). Since there were many LTS objects on each slide, especially those with higher burden, comprehensive annotation of all individual LTS objects was not practical. Also, there were many small objects densely packed with larger objects that made it very difficult to localize and annotate them. Hence, rather than using object localization methods such as region-based CNN (RCNN) or single shot multibox detector (SSD), we opted to use CNN to determine whether an image patch contains any (one or multiple) LTS object. Using the confidence score of the annotated objects as error weights in the loss function (when training the CNN classifier) also helped us to increase the sensitivity of the detector in identifying definite and probable LTS objects.
We showed that AI-based LTS detection and distribution characteristics correlate well with expert scoring performed in the previous study, but AI may offer greater speed and higher sensitivity. It currently takes our LTS classifier an average of 18 min to computationally screen an entire WSI and highlight the ROI with a high probability of LTS. Fully automatic detection of LTS at this performance level will enable large-scale screening of WSI for further confirmation by a human expert neuropathologist. This illustrates the feasibility of applying this approach to large datasets and paves the road to further adopting this approach in clinical practice. We also demonstrated that AI has higher accuracy, sensitivity, and F1 score in predicting PD status than human expert scoring; as well as higher overall accuracy in predicting PD progression. Even though the specificity of an AI in predicting PD status was lower than expert neuropathologist scoring, the current version of trained AI shows to be promising in the ability to reproducibly identify high probability LTS foci on a digital slide.
We showed that LTS cluster size characteristics as well as the graph features reflecting the spatial relationships between the detected objects were the highest-ranking features that correlated the best with the expert score per slide and per patient (Table 5). The highest-ranking features to differentiate the controls and PD and to detect the difference among the PD stages are all clustering characteristics, whether they are well-known (e.g., Calinski-Harabasz index or LTS cluster size standard deviation) or the proprietary graph features newly developed by PreciseDx (Table 6). AI features, determined using mathematical modeling, can be potentially useful to clinical-pathological-radiological correlations, exemplified with the statistically significant, although moderate, inverse relationships between selected AI features and median bilateral striatal DAT-SBR in PD patients (Table 7).
In our study, we showed that with our initial training of the CNN detector, it can achieve a similar outcome compared to the expert performance. However, the AI approach is shown to be more reliable, consistent, and cost-efficient compared to the old-fashioned way. The expert could be subjected to inter and intra-observer variation while AI is consistent and able to offer the most accurate result possible. To train a neuropathologist requires a considerable investment of both money and time. In addition to the extensive training, it could still take an expert a substantial time to fully annotate an entire WSI. While AI can annotate an entire WSI in mere minutes, and with a larger sample set AI can continue perfecting itself.
Expert scoring and AI-based LTS burden and clustering characteristics correlate well, but AI may have some advantages. On the currently limited dataset, AI has shown to have (1) high correlation with expert scoring; (2) higher accuracy, sensitivity, and F1 score in predicting PD status than expert scoring; (3) higher accuracy in predicting PD progression than expert scoring, albeit with less specificity. Overall, we found that LTS clustering characteristics are a better predictor of the outcome than crude LTS burden. Our trained weighted InceptionV4 neural network is promising in its ability to reproducibly identify high probability LTS foci on a digital slide. Together with the subsequent mathematical modeling algorithms reflecting LTS clustering characteristics offer a useful tool in assessment and screening of histological slides for total α-synuclein burden and for prediction of PD status and stage of progression and for further utilization in practical clinical applications.
This study had several notable limitations. Of note, we had a relatively small dataset. In the future, larger datasets may allow us to develop more sensitive and specific tests. Another limitation is that we focused our effort on SMG biopsies stained with the 5C12 anti-α-synuclein antisera by immunohistochemistry. It is unclear if this approach would be valid in other tissues or other antisera, which is a critical question as interest in skin biopsies for the diagnosis of PD is growing and expanding our analysis to skin and colon biopsies would be of value. Also, it is unclear whether other α-synuclein antibodies would give similar results. Potentially, we further plan to expand the subject cohort for better neural network training. Because of the nature of the study, there was no autopsy material available for definitive neuropathological diagnosis and clinical-pathological correlations. Expanding the project to include autopsy subjects will allow us to perform AI-clinical-pathological correlations.
In conclusion, we demonstrated the promise of AI in aiding an expert in making an antemortem diagnosis of definite PD, and potentially other synucleinopathies, such as dementia with Lewy bodies and multiple system atrophy. We will continue broaden and improve our research protocol and approach to the application of AI in neuropathology. The application of AI in clinical pathology is limitless, the quantitative data uncovered by AI networks will not only augment the currently used qualitative and semi-quantitative approach in the assessment of the pathognomonic features, but also be used for correlative and association analyses with clinical, radiological, genetic, and biochemical data.
Availability of data and materials
De-identified clinical data collected for this study will be available at https://braincommons.org. Data requestors will need to sign a data use agreement via the BRAIN Commons website (https://braincommons.org) to gain access. Additional computational data will be accessible on obtaining permission on GitHub: https://github.com/PreciseDx/S4-MJFF.
Abbreviations
- AI:
-
Artificial intelligence
- CSF:
-
Cerebrospinal fluid
- DAT:
-
Dopamine transporter
- DAB:
-
Diaminobenzidine
- IHC:
-
Immunohistochemistry
- LTS:
-
Lewy-type synucleinopathy
- MDS-UPDRS:
-
Movement Disorders Society Unified Parkinson Disease Rating Scale
- MDS-UPDRS-III:
-
Movement Disorders Society Unified Parkinson’s Disease Rating Scale part III
- PD:
-
Parkinson disease
- S4:
-
Systemic Synuclein Sampling Study
- SBR:
-
Dopamine transporter mean striatum specific binding ratio
- SPECT:
-
Single-photon emission computer tomography
- SMG:
-
Submandibular gland
References
(2016) Systemic synuclein sampling study s4: biospecimen collection, processing, and shipment manual. https://michaeljfox.Org/Files/S4_Biologics_Manual_Version_2.Pdf
Adler CH, Beach TG, Hentz JG, Shill HA, Caviness JN, Driver-Dunckley E, Sabbagh MN, Sue LI, Jacobson SA, Belden CM et al (2014) Low clinical diagnostic accuracy of early vs advanced Parkinson disease: clinicopathologic study. Neurology 83:406–412. https://doi.org/10.1212/Wnl.0000000000000641
Adler CH, Dugger BN, Hentz JG, Hinni ML, Lott DG, Driver-Dunckley E, Mehta S, Serrano G, Sue LI, Duffy A (2016) Peripheral synucleinopathy in early Parkinson’s disease: submandibular gland needle biopsy findings. Mov Disord 31:250–256
Adler CH, Dugger BN, Hinni ML, Lott DG, Driver-Dunckley E, Hidalgo J, Henry-Watson J, Serrano G, Sue LI, Nagel T et al (2014) Submandibular gland needle biopsy for the diagnosis of Parkinson disease. Neurology 82:858–864. https://doi.org/10.1212/Wnl.0000000000000204
Adler CH, Serrano GE, Zhang N, Hinni ML, Lott DG, Mehta SH, Sue LI, Intorcia A, Beach TG (2019) Feasibility of repeat and bilateral submandibular gland needle biopsies in Parkinson’s disease. Parkinsonism Relat Disord 68:69–72. https://doi.org/10.1016/J.Parkreldis.2019.10.006
Akkus Z, Galimzianova A, Hoogi A, Rubin DL, Erickson BJ (2017) Deep learning for brain MRI segmentation: state of the art and future directions. J Digit Imaging 30:449–459. https://doi.org/10.1007/S10278-017-9983-4
Antelmi E, Donadio V, Incensi A, Plazzi G, Liguori R (2017) Skin nerve phosphorylated alpha-synuclein deposits in idiopathic rem sleep behavior disorder. Neurology 88:2128–2131. https://doi.org/10.1212/Wnl.0000000000003989
Athauda D, Foltynie T (2015) The ongoing pursuit of neuroprotective therapies in Parkinson disease. Nat Rev Neurol 11:25–40. https://doi.org/10.1038/Nrneurol.2014.226
Beach TG, Adler CH, Serrano G, Sue LI, Walker DG, Dugger BN, Shill HA, Driver-Dunckley E, Caviness JN, Intorcia A et al (2016) Prevalence of submandibular gland synucleinopathy in Parkinson’s disease, dementia with Lewy bodies and other Lewy body disorders. J Parkinsons Dis 6:153–163. https://doi.org/10.3233/Jpd-150680
Beach TG, Adler CH, Sue LI, Vedders L, Lue L, White CL III, Akiyama H, Caviness JN, Shill HA, Sabbagh MN et al (2010) Multi-organ distribution of phosphorylated alpha-synuclein histopathology in subjects with Lewy body disorders. Acta Neuropathol 119:689–702. https://doi.org/10.1007/S00401-010-0664-3
Beach TG, Serrano GE, Kremer T, Canamero M, Dziadek S, Sade H, Derkinderen P, Corbille AG, Letournel F, Munoz DG et al (2018) Immunohistochemical method and histopathology judging for the systemic synuclein sampling study (S4). J Neuropathol Exp Neurol 77:793–802. https://doi.org/10.1093/Jnen/NLY056
Bodenhofer U, Kothmeier A, Hochreiter S (2011) Apcluster: an R package for affinity propagation clustering. Bioinformatics 27:2463–2464. https://doi.org/10.1093/Bioinformatics/Btr406
Chahine LM, Beach TG, Brumm MC, Adler CH, Coffey CS, Mosovsky S, Caspell-Garcia C, Serrano GE, Munoz DG, White CL et al (2020) In vivo distribution of alpha-synuclein in multiple tissues and biofluids in parkinson disease. Neurology 95:E1267–E1284. https://doi.org/10.1212/Wnl.0000000000010404
Chahine LM, Beach TG, Seedorff N, Caspell-Garcia C, Coffey CS, Brumm M, Adler CH, Serrano GE, Linder C et al (2018) Feasibility and safety of multicenter tissue and biofluid sampling for alpha-synuclein in Parkinson’s disease: the systemic synuclein sampling study (S4). J Parkinsons Dis 8:517–527. https://doi.org/10.3233/Jpd-181434
Del Tredici K, Hawkes CH, Ghebremedhin E, Braak H (2010) Lewy pathology in the submandibular gland of individuals with incidental Lewy body disease and sporadic Parkinson’s disease. Acta Neuropathol 119:703–713. https://doi.org/10.1007/S00401-010-0665-2
Deng J, Dong W, Socher R, Li L-J, Li K, Fei-Fei L (2009) Imagenet: a large-scale hierarchical image database. In: 2009 IEEE Conference on Computer Vision and Pattern Recognition. IEEE, City, pp 248–255
Desgraupes B (2013) Clustering indices. Univ Paris Ouest-Lab Modal’x 1:34
Donadio V, Doppler K, Incensi A, Kuzkina A, Janzen A, Mayer G, Volkmann J, Rizzo G, Antelmi E, Plazzi G et al (2019) Abnormal alpha-synuclein deposits in skin nerves: intra- and inter-laboratory reproducibility. Eur J Neurol 26:1245–1251. https://doi.org/10.1111/Ene.13939
Donadio V, Incensi A, Leta V, Giannoccaro MP, Scaglione C, Martinelli P, Capellari S, Avoni P, Baruzzi A, Liguori R (2014) Skin nerve alpha-synuclein deposits: a biomarker for idiopathic Parkinson disease. Neurology 82:1362–1369. https://doi.org/10.1212/Wnl.0000000000000316
Donadio V, Incensi A, Piccinini C, Cortelli P, Mp G, Baruzzi A, Liguori R (2016) Skin nerve misfolded alpha-synuclein in pure autonomic failure and Parkinson disease. Ann Neurol 79:306–316. https://doi.org/10.1002/Ana.24567
Doppler K, Jentschke H-M, Schulmeyer L, Vadasz D, Janzen A, Luster M, Höffken H, Mayer G, Brumberg J, Booij J (2017) Dermal phospho-alpha-synuclein deposits confirm rem sleep behaviour disorder as prodromal Parkinson’s disease. Acta Neuropathol 133:535–545
Doppler K, Volkmann J, Sommer C (2016) Skin biopsies in the differential diagnosis of Parkinsonism: are we ready for simplified protocols? Brain 139:E5–E5
Dorsey E, Constantinescu R, Thompson J, Biglan K, Holloway R, Kieburtz K, Marshall F, Ravina B, Schifitto G, Siderowf A (2007) Projected number of people with Parkinson disease in the most populous nations, 2005 through 2030. Neurology 68:384–386
El-Dahshan E-SA, Mohsen HM, Revett K, Salem A-BM (2014) Computer-aided diagnosis of human brain tumor through MRI: a survey and a new algorithm. Expert Syst Appl 41:5526–5545
Fernandez G, Madduri AS, Marami B, Prastawa M, Scott R, Zeineh J, Donovan M (2021) Artificial intelligence methods for predictive image-based grading of human cancers. Artif Intell Deep Learn Pathol, pp 175–210
Frey BJ, Dueck D (2005) Mixture modeling by affinity propagation. Adv Neural Inf Process Syst 18:379–386
Goetz CG, Tilley BC, Shaftman SR, Stebbins GT, Fahn S, Martinez-Martin P, Poewe W, Sampaio C, Stern MB, Dodel R et al (2008) Movement disorder society-sponsored revision of the unified Parkinson’s disease rating scale (Mds-Updrs): scale presentation and clinimetric testing results. Mov Disord 23:2129–2170. https://doi.org/10.1002/Mds.22340
Goldman JG, Andrews H, Amara A, Naito A, Alcalay RN, Shaw LM, Taylor P, Xie T, Tuite P, Henchcliffe C (2018) Cerebrospinal fluid, plasma, and saliva in the biofind study: relationships among biomarkers and Parkinson’s disease features. Mov Disord 33:282–288
Hinton G (2018) Deep learning-a technology with the potential to transform health care. JAMA 320:1101–1102. https://doi.org/10.1001/Jama.2018.11100
Lang AE, Espay AJ (2018) Disease modification in Parkinson’s disease: current approaches, challenges, and future considerations. Mov Disord 33:660–677. https://doi.org/10.1002/Mds.27360
Lecun Y, Bengio Y, Hinton G (2015) Deep learning. Nature 521:436–444. https://doi.org/10.1038/Nature14539
Lee JM, Derkinderen P, Kordower JH, Freeman R, Munoz DG, Kremer T, Zago W, Hutten SJ, Adler CH, Serrano GE et al (2017) The search for a peripheral biopsy indicator of alpha-synuclein pathology for Parkinson disease. J Neuropathol Exp Neurol 76:2–15. https://doi.org/10.1093/Jnen/Nlw103
Litjens G, Kooi T, Bejnordi BE, Setio AAA, Ciompi F, Ghafoorian M, Van Der Laak J, Van Ginneken B, Sanchez CI (2017) A survey on deep learning in medical image analysis. Med Image Anal 42:60–88. https://doi.org/10.1016/J.Media.2017.07.005
Liu F, Jang H, Kijowski R, Bradshaw T, Mcmillan AB (2018) Deep learning MR imaging-based attenuation correction for PET/MR imaging. Radiology 286:676–684. https://doi.org/10.1148/Radiol.2017170700
Loshchilov I, Hutter F (2017) Decoupled weight decay regularization. arXiv:1711.05101
Ma LY, Liu GL, Wang DX, Zhang MM, Kou WY, Feng T (2019) Alpha-synuclein in peripheral tissues in Parkinson’s disease. Acs Chem Neurosci 10:812–823. https://doi.org/10.1021/Acschemneuro.8b00383
Manne S, Kondru N, Jin H, Anantharam V, Huang X, Kanthasamy A, Kanthasamy A (2020) Alpha-synuclein real-time quaking-induced conversion in the submandibular glands of Parkinson’s disease patients. Mov Disord 35:268–278. https://doi.org/10.1002/Mds.27907
Mazzetti S, Basellini MJ, Ferri V, Cassani E, Cereda E, Paolini M, Calogero AM, Bolliri C, De Leonardis M, Sacilotto G et al (2020) Alpha-synuclein oligomers in skin biopsy of idiopathic and monozygotic twin patients with Parkinson’s disease. Brain 143:920–931. https://doi.org/10.1093/Brain/Awaa008
Mckeith IG, Boeve BF, Dickson DW, Halliday G, Taylor JP, Weintraub D, Aarsland D, Galvin J, Attems J, Ballard CG et al (2017) Diagnosis and management of dementia with Lewy bodies: fourth consensus report of the DLB consortium. Neurology 89:88–100. https://doi.org/10.1212/Wnl.0000000000004058
Mollenhauer B, Bowman FD, Drake D, Duong J, Blennow K, El-Agnaf O, Shaw LM, Masucci J, Taylor P, Umek RM et al (2019) Antibody-based methods for the measurement of alpha-synuclein concentration in human cerebrospinal fluid—method comparison and round robin study. J Neurochem 149:126–138. https://doi.org/10.1111/Jnc.14569
Naylor Cd (2018) On the prospects for a (deep) learning health care system. JAMA 320:1099–1100. https://doi.org/10.1001/Jama.2018.11103
Pouclet H, Lebouvier T, Coron E, Des Varannes S, Neunlist M, Derkinderen P (2012) A comparison between colonic submucosa and mucosa to detect Lewy pathology in Parkinson’s disease. Neurogastroenterol Motil 24:E202–E205
Pouclet H, Lebouvier T, Coron E, Des Varannes SB, Rouaud T, Roy M, Neunlist M, Derkinderen P (2012) A comparison between rectal and colonic biopsies to detect Lewy pathology in Parkinson’s disease. Neurobiol Dis 45:305–309
Rizzo G, Copetti M, Arcuti S, Martino D, Fontana A, Logroscino G (2016) Accuracy of clinical diagnosis of Parkinson disease: a systematic review and meta-analysis. Neurology 86:566–576. https://doi.org/10.1212/Wnl.0000000000002350
Ruifrok AC, Johnston DA (2001) Quantification of histochemical staining by color deconvolution. Anal Quant Cytol Histol 23:291–299
Shin J, Park S-H, Shin C, Kim J-H, Yun TJ, Kim H-J, Jeon B (2019) Submandibular gland is a suitable site for alpha synuclein pathology in Parkinson disease. Parkinsonism Relat Disord 58:35–39
Signaevsky M, Prastawa M, Farrell K, Tabish N, Baldwin E, Han N, Iida MA, Koll J, Bryce C, Purohit D et al (2019) Artificial intelligence in neuropathology: deep learning-based assessment of tauopathy. Lab Invest 99:1019–1029. https://doi.org/10.1038/S41374-019-0202-4
Szegedy C, Ioffe S, Vanhoucke V, Alemi A (2016) Inception-V4, inception-resnet and the impact of residual connections on learning. arXiv:1602.07261
Tang Z, Chuang KV, Decarli C, Jin LW, Beckett L, Keiser MJ, Dugger BN (2019) Interpretable classification of Alzheimer’s disease pathologies with a convolutional neural network pipeline. Nat Commun 10:2173. https://doi.org/10.1038/S41467-019-10212-1
Vilas D, Iranzo A, Tolosa E, Aldecoa I, Berenguer J, Vilaseca I, Marti C, Serradell M, Lomena F, Alos L et al (2016) Assessment of alpha-synuclein in submandibular glands of patients with idiopathic rapid-eye-movement sleep behaviour disorder: a case-control study. Lancet Neurol 15:708–718. https://doi.org/10.1016/S1474-4422(16)00080-6
Visanji NP, Mollenhauer B, Beach TG, Adler CH, Coffey CS, Kopil CM, Dave KD, Foroud T, Chahine L, Jennings D et al (2017) The systemic synuclein sampling study: toward a biomarker for Parkinson’s disease. Biomark Med 11:359–368. https://doi.org/10.2217/Bmm-2016-0366
Vizcarra JC, Gearing M, Keiser MJ, Glass JD, Dugger BN, Gutman DA (2020) Validation of machine learning models to detect amyloid pathologies across institutions. Acta Neuropathol Commun 8:59. https://doi.org/10.1186/S40478-020-00927-4
Wurts A, Oakley DH, Hyman BT, Samsi S (2020) Segmentation of tau stained Alzheimers brain tissue using convolutional neural networks. In: 2020 42nd annual international conference of the IEEE engineering in medicine & biology society (Embc). IEEE, City, pp 1420–1423
Acknowledgements
This work was supported by the Michael J. Fox Foundation for Parkinson’s Research, National Institutes of Health [R01 AG054008, R01 NS095252, R01 NS086736 and, R01 AG062348 to JFC], the Rainwater Charitable Trust (Tau Consortium), and the Javed and Shahnaz Iqbal Family Trust.
Author information
Authors and Affiliations
Contributions
All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All images were de-identified in accordance with the policies and regulation at the Icahn School of Medicine at Mount Sinai and its institutional review board.
Competing interests
Bahram Marami, Marcel Prastawa, Mary Sawyer, Israel Duran, John Koll, Gerardo Fernandez, Jack Zeineh, and Carlos Cordon-Cardo disclose their relationship with PreciseDx™, an artificial intelligence-guided pathology diagnostics company, which has developed proprietary platform and AI algorithms used in this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplementary tables.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Signaevsky, M., Marami, B., Prastawa, M. et al. Antemortem detection of Parkinson’s disease pathology in peripheral biopsies using artificial intelligence. acta neuropathol commun 10, 21 (2022). https://doi.org/10.1186/s40478-022-01318-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40478-022-01318-7