
Abstract
Purpose
Menopause occurring before the age of 40 is premature and between 40 and 44 years age is early, since the natural age of menopause lies between 45 and 50. The endocrine changes that come with menopause include an erratic decline in estrogen levels which affects the brain. Thus, leading to changes in cognitive function in the longer term due to the menopausal transition. The study aims to explore the effect of premature and early menopause on cognitive health, and psychosocial well-being. The moderated multiple mediation hypothesis of the study is that the effect of premature or early menopause is mediated by depression and insomnia, while all the pathways are moderated by smoking habits.
Data and Methods
The study utilized Longitudinal Aging Study in India (LASI), 2017–2018, Wave 1 data. The sample of 31,435 women were aged 45 and above and did not undergo hysterectomy. A moderated multiple mediation model was used to understand the association between premature or early menopause (X), insomnia (M1), depression (M2), moderator (W), and cognitive health (Y), while controlling for possible confounders.
Results
Premature menopause was negatively associated with cognition (β:-0.33; SE:0.12; p < 0.05), whereas positively associated with insomnia (β:0.18; SE:0.03; p < 0.001) and depression (β:0.25; SE:0.04; p < 0.001). There is a moderating effect of smoking or tobacco consumption has a significant moderating effect on the pathways among premature menopause, depression, insomnia and cognition. When the same model was carried out for early menopause (40–44 years), the results were not significant.
Conclusions
The findings emphasize the fact that smoking is associated with premature menopause, depression and insomnia. Women who experienced premature menopause has lower cognitive scores, depressive symptoms and insomnia symptoms, which were higher among those who consumed tobacco. The study, strongly recommends the dissemination of information on the negative effects of tobacco consumption and making more informed choices to maintain a healthy life. More research into various methods and therapy is needed to determine the relationship between the age of early menopause and their psychosocial well-being.
Similar content being viewed by others

Introduction
Menopause is an important event that marks the end of a woman’s reproductive period. The majority of women normally attain menopause in the age bracket of 45 and 55 [1]. Some women, due to ovarian insufficiency attains menopause at an early age due to lifestyle factors and hormonal imbalances. Menopause occurring before the age of 40 is premature and between 40 and 44 years age is early, since the natural age of menopause lies between 45 and 50. The cessation of menses is marked by amenorrhea, a rise in gonadotropin levels and oestrogen deficiency [2].
The endocrine changes that come with menopause include an erratic decline in estrogen levels which affects the brain [3]. Thus, leading to changes in cognitive function in the longer term due to the menopausal transition [4].
Effect of premature failure of ovarian function on cognitive abilities
Evidence of changes in estrogen levels accounting for speculated increased memory complaints during the menopausal transition exists [5, 6]. There are experimental studies that have suggested that estrogen has neurological effects post menopause, the brain atrophy of women accelerates at a faster rate than in men [7, 8]. Given that this fact is still debatable [9, 10], there have been reported positive correlations between endogenous estrogen levels and cognitive function [11, 12]. Also, there have been empirical studies that reported that women who experience premature ovarian failure, be it surgical or natural, have poor verbal fluency and memory in later life. It is associated with an increased risk of psychomotor speed decline [1, 13].
Mediating role of depression between premature failure of ovarian function and cognition
An emerging public health challenge in the global scenario is depression, which affects people of all ages and is one of the leading causes of morbidity. Stress, adverse life events, biological, psychological, and social factors are all associated with depression [14]. Cognitive impairments interfere with one’s ability to think or focus, including indecisiveness, and memory loss all of which are criterion items for a diagnosis of depression [15]. Postmenopausal hormonal imbalances lead to neurological impacts and evidences show that depression is increased in later life, is menopause is attained prematurely [4, 16].
In addition to the psychological impacts, depression typically affects a person’s life, social relationships, psychomotor abilities, and leads to fatigue and even insomnia [17]. Studies have found that patients suffering from depression had problems distinguishing between similar or identical objects and suffered short-term memory loss [18,19,20]. Depression is one of the evident symptoms of menopause and attaining menopause prematurely or before the natural age, can lead to amplification of the symptoms [21]. Reinforcing the neurological evidence of premature ovarian failure and cognitive outcomes of depression, we posit that depression could play a mediating role in the associations between premature or early menopause and cognitive impairment.
Mediating role of insomnia between premature failure of ovarian function and cognition
Ageing comes with difficulties with sleep caused by many factors such as multimorbidity, ageing process, increased medication use and others [22,23,24,25]. Insomnia is one of the common symptoms of menopause, along with other features like hot flushes, headache, body weakness, and depression [21].
Evidently, changes in sleep structure with aging are linked to cognitive decline, that is, decreased performance across various cognitive activities, including information processing speed, perceptual speed, executive functioning, concentration and attention, inhibitory functioning, and memory [26]. Per a growing body of literature, sleep facilitates synaptic plasticity, promotes procedural learning processes, and the consolidation of declarative memories and other cognitive functions [23, 27,28,29]. Thus, treating nocturnal insomnia may enhance cognitive performance and overall quality of life. With the understanding of the possibility of the woman’s early onset of ovarian failure influencing sleep disturbances, we hypothesize that insomnia would mediate the association between premature or early menopause and cognitive impairment.
Moderating role of smoking among premature failure of ovarian function, insomnia, depression and cognition
Lifestyle habits are a major factor that has an impact on a woman’s reproductive cycle [30]. In recent times, smoking cigarettes and in general tobacco consumption in any form is very common, and also a highlighted factor in damaging the reproductive life [31,32,33]. Studies have suggested that cigarette smoking leads to menstrual disorders and also has a moderate impact on ex-smokers. These studies showed that those who smoked had more risk of having oligomenorrhea and abnormal menstruation like irregularity and intermenstrual bleeding [34,35,36,37]. A 21-year follow-up study by [38], also found that the risk of early menopause is lower for those who do not smoke or have quit smoking.
Large cohort studies have shown that smoking reduces sleep quality and contributes to more insomnia-like symptoms [39,40,41,42]. Smoking leads to more severity of menopausal symptoms and poor sleep quality [43]. Along with sleep disturbances, there is also a prevalence of depressive symptoms due to smoking addiction [44,45,46,47]. Active smoking has neurotoxic effects on the brain, which leads to an increased risk of cognitive impairment, along with the development of underlying vascular disorders [48]. Longitudinal studies have shown that smoking is a major risk factor for cognitive decline with ageing [49]. Thus, it can be assumed that smoking moderates the pathways among early cessation of menopause, insomnia, depression and cognition.
Study hypothesis
Mediation hypothesis
There is a direct or indirect effect of premature or early menopause on cognitive health through insomnia and depression while controlling possible confounders.
Ha : Having premature or early menopause is associated with deteriorating cognitive health.
Hb : Having premature or early menopause is associated with higher depression levels, which leads to deteriorating cognitive health.
Hc : Having premature or early menopause is associated with higher insomnia symptoms, which leads to deteriorating cognitive health.
Moderated-mediation hypothesis
Hd : There is a direct or indirect effect of premature or early menopause on cognitive health through insomnia and depression, moderated by smoking (tobacco consumption) while controlling possible confounders.
Methods
Data source
The study utilized the Longitudinal Aging Study in India (LASI), 2017–2018, Wave 1 data. It is a multipurpose nationally-representative longitudinal survey that provides rich information on demographics, cognition, mental and physical health, and social networks of the ageing population in India. The survey collected extensive information on individuals’ physical, social and cognitive health (72,250) aged 45 and above across all states and union territories of India (excluding Sikkim). The survey used a multistage stratified area probability cluster sampling design wherein three-stage sampling was conducted for rural areas and a four-stage sampling design was conducted for urban areas to arrive at the eventual units of observation: older adults age 45 and above and their spouses irrespective of age. The goal was to select a representative sample in each stage of sample selection. India is a union comprising 30 states and 6 union territories with a population of 1,211 million [50] at the time of the survey. India’s states vary significantly with respect to geography, culture, population size, health conditions, demographics, and socio-economic characteristics.
The research design of the study is cross-sectional and descriptive, where the study attempts to analyze the secondary data to understand the effect of premature and early menopause on the psychosocial well-being of women in later ages.
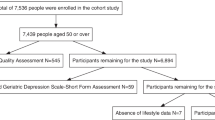
The present study has used data on women aged 45 and above and did not go through hysterectomy, which is a sample of 31,435 women. Their age of menopause is computed indirectly from the available questions and measured for premature (below 30 years) and early (40 to 44 years) menopause. The flowchart of the sample selection is given in Fig. 1.

Flowchart of sample selection
Ethical approval
The analysis is based on publicly available secondary data. As a result, no institutional review board (IRB) permission was necessary from the researchers. The LASI was carried out in accordance with ethical standards. As part of the ethical protocols, participants were given brochures that detailed the aim of the survey, privacy protection, health assessments, and safety precautions. The consent forms followed the Human Subjects Protection Act. The data is publicly accessible via https://www.iipsindia.ac.in/content/LASI-data.
Variable description
Dependent variable
Cognitive decline is a measure of ageing and a predictor of physical impairment and disability, which is likely to impact one’s capacity to work, make decisions, and interact socially [51]. Cognitive health was measured under five domains: memory, orientation, arithmetic, executive functioning, and object naming. Furthermore, a composite index was constructed as a part of the regular cognition module of the Health and Retirement Study (HRS) [52]. Overall, the cognitive score ranged from 3 to 43, where high scores indicated better cognitive function, with good reliability (Cronbach’s α = 0.93).
Mediators
To measure the presence of depressive symptoms, 10 Centre for Epidemiologic Studies Depression (CES-D) items were considered [53]. These items were divided into 7 negative symptoms and 3 positive symptoms, with a score ranging from 0 to 10. Furthermore, the negative symptoms were scored in ascending order, whereas the positive symptoms scoring were ranked in reverse order. Thus, high scores indicate severe depressive symptoms [52]. The Cronbach’s alpha reported is 0.85 in this analysis, indicating good reliability of the depression scale.
Insomnia is measured by four indicators, including, trouble falling asleep, waking up in the middle of the night, waking up too early, and feeling of unrest in the daytime. The categories occasionally (3–4 nights/ week) and frequently (5 or more nights per week) were considered to be insomniac. All were combined to measure insomnia and the score ranged from 0 to 4. The Cronbach’s alpha reported is 0.78 in this analysis, indicating good reliability of the insomnia indicator.
Independent variables
The main independent variable of the study is premature menopause and early menopause, which indicated the depletion of ovarian function. To measure the effect on late-life health, the woman’s age at menopause is checked is it is before the age of 45. Firstly, the condition is taken as the last menstrual month is more than 12 months before the survey year. The age at menopause is computed by.
Age at Menopause = Year of menopause - Birth year.
If the age at menopause is before the age of 40, then it is taken as premature menopause, while if the age at menopause is between 40 and 44 then it is taken as early menopause. Both of which are dummy variables, coded as ‘0’ and ‘1’ [54].
Moderator
The moderator used in the study is tobacco consumption or smoking in general. The respondent was asked about their tobacco consumption and smoking habit, and those who responded as yes were coded ‘1’ and no was coded as ‘0’.
Control variables
The present study adjusted socioeconomic, demographic, as well as, functional ability factors. The variables were kept as continuous or dichotomous for the convenience of the model. The age of the respondents and years of schooling were taken as continuous. The religion of the respondents was categorized as the Hindu and Other religions. The social class of the households was recoded as the schedule caste or schedule tribe, and other castes. The marital status was coded as currently married, and widowed/divorced/separated/not married.
The monthly per capita expenditure (MPCE) quintile was measured using household consumption data. Sets of 11 and 29 questions on the expenditures on food and non-food items, respectively, were used to canvas the sample households. Food expenditure was collected based on a reference period of seven days, and non-food expenditure was collected based on reference periods of 30 days and 365 days. Food and non-food expenditures have been standardized to the 30-day reference period (34). The monthly per capita consumption expenditure (MPCE) is computed and used as the summary measure of consumption. MPCE was then classified as poorest, poorer, middle, richer and richest.
In terms of health measurement, LASI has information on the prevalence of seven self-reported diagnosed chronic health conditions including, cardiovascular disease (including hypertension, heart diseases and stroke), lung disease, diabetes, bone or joint disease, psychiatric disorder and high cholesterol. The occurrence of the above diseases was coded as 0 ‘No’ and 1 ‘Yes.‘ Further, the number of cited diseases was used to calculate the ‘number of chronic diseases’ variable, which had a value ranging from 0 to 7, with a larger value suggesting more diseases.
The functional ability and mobility indicator consists of three variables, Activities of Daily Living (ADL), Instrumental Activities of Daily Living (IADL) and Mobility restriction. ADL refers to normal daily self-care activities, such as difficulty with dressing, walking across the room, bathing, eating, getting in or out of bed, or using the toilet (including getting up and down) [52]. Similarly, for the measurement of IADL, questions were asked if they were having any difficulties that were expected to last more than three months, such as preparing a hot meal, shopping for groceries, making a telephone call, taking medications, doing work around the house or garden, managing money (such as paying bills and keeping track of expenses), and getting around or finding an address in unfamiliar places [55]. Both the indices were coded dichotomous as 0 ‘No’ and 1 ‘Yes.‘ Lastly, a set of seven questions related to mobility: walking 100 yards, sitting for 2 h or more, getting up from a chair after sitting for long periods, climbing one flight of stairs without resting, stooping, kneeling or crouching, reaching or extending arms above shoulder level (either arm), pulling or pushing large objects, lifting or carrying weights over 10 pounds(such as a heavy bag of groceries), and picking up a coin from a table.
Statistical methods
Summary statistics was used to describe the study variables, that is, mean, standard deviations (continuous variables), frequency distribution and percentages (categorical variables). Bivariate analysis was carried out to examine the significant association between the independent variable (X), mediators (M1 & M2), moderator (W), control variables and the dependent variable (Y). Independent t-tests were used for categorical variables with two categories and one-way ANOVA F-test for more than 2 categories; whereas for continuous variables correlation tests were used. Since the control variables considered in the study could have potential confounding effects, hence they were controlled for in the moderated mediation models.
To test the mediation and moderated mediation hypothesis, the guidelines outlined by Preacher and Hayes (2008), have been followed. Firstly, the simple mediation model (Fig. 2a) was examined for the mediation hypothesis. The model analyses the relationship between premature or early menopause (X) and cognition (Y) mediated through insomnia (M1) and depression (M2), by the following steps: (i) regressing Y on X; (ii) regressing M1 and M2 on X; and (iii) regressing Y on X and M1 & M2. There are three requirements for mediation to exist, that includes- a is significant, indicating X is related to M1 and M2 (Eqs. 2 and 3); b is significant, indicating M1 and M2 is related to Y (Eq. 4); and if the indirect effect (a*b) c’ is not significant, but if significant then it indicates partial mediation (Fig. 2a). This model provides direct and indirect paths among the variables controlling the possible confounders.

Multiple moderated mediation model, where, ai’s and bi’s are the model coefficients and the estimated effects of moderator on the indirect effect of independent variable on dependent variable through mediator, is nothing but the coefficients of the interaction terms in the models
Then the proposed moderator variable was integrated into the model for testing the moderated mediation hypothesis. In all the other models, as shown in (Fig. 2b-f), we assessed the mediation effect of insomnia and depression moderated at categories of smoking (No, Yes), and interaction terms were computed in each model. Both the mediation and moderated mediation analysis were performed in SPSS based on 5000 bootstrapped samples (bias corrected) and sorting them to yield 95th percentile confidence interval.
Results
Table 1 shows that, in a sample of 31,435, the mean age of the sample is 60 years and ranges from 45 to 110 years. Majority of the respondents belonged to rural areas (68.9%), belonging to Hindu religion (8.6%), and poor MPCE quintile (22%). Around 29% of the women belonged to scheduled caste or scheduled tribe (SC/ST). The average years of schooling of the sample is 2.5 years, ranging from zero to 23 years The marital status of around 61% of respondents were married and 39% unmarried/divorced/widowed/separated. The mean functional abilities indicated by ADL and IADL was 0.4 (range 0–6) and 1.28 (range 0–7) respectively. The mobility restriction score ranging from 0 to 7 has a mean score of 2.56 (SD: 2.44). The mean number of chronic diseases were 1.04 (SD: 1.12) in a range of 0 to 7.
The age distribution of the age at menopause of the sample from Fig. 3, shows that mainly it is concentrated at the ages between 45 and 50. Approximately 8% of the older women reported that they had prematurely menopaused (< 40 years age), while 12.4% reported having early menopause (40 to 44 years age) (Table 1).

Distribution of age at menopause of the sample
The dependent variable, cognitive health score ranging from 3 to 43 has mean score of 22.4 (SD:6.87). The mediators depression has a mean score of 2.97 (SD: 1.77) and insomnia has a mean score of 0.9 (SD: 1.3). The moderator of the study is smoking or tobacco consumption, and 2.68% of the women.
The bivariate results are presented in Table 2, with tests of association between the study variables and dependent variable cognition. The results show that all the socioeconomic and demographic variables were significantly associated with cognition, except for religion. The age of the respondent and cognition is significantly negatively correlated (r= -0.31). The mean cognitive score was higher respondents in urban areas (26.2), not belonging to scheduled caste or scheduled tribe (24.98), and in highest MPCE quintile (25.48). Cognitive ability is also significantly positively correlated with years of schooling (r = 0.52).
The measures of functional abilities ADL (r=-0.15) and IADL (r=-0.28), also mobility restriction (r=-0.16) showed a significant negative correlation with cognition. Depression (r=-0.15) and insomnia (r= -0.11) showed a significantly strong negative correlation with cognition. The cognitive score is significantly lower (19.84) among those who consume tobacco. Premature menopause is significantly associated with cognition and the score is lower among those who had premature menopause (Table 2).
Depression and insomnia as mediators
The correlation matrix in Fig. 4, shows that the association between the mediators is positive, that is with increasing levels of depression, insomnia increases too, and vice versa. The relationship between premature menopause (X) and cognition (Y) has been analyzed and observed if the relationship is mediated through insomnia (M1) and depression (M2), which has been presented in Table 3. The unstandardized regression coefficients (β) with significance and standard errors (SE) have been reported. Premature ovarian failure measured by premature menopause was negatively associated with cognition (β:-0.33; SE:0.12; p < 0.05), whereas positively associated with insomnia (β:0.18; SE:0.03; p < 0.001) and depression (β:0.25; SE:0.04; p < 0.001). Finally, depression and premature menopause both were concurrently included in the model, where depression was negatively associated with cognitive health (β:-0.27; SE:0.02; p < 0.001). When the mediators are included, the negative effect of premature menopause on cognition decreases and is significant at 1% level of significance (β:-0.25; SE:0.12; p < 0.01). The indirect effect of premature menopause on cognition which is mediated by insomnia and depression is -0.07 and significant. This indicates partial mediation of insomnia and depression between premature menopause and cognitive health, thus resulting in 21% variability of the total effect in cognitive health.
Similarly, the model was run for early menopause as well, and the effect on cognition was not significant. Though the coefficients for insomnia and depression were significant but that does not show any mediating effect, since the main relation between independent and dependent is not significant (Table S1).

Correlation Matrix among cognition, depression and insomnia scores
Tobacco consumption as a moderator
The relationship between premature menopause and cognition mediated through insomnia and depression and moderated by MPCE has been analyzed. Table 4 provides with unstandardized regression coefficients with significance and standard errors of the interaction terms in various moderated mediation models that estimated insomnia, depression and cognition. In model B and D, tobacco consumption or smoking is observed to be negatively related to cognitive function (β= -0.79; SE:0.08; p < 0.001), as well as in model E (β= -0.87; SE:0.16; p < 0.001) and F (β= -0.89; SE:0.16; p < 0.001). The significant effect of moderation of smoking is highest in model B and D, where all the effects in the model, including the interaction of premature menopause and smoking (β= -0.64; SE:0.12; p < 0.001). Model C and D shows that smoking has a significant negative association with depression (β=-0.08; SE:0.03; p < 0.001), although the relation of smoking and insomnia is not significant here. Interestingly, it can be observed that the interaction of moderator (smoking) with the mediators, insomnia (β=-0.17; SE:0.03; p < 0.01) and depression (β=-0.13; SE:0.01; p < 0.001), and is negatively associated with dependent variable (cognition) (Model E). In model F, the same interactions have lower negative coefficients. Overall, there is a moderating effect of smoking or tobacco consumption has a significant moderating effect in the pathways among premature menopause, depression, insomnia and cognition (Fig. 5).

Consolidated representation of the moderated multiple mediation model; Note: *** p < 0.001; **p < 0.01; * p < 0.05
Taking early menopause, the models were run similarly in this context as well, but the result was not significant in relation to early menopause and cognition (Table S2). Thus, the hypothesis for the present study is rejected in the case of early menopause.
As observed from Fig. 6a and b, showing the conditional indirect effects of premature menopause on cognition at different moderator levels (Smoking-No and Yes), there is a stronger mediation of insomnia as well as depression, among the women who do not smoke. Also, Fig. 5c shows the conditional direct effects of premature menopause on cognition at different moderator levels, where again there is a stronger mediation of both the mediators among the women who do not smoke. It can also be inferred from the plots that, with premature menopause coupled with more depression and insomnia, there is a depletion in cognitive function (Fig. 6).

Test of moderation model indicating that the regression slopes for the two categories of smoking -No and Yes
Discussion
The present study attempted to determine the effect of premature or early menopause on late-life cognitive health in India. The study hypothesized that insomnia and depression have a mediating role and that smoking or tobacco consumption has moderated the relationship between premature ovarian failure and cognitive decline. There exist limited studies using moderated mediation analysis in such public health research and this study is a major contribution to the literature. Overall, the study has shown significant results from premature menopause, while for early menopause the hypothesis was rejected. This indicates the severity of lower menopausal age and its effect on psychosocial health.
The study findings from mediation analysis indicated that insomnia and depression play a significant mediating role between premature menopause and cognitive health. Smoking was found to play a significant moderating role here, and it is worth noting that the effects were higher among smokers. The study has controlled for some of the possible confounding factors that include socio-economic and demographic factors, as well as ADL, IADL, mobility restriction and a number of chronic diseases.
The direct effect of a premature menopause on cognitive health, without any mediators or moderators, and controlling for the possible confounders, have shown that there is a negative impact. There have been no studies that focussed on how premature menopause can affect the cognitive function of women in the Indian context. Overall, too there exists scanty literature exploring this association. Among these studies, the results showed that earlier age at menopause leads to an earlier decline in cognitive function, which remains consistent with the current study results [13, 56].
The mediating role of insomnia and depression
A woman experiencing menopause have decreased production of estrogen which leads to symptoms of sleep problems or insomnia along with other prominent one like vaginal dryness, hot flushes, joint pain etc. There are also psychological symptoms like irritations, anxieties, extreme mood swings, depression and emotional turbulences [57]. Now when a woman is experiencing menopause at an early age, before 40s then it is due to premature ovarian insufficiency, and the aforementioned symptoms also occur to them.
A study by Ates et al. (2022), which is based on 62 women with premature ovarian insufficiency and 62 controls, in Turkey, found poor sleep quality and insomnia among the premature menopausal women than the controls [58]. The severity of depression and anxiety was also high among premature menopausal women. The present study findings also suggest an effect of a premature menopause on insomnia and depression, and the relationship is positively associated. There also exists a strong mediation effect of insomnia and depression between premature menopause and cognitive decline. Women with premature ovarian failure also have low sex steroid levels and higher gonadotropic levels [59, 60]. They have more anxiety, depression, sensitivity and psychological distress [61]. All of this cumulatively affects cognitive health, and there is an increased risk of premature menopausal women of developing cognitive impairment or dementia [1, 62].
The moderating role of smoking
The present research constructed a moderated multiple mediation model for testing whether insomnia and depression mediated the relation between premature menopause and cognitive health, and whether this indirect relationship is moderated by smoking habit. The results indicated that smoking moderated this indirect link and the study hypothesis is accepted.
Cigarette smoking as a lifestyle factor has been consistently linked with earlier age at spontaneous menopause in previous studies. Smoking has an anti-oestrogenic impact due to the increased production of adrenal androgens, which leads to resistance of the oestrogen functions [63,64,65,66]. This overall jeopardizes the normal female hormonal balance, which affects the overall system. When smoking effect interacts with being prematurely menopaused, hormonal imbalances lead to sleep disturbances, cause depressive symptoms and ultimately affect cognitive function [67, 68].
Strengths and Limitations of the study
The study has several strengths owing to its national representativeness and methodological robustness. This study controlled for most of the factors that could confound the results. The use of the statistical tool ‘PROCESS’ which allows the analysis of mediation, moderation and moderated mediation models, is very less in the Indian context and especially in public health research, and this study adds on to it. However, the cross-sectional nature of the data limits the establishment of more causal relationships. Mental health issues and sleep problems can occur anytime due to other reasons as well. A longitudinal study in future in this context can yield better results.
Conclusion
The study is the first attempt in carrying out multiple mediations and moderated analysis to show the effect of premature ovarian failure on cognitive health, mediated through insomnia and depression and moderated by smoking habit. The findings emphasize the fact that smoking is associated with premature menopause, depression and insomnia. Women who experienced premature menopause has lower cognitive scores, depressive symptoms and insomnia symptoms, which were higher among those who consumed tobacco.
Practice recommendations
There needs to be more awareness and research on the topic of early onset of menopause. The study, strongly recommends the dissemination of information on the negative effects of tobacco consumption and making more informed choices to maintain a healthy life. More research into various methods and therapy is needed to determine the relationship between the age of early menopause and psychosocial well-being. Public awareness and education are crucial tools for maintaining healthy lives. However, greater study on the repercussions of premature or early menopause is strongly advised, given there are relatively few studies available in the Indian setting.
Data Availability
The analysis is based on secondary data available in public domain for research; thus, no approval was required from any institutional review board (IRB). The data is freely available upon request from https://iipsindia.ac.in/sites/default/files/LASI_DataRequestForm_0.pdf.
Point of contact: Sampurna Kundu, Email: sampurna34@gmail.com.
References
Faubion SS, Kuhle CL, Shuster LT, Rocca WA. Long-term health consequences of premature or early menopause and considerations for management. Climacteric. 2015;18:483–91.
Okeke T, Anyaehie U, Ezenyeaku C. Premature menopause. Ann Med Health Sci Res. 2013;3:90–5.
Dennerstein L, Lehert P, Guthrie JR, Burger HG. Modeling women’s health during the menopausal transition: a longitudinal analysis. Menopause. 2007;14:53–62.
Hogervorst E, Craig J, O’Donnell E. Cognition and mental health in menopause: a review. Best Pract Res Clin Obstet Gynecol. 2022;81:69–84.
Weber MT, Maki PM, McDermott MP. Cognition and mood in perimenopause: a systematic review and meta-analysis. J Steroid Biochem Mol Biol. 2014;142:90–8.
Woods NF, Mitchell ES, Adams C. Memory functioning among midlife women: observations from the seattle midlife women’s Health Study. Menopause. 2000;7:257–65.
Spencer JL, Waters EM, Romeo RD, Wood GE, Milner TA, McEwen BS. Uncovering the mechanisms of estrogen effects on hippocampal function. Front Neuroendocr. 2008;29:219–37.
Takeda S, Matsuzawa T. Age-Related brain atrophy: a study with computed Tomography1. J Gerontol. 1985;40:159–63.
Lethaby A, Hogervorst E, Richards M, Yesufu A, Yaffe K. Hormone replacement therapy for cognitive function in postmenopausal women. Cochrane Database of Systematic Reviews. 2008. https://doi.org/10.1002/14651858.CD003122.pub2.
Ryan J, Scali J, Carriere I, Ritchie K, Ancelin M-L. Hormonal treatment, mild cognitive impairment and Alzheimer’s disease. Int Psychogeriatr. 2008;20:47–56.
Lebrun CEI, Van Der Schouw YT, De Jong FH, Pols HAP, Grobbee DE, Lamberts SWJ. Endogenous oestrogens are related to cognition in healthy elderly women. Clin Endocrinol. 2005;63:50–5.
Ryan J, Stanczyk FZ, Dennerstein L, Mack WJ, Clark MS, Szoeke C, et al. Hormone levels and cognitive function in postmenopausal midlife women. Neurobiol Aging. 2012;33:617e11–22.
Ryan J, Scali J, Carrière I, Amieva H, Rouaud O, Berr C, et al. Impact of a premature menopause on cognitive function in later life. BJOG: An International Journal of Obstetrics & Gynaecology. 2014;121:1729–39.
Szyszkowicz M. Air Pollution and Emergency Department visits for Depression in Edmonton, Canada. Int J Occup Med Environ Health. 2007;20:241–5.
Murrough JW, Iacoviello B, Neumeister A, Charney DS, Iosifescu DV. Cognitive dysfunction in depression: Neurocircuitry and new therapeutic strategies. Neurobiol Learn Mem. 2011;96:553–63.
Deeks AA. Psychological aspects of menopause management. Best Pract Res Clin Endocrinol Metab. 2003;17:17–31.
Lam RW, Kennedy SH, McIntyre RS, Khullar A. Cognitive dysfunction in major depressive disorder: Effects on Psychosocial Functioning and Implications for treatment. Can J Psychiatry. 2014;59:649–54.
Crocco EA, Castro K, Loewenstein DA. How late-life Depression affects cognition: neural mechanisms. Curr Psychiatry Rep. 2010;12:34–8.
Hubbard NA, Hutchison JL, Turner M, Montroy J, Bowles RP, Rypma B. Depressive thoughts limit working memory capacity in dysphoria. Cogn Emot. 2016;30:193–209.
Shelton DJ, Kirwan CB. A possible negative influence of depression on the ability to overcome memory interference. Behav Brain Res. 2013;256:20–6.
Chimbira THK& KJ. Premature menopause. Cent Afr J Med. 1987;33:235–9.
Desforges JF, Prinz PN, Vitiello MV, Raskind MA, Thorpy MJ. Geriatrics: sleep disorders and aging. N Engl J Med. 1990;323:520–6.
Haimov I, Hanuka E, Horowitz Y. Chronic insomnia and cognitive functioning among older adults. Behav sleep Med. 2008;6:32–54.
Miner B, Kryger MH. Sleep in the Aging Population. Sleep Med Clin. 2017;12:31–8.
Neikrug AB, Ancoli-Israel S. Sleep Disorders in the older adult – A Mini-Review. Gerontology. 2010;56:181–9.
PARK. Cognitive aging: a primer. Psychology Press; 2000.
Benington JH, Frank MG. Cellular and molecular connections between sleep and synaptic plasticity. Prog Neurobiol. 2003;69:71–101.
Gais S, Born J. Low acetylcholine during slow-wave sleep is critical for declarative memory consolidation. Proceedings of the National Academy of Sciences. 2004;101:2140–4.
Walker MP, Stickgold R, Sleep. Memory, and plasticity. Ann Rev Psychol. 2006;57:139–66.
Kato I, Toniolo P, Akhmedkhanov A, Koenig KL, Shore R, Zeleniuch-Jacquotte A. Prospective study of factors influencing the onset of natural menopause. J Clin Epidemiol. 1998;51:1271–6.
Bromberger JT, Matthews KA, Kuller LH, Wing RR, Meilahn EN, Plantinga P. Prospective study of the determinants of age at Menopause. Am J Epidemiol. 1997;145:124–33.
Hardy R, Kuh D, Wadsworth M. Smoking, body mass index, socioeconomic status and the menopausal transition in a british national cohort. Int J Epidemiol. 2000;29:845–51.
Windham GC, Elkin EP, Swan SH, Waller KO, Fenster L. Cigarette smoking and effects on menstrual function. Obstet Gynecol. 1999;93:59–65.
Brown S, Vessey M, Stratton I. The influence of method of contraception and cigarette smoking on menstrual patterns. BJOG: An International Journal of Obstetrics & Gynaecology. 1988;95:905–10.
Hornsby PP, Wilcox AJ, Weinberg CR. Cigarette smoking and disturbance of menstrual function. Epidemiology. 1998;9:193–8.
Pettersson F, Fries H, Nillius SJ. Epidemiology of secondary amenorrhea: I. incidence and prevalence rates. Am J Obstet Gynecol. 1973;117:80–6.
Sloss EM, Frerichs RR. Smoking and Menstrual Disorders. Int J Epidemiol. 1983;12:107–9.
Hayatbakhsh MR, Clavarino A, Williams GM, Sina M, Najman JM. Cigarette smoking and age of menopause: a large prospective study. Maturitas. 2012;72:346–52.
Jaehne A, Unbehaun T, Feige B, Lutz UC, Batra A, Riemann D. How smoking affects sleep: a polysomnographical analysis. Sleep Med. 2012;13:1286–92.
Patten CA, Choi WS, Gillin JC, Pierce JP. Depressive symptoms and cigarette smoking Predict Development and persistence of sleep problems in US adolescents. Pediatrics. 2000;106:e23.
Riedel BW, Durrence HH, Lichstein KL, Taylor DJ, Bush AJ. The relation between smoking and sleep: the influence of Smoking Level, Health, and psychological variables. Behav sleep Med. 2004;2:63–78.
Wetter DW, Young TB. The relation between cigarette smoking and sleep disturbance. Prev Med. 1994;23:328–34.
Monterrosa-Castro A, Marrugo-Flórez M, Romero-Pérez I, Fernández-Alonso AM, Chedraui P, Pérez-López FR. Assessment of sleep quality and correlates in a large cohort of colombian women around menopause. Menopause. 2013;20:464–9.
Baglioni C, Spiegelhalder K, Lombardo C, Riemann D. Sleep and emotions: a focus on insomnia. Sleep Med Rev. 2010;14:227–38.
Gillin JC. Are sleep disturbances risk factors for anxiety, depressive and addictive disorders? Acta psychiatrica Scandinavica. 1998;98:39–43.
Riemann D. Insomnia and comorbid psychiatric disorders. Sleep Med. 2007;8:15–20.
Riemann D. Does Effective Management of Sleep Disorders reduce depressive symptoms and the risk of Depression? Drugs. 2009;69:43–64.
Lewis CR, Talboom JS, De Both MD, Schmidt AM, Naymik MA, Håberg AK, et al. Smoking is associated with impaired verbal learning and memory performance in women more than men. Sci Rep. 2021;11:10248.
Anstey KJ, von Sanden C, Salim A, O’Kearney R. Smoking as a risk factor for Dementia and Cognitive decline: a Meta-analysis of prospective studies. Am J Epidemiol. 2007;166:367–78.
Ministry of Home Affairs, India. Census 2011: provisional population totals. New Delhi: Office of Registrar General and Census Commissioner, Ministry of Home Affairs, Government of India; 2011.
Ofstedal M, Fisher G, Herzog AR, Herzog AR. Documentation of Cognitive Functioning Measures in the Health and Retirement Study. 2005.
International Institute for Population Sciences (IIPS). National Programme for, Health Care of Elderly (NPHCE), MoHFW, Public Health (HSPH) and the University of Southern California (USC). Longitudinal ageing study in India (LASI) Wave 1, 2017-18, India Report. International Institute for Population Sciences, Mumbai.; 2020.
Radloff LS, The CES-D, Scale. A self-report Depression Scale for Research in the General Population. Appl Psychol Meas. 1977;1:385–401.
Kundu S, Acharya SS. Study on depletion of ovarian function and late-life chronic diseases in India. Int J Gynecol Obstet. 2023. https://doi.org/10.1002/ijgo.14818.
Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179–86.
Kok HS, Kuh D, Cooper R, van der Schouw YT, Grobbee DE, Wadsworth MEJ, et al. Cognitive function across the life course and the menopausal transition in a british birth cohort. Menopause. 2006;13:19–27.
Adewuyi TDO, Akinade EA. Perception and attitudes of nigerian women towards menopause. Procedia - Social and Behavioral Sciences. 2010;5:1777–82.
Ates S, Aydın S, Ozcan P, Bakar RZ, Cetin C. Sleep, depression, anxiety and fatigue in women with premature ovarian insufficiency. J Psychosom Obstet Gynecol. 2022;0:1–6.
Nelson LM. Primary ovarian insufficiency. N Engl J Med. 2009;360:606–14.
Shuster LT, Rhodes DJ, Gostout BS, Grossardt BR, Rocca WA. Premature menopause or early menopause: long-term health consequences. Maturitas. 2010;65:161.
van der Stege JG, Groen H, van Zadelhoff SJN, Lambalk CB, Braat DDM, van Kasteren YM, et al. Decreased androgen concentrations and diminished general and sexual well-being in women with premature ovarian failure. Menopause. 2008;15:23–31.
Rocca WA, Bower JH, Maraganore DM, Ahlskog JE, Grossardt BR, de Andrade M, et al. Increased risk of cognitive impairment or dementia in women who underwent oophorectomy before menopause. Neurology. 2007;69:1074–83.
Gold EB. The timing of the age at which natural menopause occurs. Obstet Gynecol Clin N Am. 2011;38:425–40.
Hyland A, Piazza K, Hovey KM, Tindle HA, Manson JE, Messina C, et al. Associations between lifetime tobacco exposure with infertility and age at natural menopause: the women’s Health Initiative Observational Study. Tob Control. 2016;25:706–14.
Parente RC, Faerstein E, Celeste RK, Werneck GL. The relationship between smoking and age at the menopause: a systematic review. Maturitas. 2008;61:287–98.
Schoenaker DAJM, Jackson CA, Rowlands JV, Mishra GD. Socioeconomic position, lifestyle factors and age at natural menopause: a systematic review and meta-analyses of studies across six continents. Int J Epidemiol. 2014;43:1542–62.
Dalal PK, Agarwal M. Postmenopausal syndrome. Indian J Psychiatry. 2015;57(Suppl 2):222–32.
Mishra GD, Chung H-F, Cano A, Chedraui P, Goulis DG, Lopes P, et al. EMAS position statement: predictors of premature and early natural menopause. Maturitas. 2019;123:82–8.
Acknowledgements
The authors would like to thank Centre of Social Medicine and Community Health, Jawaharlal Nehru University, for allowing Ms. Sampurna Kundu to work on this topic for her PhD thesis. The authors would also like to acknowledge DST INSPIRE Fellowship for supporting Ms. Sampurna Kundu in her PhD journey.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
SK: Conceptualization, data curation, analysis and writing; SSA: Supervision, reviewing, and editing. All authors have critically reviewed and approved the final version of the manuscript submitted for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The analysis is based on secondary data available in the public domain for research; thus, no approval was required from any institutional review board (IRB). The survey agencies had conducted the fieldwork with prior consent from the respondents. The LASI was conducted in accordance with the relevant ethical guidelines and regulations.
Consent for publication
Not applicable.
Completing interest
The authors declare no conflict of interest among them.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kundu, S., Acharya, S.S. Linkage of premature and early menopause with psychosocial well-being: a moderated multiple mediation approach. BMC Psychol 11, 228 (2023). https://doi.org/10.1186/s40359-023-01267-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40359-023-01267-3