
Abstract
Background
Eating disorders have one of the highest mortality of all mental illnesses but are associated with low rates of screening and early intervention. In addition, there remains considerable uncertainty regarding the use of current standardised screening tools in measuring eating pathology in vegetarians and vegans. With these groups presenting as potential at-risk groups for disordered eating development, the present study aimed to develop and preliminary validate a novel eating disorder screening tool, the Vegetarian Vegan Eating Disorder Screener (V-EDS).
Methods
We utilised a mixed-methods approach, comprising four phases.
Results
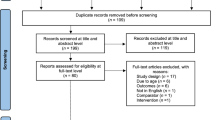
A conceptual framework was developed from 25 community, clinician, and lived experience interviews and used to derive a preliminary set of 163 items (Phase 1). Phase 2 piloted the items to establish face and content validity through cognitive debriefing interviews of 18 additional community, clinician, and lived experience participants, resulting in a reduced, revised questionnaire of 53 items. Phase 3 involved scale purification using Item Response Theory in analysis of 230 vegetarians and 230 vegans resulting in a further reduced 18-item questionnaire. Phase 4 validated the screening tool in a large community sample of 245 vegetarians and 405 vegans using traditional psychometric analysis, finding the V-EDS supports a unidimensional factor structure with excellent internal consistency (α = 0.95–0.96) and convergent validity (0.87–0.88), and moderate discriminate validity (0.45–0.55).
Conclusions
This study provided strong initial support for the psychometric validity and theoretical assumptions of the novel V-EDS screening tool. The V-EDS has the potential to increase early intervention rates for vegetarians and vegans experiencing eating disorder symptoms, further supporting advocacy and treatment approaches for these expanding dietary groups.
Plain English summary
The present study describes the development and preliminary validation of the first screening tool designed to uniquely assess eating disorder symptoms in individuals following a vegetarian or vegan diet. Following several development phases, the final version of the Vegetarian Vegan Eating Disorder Screener (V-EDS) comprises 18-items, with six dietary characteristic items and 12 eating disorder scored items. The current findings support excellent initial reliability and validity of the V-EDS. The V-EDS constitutes a promising tool that could potentially be integrated as a standalone measure for initial screening in clinical and research settings, but also for more comprehensive assessment when combined with other gold-standard eating disorder tools.
Similar content being viewed by others


Background
The number of people following a vegetarian or vegan diet is increasing around the globe, with estimates suggesting approximately 12% and 2% of the Australian population are vegetarian or vegan, respectively [1, 2]. These rates have been similarly demonstrated in other Western countries such as the United Kingdom and Germany [3, 4], and have been noted to be driven by a variety of reasons such as increasing animal welfare and environmental sustainability concerns, and the positive health benefits of consuming more plant-based foods [5, 6]. Within the eating disorder research field however, vegetarianism and veganism have long been thought to be related to an elevated risk of eating disorder symptoms [7,8,9,10]. For example, a degree of dietary restraint is necessary for vegetarian and vegan diets in order to consciously regulate the consumption of meat and/or animal products [11, 12], though this may not necessarily be driven by weight or shape control reasons (i.e., cognitive restraint; defined as the limited dietary intake to manage body weight). Yet indeed, the distinction between dietary restraint and cognitive restraint is often blurred within the vegetarian/vegan literature, positing that vegetarianism and veganism may act as a socially acceptable way to restrict food intake for weight control means and conceal disordered eating behaviours [13,14,15,16]. A systematic review of 48 studies examining the link between vegetarianism, veganism, and higher levels of disordered eating were unable to confirm this association with overall mixed findings [11]. The authors also noted that the majority of included studies had satisfactory to poor quality ratings, indicating a potential high risk of bias due to poor reporting of methodological and participant characteristics. For example, vegetarian and vegan samples were often disproportionately small relative to omnivore control groups or frequently grouped into one sample meaning that true associations between groups may have been masked.
The identification of eating disorders can be achieved through clinician-led interviews, such as the widely used Eating Disorder Examination Interview (EDE; [17]), or self-report questionnaires which are most commonly employed as screening or assessment tools. However, literature to date examining the use of eating disorder tools in strict vegetarian and vegan populations is scarce and focuses largely on the employment of self-report questionnaires [11, 18]. For example, Heiss, Boswell [19] were unable to support the original and alternate factor models of the gold-standard eating disorder tool, the Eating Disorder Examination-Questionnaire (EDE-Q; [20]) in a sample of 318 vegans, and further validated in separate analyses of vegetarians and vegans [6]. More positive findings have been reported for brief versions of the EDE-Q, with Zickgraf et al. [21] demonstrating strict measurement invariance of the Short-EDE-Q between non-vegetarians/vegans, weight-motivated vegetarians/vegans, and non-weight-motivated vegetarians/vegan university students. Heiss et al. [22] found adequate support for a brief three-factor version of the EDE-Q in vegans, however this model does not meet the minimum recommendations for factor analysis by containing just two items per latent variable [23]. Taken together, it is clear that exploring the factor structure of common eating disorder tools in these groups remains a critical future research avenue. These preliminary findings also potentially suggest that the theoretical constructs that eating disorder tools are designed to assess may not necessarily be suitable to capture the unique eating attitudes and behaviours of vegetarians and vegans. While it is the case that these tools were originally developed in omnivorous groups prior to the wide uptake of meat-free diets, their generalisability to vegetarian and vegan samples is often assumed [19]. Indeed, potentially confusing eating disorder measure items have been previously noted (see Table 1 in McLean et al. [11]), confirming concerns around the face validity of such measures.
There are several specialised tools to assess eating disorder symptoms in at-risk groups such as athletes and people with diabetes (e.g., [24, 25]). For example, the Diabetes Eating Problem Survey (DEPS-R) is a revised 16-item self-report tool developed to screen for disordered eating in people with type 1 diabetes. However, there is currently no available tool to uniquely target people who follow a vegetarian or vegan diet. Current measures may be inappropriate for use in vegetarians and vegans for several reasons. First, vegetarianism and veganism require a degree of dietary restraint to ensure meat and/or animal products are not consumed [11]. Current measures may not be able to decipher the fundamental driving factors behind dietary restraint versus cognitive restraint in these groups (e.g., to follow a vegetarian or vegan diet versus to influence weight or shape), resulting in overall higher levels of disordered eating measured. Second, current measures appear not to be able to identify eating behaviours that are unique to individuals following a vegetarian or vegan diet, such as displaying self-control around food in public or extensively reading ingredient lists of foods to ensure meat and/or animal products are not consumed [11]. For these reasons, it is potentially important to employ a screening tool designed specifically for individuals following a vegetarian or vegan diet when assessing eating disorder symptomology in these groups. A valid self-report tool designed for this purpose could allow clinicians and researchers a quick, inexpensive, and efficient way to potentially identify individuals who may need further evaluation or intervention. Therefore, the present study aimed to develop and preliminary validate a novel screening tool to identify eating disorder symptoms in individuals following a vegetarian and vegan diet.
Phase 1: Conceptual framework development
This stage of development aimed to create a conceptual framework for the presentation of eating disorder symptoms in vegetarians and vegans.
Methods
Transparency and openness
Methods for the following study phases were approved by Monash University Human Research Ethics Committee (Project ID: 30651).
Participants
A total of 25 participants, including vegetarians (n = 4) and vegans (n = 5) without lived eating disorder experience; vegetarians, vegans, and omnivores with lived eating disorder experience (n = 8); and psychologists (n = 4), and dieticians (n = 4) took part in either a semi-structured interview or focus group. Participants were recruited through various social media advertisements (e.g., private vegan Facebook groups and community noticeboards), established participant recruitment databases, and researchers’ professional networks (e.g., local and national eating disorder charities, colleagues within the eating disorder field). Participants were required to be 18 years or over, residing in Australia, and have access to video-conferencing equipment. Those taking part as a community-based participant (i.e., vegetarians, vegans, omnivores, lived experience) were required to adhere to a vegetarian or vegan diet and/or have lived eating disorder experience, whereas those taking part as a psychologist or dietician were required to have self-reported professional experience within the eating disorder field. Taking into consideration sample variability, participant availability, age, gender, dietary adherence, and if applicable, lived eating disorder history or experience in the field, participants were invited to take part in the study between March and April of 2022. Sample size was determined by data saturation whereby no new information emerged and no new themes could be generated within and between participant groups from the interviews [26].
Data collection
First, participants were required to complete a short expression of interest survey detailing basic demographic characteristic information, including age, gender, dietary adherence, and eating disorder history if applicable. If inclusion criteria were met, community-based participants were invited to an individual semi-structured interview with two researchers hosted via video conferencing platform, Zoom. Psychologist and dietician participants were invited to share their professional opinion on vegetarian and vegan eating attitudes and behaviours through a combination of focus groups and one-on-one interviews via Zoom. Each session lasted 30–60 min (M = 41.20, SD = 6.40) and were audio recorded.
The interview script was targeted towards understanding the eating habits of vegetarians and vegans, the relationship between vegetarianism, veganism, and disordered eating, and the applicability of eating disorder instruments in vegetarian and vegan groups. The psychologist and dietician interview script also focused on the diagnosis, treatment, and recovery of eating disorders in individuals following a vegetarian and vegan diet.
Data analysis
Interviews were first de-identified and transcribed by a member of the research team. Each transcript was then imported into an individual excel document with text grouped under each interview question, whereby data were analysed using an inductive approach. Three researchers were involved in data analysis, employing the following steps: transcripts were read for familiarity, relevant quotations were highlighted, codes were developed, and codes were merged into themes and subthemes. At the completion of data analysis, the research team discussed codes and themes generated, whereby those with discrepancies were deleted, added, or collapsed until consensus was reached [26].
Results
Participants in Phase 1 comprised primarily women (80.0%) and had an average age of 37.1 years (SD = 13.1; see Table 1).
Based on the interview data generated, eight key themes formed our conceptual framework for the presentation of eating disorder symptoms in vegetarians and vegans. As per Fig. 1, we note the inclusion of vegetarian and vegan-specific themes (e.g., dietary motivations), in addition to several core eating disorder themes (e.g., body dissatisfaction; see Additional File 1 for a description of themes).

V-EDS conceptual framework
Phase 2: Item generation and pretesting
This phase involved developing an exhaustive list of prospective items using the conceptual framework developed in Phase 1 and piloting them for discussion and feedback.
Methods
Participants
A total of 18 participants, including vegetarians, vegans, and omnivores with and without lived eating disorder experience, psychologists, and dieticians took part in semi-structured interviews. Participants were recruited using social media, snowballing techniques, and participant recruitment databases and were required to adhere to the same eligibility criteria as per Phase 1. Based on demographic variability, participants were invited to take part in the study via Zoom between July and August of 2022. A total of 38.9% of participants from Phase 1 also took part in this phase of the study, whereby sample size was determined by data saturation if no new information emerged and no new themes could be generated within and between participant groups [26].
Data collection
Data collection methods were identical to Phase 1 with each session lasting 30–60 min (M = 52.50, SD = 14.63). Cognitive debriefing techniques were integrated to examine the degree to which the developed items resonated with relevant personal or professional experiences, that the items were understandable, to rule out any unclear or ambiguous items, and to ensure readability of the items.
Data analysis
Interviews were first de-identified manually by a member of the research team, then transcribed using the confidential third-party platform, Otter.ai [27]. Additional data analysis processes followed that of Phase 1, with conclusions reached for each individual item by examining within and between subgroup data.
Results
Participants in Phase 2 comprised primarily women (80.0%) and had an average age of 36.1 years (SD = 11.6; see Table 1). The process of item generation led to the creation of an exhaustive list of 163 items across the eight conceptual framework themes. We further examined current and widely available eating disorder screening tools, including the EDE-Q [20], SCOFF [28], Eating Pathology Symptoms Inventory (EPSI; [29]), and Eating Disorder Inventory (EDI; [30]), to confirm that key item themes had been integrated. However, this did not result in the addition of any new items. Finally, psychologists and dieticians were invited to nominate items that they considered to be missing from the list or required further clarification. Based on the interview data generated, pilot testing of the items resulted in a reduced, revised questionnaire of 53 items.
Phase 3: Testing and scale construction
This phase of development aimed to test the preliminary set of developed items on a large sample of participants to aid in item reduction and final scale formation.
Methods
Participants
Through social media advertisements and participant recruitment databases, a total of 961 participants were recruited to take part in an online survey. Inclusion criteria required that participants were 18 years or over and residing in Australia to be eligible. Dietary status was assessed using a two-tier classification previously described in McLean et al. [6]. Due to our specific focus on vegetarian and vegan eating behaviours, meat-reducers (i.e., flexitarians, pescatarians, semi-vegetarians) were excluded from the final dataset and all analyses (n = 80). This resulted in a sample of 881 participants, comprising 230 vegetarians and 651 vegans. As there were a great deal more vegan participants than vegetarians, a random subsample of 230 vegan participants were selected to make the sample size of each dietary group equitable [31]. This approach was taken to ensure the developed screening tool would be applicable to both groups, resulting in a final sample of 460 participants.
Measures
Demographic characteristic information including age, gender, ethnicity, religion, and highest completed education were collected. Participants who stated they followed a vegetarian or vegan diet were asked additional specific questions around their dietary adherence, including length of dietary adherence and dietary motivations, with possible categorical responses being animal welfare, family tradition, financial, health, spiritual beliefs, environment, weight control, food sensitivity or intolerance, and taste, texture, and /or smell preferences.
Participants responded to the preliminary 53-item self-report Vegetarian Vegan Eating Disorder Screener (V-EDS) designed to assess the unique eating disorder symptomology of vegetarians and vegans over the past seven days. The reference time of seven days was chosen to provide optimal recall accuracy and allow for the V-EDS to track changes of symptoms over a short timeframe. The preliminary V-EDS consisted of 11 dietary characteristic items designed to provide important information about the respondent’s dietary attitudes (e.g., “The thought of accidentally eating meat causes you significant distress”) along a 5-point Likert scale from strongly disagree to strongly agree. While these items do not inherently indicate eating pathology when considered in isolation, we discovered through Phase 1 and 2 interviews that these attitudes are important to the respondent’s history. The questionnaire is followed by 42 behavioural and attitudinal items (e.g., “Has the way you think about food become intrusive?”) designed to measure the presence of eating disorder pathology, rated along a 5-point Likert scale from no days to every day, with higher scores indicating higher eating disorder pathology.
Procedure
Participants were advertised with a link to the online survey titled “Development of a New Eating Disorder Screener for Vegetarians and Vegans” and presented with the Explanatory Statement to provide informed consent. To ensure high data quality, participants were directed to complete a Captcha, a simple arithmetic question presented as an image, and two attention checks presented throughout the survey [32]. If participants failed any of the above quality or attention checks, they were excluded from the online survey and their IP address was not allowed to re-enter the survey. Participants then responded to demographic characteristic information, their weight and height to calculate BMI (weight in kg/height in m2), and the V-EDS. Finally, participants noted if they had ever received an eating disorder or mental health diagnosis from a health professional. Participants were given the opportunity to enter the draw to win one of four $AU50 gift cards (~ $US35).
Statistical analysis
SPSS Version 27.0 [33] was used to conduct frequencies and descriptive statistics for participant demographic characteristics. Stata 17 software [34] was used to conduct Item Response Theory (IRT) analysis whereby the 42 scored V-EDS items were examined using two-parameter logistic (2PL) models in combined and separate vegetarian and vegan samples to estimate individual parameters for difficulty and discrimination. Items were deemed unacceptable if they had limited ability to discriminate between low- and high-ability participants or discrimination coefficients with p > 0.05. The 11 dietary characteristic items were not included in the IRT analysis as they are not designed to be scored along a measurement scale, but rather used to provide categorical insight into a respondent’s eating attitudes and behaviours when considered alongside the V-EDS scored items. The dietary characteristic items were assessed for final inclusion between the authorship group.
Results
In the present study, the most common primary motivation for adhering to a vegetarian diet was animal welfare (53.9%), the environment (19.6%), and taste, texture, and/or smell preferences (10.0%), with a median diet length of 10.0 years (IQR = 17.0). In the vegan sample, the most common primary dietary motivation was animal welfare (75.7%), health (8.3%), and the environment (7.8%), with a median diet length of 7.0 years (IQR = 7.0). Table 2 presents descriptive statistics for the overall sample and subgroups, and test statistic results.
In separate 2PL models of vegetarians and vegans, parameter estimates indicated that a number of items were not well-suited to measure the latent variable with poor discrimination and difficulty parameters. Such findings were compared between dietary groups, with items with the poorest parameter estimates iteratively removed until well-performing items were remaining. Next, items with similar wording (e.g., “Have you restricted large amounts of food to change the way your body looks?”, “Have you excluded large amounts of food to change the way your body looks?”) were compared between vegetarian, vegan, and combined 2PL models with poorer functioning items removed. This resulted in a reduced, revised questionnaire of 12 scored items. The final IRT of the reduced 12-item scale in a combined and separate sample of vegetarians and vegans showed the test information function was single-peaked and reached its maximum in the middle-left of the distribution of the latent variable. Several dietary characteristic items were also removed until a consensus of six items was reached between the authorship group. The removal of items was based on those which had similar wording or addressed a similar expected outcome.
Phase 4: Psychometric assessment
This phase of development aimed to conduct psychometric analysis of the final version of the developed scale to validate its use in a non-clinical community sample of vegetarians and vegans. In doing so, we elected to undertake exploratory factor analysis to discover the underlying factor structure of the V-EDS in separate groups of vegetarians and vegans. It is expected that the V-EDS will support good to excellent initial psychometric properties.
Methods
Participants
A total of 1095 participants were recruited through social media advertisements and participant recruitment databases to take part via an online survey. Participants were required to adhere to identical inclusion criteria as per Phase 3, with meat-reducers and omnivores excluded from all analyses (n = 445). This resulted in a final sample of 650 participants (vegan = 405, vegetarian = 245). A smaller subtest of the sample (n = 71, 10.9%) took part in a 14-day test–retest reliability study comprising a further 22 vegetarian and 49 vegan participants.
Measures
Similar to Phase 3, participants responded to demographic characteristic information and dietary adherence questions.
The final Vegetarian Vegan Eating Disorder Screener (V-EDS) is an 18-item self-report screening tool designed to assess the unique eating disorder symptomology of vegetarians and vegans over the past seven days (see Additional file 2). The V-EDS consists of 6 dietary characteristic items designed to provide important background information to the respondent’s dietary attitudes, rated along a 5-point Likert scale from strongly disagree to strongly agree. The dietary characteristic items are followed by 12 behavioural and attitudinal items (e.g., “Has the way you think about food become intrusive?”) designed to measure the presence of eating disorder pathology, rated along a 5-point Likert scale from no days to every day. Higher scores on the V-EDS indicated greater eating disorder pathology.
The Eating Disorder Examination-Questionnaire (EDE-Q; [20]) is a self-report tool designed to measure the attitudinal and behavioural symptoms of eating disorders over the past 28 days. The EDE-Q comprises 28 items, including 22 attitudinal items and six open-response behavioural frequency items, whereby participants respond to each attitudinal item (e.g., “Have you had a definite fear of losing control over eating?”) along a 7-point Likert scale ranging from not at all to markedly. A global score is calculated by summing the four subscales: Eating Concern, Weight Concern, Shape Concern, and Restraint, and dividing by four (i.e., the number of subscales), with higher scores indicating greater eating disorder pathology. The EDE-Q has demonstrated good internal consistency, with a score of 0.96 in the total sample for the present study. As the EDE-Q is the most widely recognised clinical tool and forms part of the eligibility criteria for Medicare-subsidised treatment in Australia, it was included in the present study to assess the convergent validity of the V-EDS.
The Depression, Anxiety, and Stress Scale (DASS-21; [35]) is a 21-item self-report scale designed to assess the negative emotions associated with depression, anxiety, and stress over the past seven days. Each negative emotional subscale contains seven items and are responded to along a 4-point Likert scale from never to almost always. A subscale score is calculated by summing the seven associated items and multiplying by two, with higher scores indicating greater negative emotions. The DASS-21 has demonstrated good internal consistency, with a score of 0.93, 0.84, and 0.89 for the Depression, Anxiety, and Stress subscales, respectively, in the total sample for the present study. As depression traits are shown to have moderate divergent patterns with eating disorders [36], the DASS-21 was included in the present study to examine the divergent validity of the V-EDS.
Procedure
As with Phase 3, participants were advertised with a link to the online survey and presented with the Explanatory Statement to provide informed consent. Participants then responded to demographic characteristic information, their weight and height to calculate BMI, and the V-EDS, EDE-Q, and DASS-21 in randomised order. Finally, participants noted if they had ever received an eating disorder or mental health diagnosis from a health professional and were given an opportunity to enter a gift card draw. Identical data quality processes were integrated as per Phase 3.
Statistical analysis
SPSS Version 27.0 [33] was used to conduct frequencies and descriptive statistics for participant demographic characteristics, reliabilities, validities, and exploratory factor analysis (EFA). The vegetarian and vegan samples each had one variable with missing data at random and was imputed with the variable median [37]. CFA was conducted separately for vegetarians and vegans to confirm fit of the V-EDS model discovered via Phase C. Diagonally weighted least squares was used as the estimation method as it provides a robust estimation when dealing with ordinal data that violates the assumption of multivariate normality [38]. Adequacy of model fit was evaluated by examining several fit indices as judged using a two-index presentation strategy [39]. Relative model fit was judged with a specific focus on Comparative Fit Index (CFI), with ≥ 0.90 being acceptable and ≥ 0.95 being excellent [39]. Absolute model fit was judged with a focus on point estimate of root mean square error of approximation (RMSEA), with < 0.05 demonstrating good fit, between 0.05 and 0.08 acceptable fit, and > 0.08 poor fit [40]. Information linked to other fit indices were also reported and considered, including x2 value, Tucker-Lewis Index (TLI), and standardised root mean square residual (SRMR; [41,42,43]).
Internal consistency of the 12 scored V-EDS items were calculated using Cronbach’s coefficient alpha (α) for each dietary group. Convergent and discriminant validity were calculated using Pearson correlations (r) between the V-ED scored items and scores on the EDE-Q and DASS-21 subscales, respectively, for each group. Due to an insufficient sample size required to obtain 95% confidence in the test–retest reliability arm [44], analyses were not conducted for this statistic.
Results
Descriptive statistics
In the present study, the most common primary motivation for adhering to a vegetarian diet was animal welfare (58.8%), the environment (16.3%), and taste, texture, and/or smell preferences (9.0%), with a median diet length of 10.0 years (IQR = 16.0). In the vegan sample, the most common primary motivation was animal welfare (79.8%), health (8.9%), and the environment (7.4%), with a median diet length of 8.0 years IQR = 8.0). Table 3 presents descriptive statistics for the overall sample and subgroups, and omnibus test results to compare the vegetarian and vegan groups.
Dietary characteristic items
Item 1: I’m motivated to eat my food choices for…?
This item aimed to understand the primary dietary motivation driving the respondent’s adherence to a vegetarian or vegan diet (Fig. 2). Respondents are presented with five categorical options shown to be the most common dietary motivations (e.g., [6]).

Item 1 response characteristics across dietary groups
Item 2: Your vegetarian/vegan diet is part of your identity
Item 2 aimed to examine the degree the respondent perceives their dietary adherence to be tied to their identity (Fig. 3). We found significant differences in scores between dietary groups (t(648) = -5.14, p < 0.001, d = 0.42), with vegans more likely to strongly agree with this item.

Item 2 response characteristics across dietary groups
Item 3: A balanced diet can include eating processed plant-based products (e.g., mock meats)
This item aimed to assess the respondent’s rigidity around the consumption of processed plant-based products which may provide insight into “clean eating” practices (i.e., a diet approach of eating primarily unprocessed and unrefined foods; [45]) often associated with vegetarian and vegan diets (Fig. 4). We found no significant differences in scores between dietary groups (t(648) = −1.45, p = 0.147, d = 0.12.

Item 3 response characteristics across dietary groups
Item 4: You are willing to introduce meat to your diet if it is vital for your survival
Item 4 was developed to explore the respondent’s openness to the introduction of meat if necessary for their physical and/or mental health as part of eating disorder recovery. If accompanied by higher V-EDS scores and subsequent diagnosis of an eating disorder, this item may provide clinicians with potential insights into the respondent’s receptiveness to the consumption of meat and can be used to approach future client discussions on the topic. We found significant differences in scores between dietary groups (t(648) = 3.85, p < 0.001, d = 0.31), with vegans demonstrating stronger disagreement with the sentiment (Fig. 5).

Item 4 response characteristics across dietary groups
Item 5: The thought of accidentally eating meat causes you significant distress
Item 5 explores a respondent’s potential aversion to the consumption of meat (Fig. 6). There were statistically significant differences in scores between dietary groups (t(648) = −5.20, p < 0.001, d = 0.42), with vegans demonstrating overall stronger agreement with the sentiment.

Item 5 response characteristics across dietary groups
Item 6: Removing meat and/or animal products from your diet allows you to control the way your body looks
This item was developed to pick up on whether a respondent may be engaging in a vegetarian or vegan diet for body modification reasons, and thus may be at a higher risk for eating disorder development (Fig. 7). There were no significant differences in scores between dietary groups (t(648) = −0.91, p = 0.364, d = 0.07).

Item 6 response characteristics across dietary groups
Confirmatory factor analysis
Model fit of the one-factor model was judged to be acceptable in separate analysis of vegetarians and vegans. See Table 4 for individual model fit indices across dietary groups.
Internal consistency and construct validity
Table 5 summarises the internal consistency reliability, convergent bivariate Pearson correlations with the EDE-Q global score, and discriminant bivariate Pearson correlations with the DASS-21 subscales across dietary groups. Internal consistency, as measured by Cronbach’s alpha, was excellent in separate vegan and vegetarian groups. Convergent correlations were very strong in strength, demonstrating excellent convergent validity of the V-EDS with the EDE-Q. Divergent correlations with the DASS-21 depression subscale was moderate in strength, demonstrating moderate discriminant validity.
Discussion
Eating disorders remain one of the most underdiagnosed mental illnesses, with early detection and intervention known to significantly improve the speed of recovery and symptom severity [46, 47]. Furthermore, some “normal” vegetarian and vegan eating attitudes and behaviours may overlap with eating disorder symptomology, and therefore such practices may be inappropriately captured by existing eating disorder instruments [11]. To address this gap, the present study employed a rigorous methodological design aimed at developing and preliminary validating a novel eating disorder screening tool for individuals following a vegetarian and vegan diet, the Vegetarian Vegan Eating Disorder Screener (V-EDS). The V-EDS was found to support a unidimensional model comprising six dietary characteristic items and 12 core behavioural and attitudinal items and there appear to be strong psychometric properties for use in non-clinical, community samples of vegetarians and vegans.
The V-EDS development relied on the personal and professional expertise of a wide range of participants across four phases of construct and item development. The V-EDS is a relatively brief, 18-item, self-administered screening tool designed to potentially identify eating disorder risk across clinical or research settings in individuals following a vegetarian or vegan diet. Demonstrating excellent psychometric properties, each item of the V-EDS was deemed to measure the same underlying dimension as supported by CFA. The V-EDS also correlated strongly with the widely employed diagnostic tool, the EDE-Q, and therefore may possibly, with further validation, be considered a candidate as a standalone measure or when combined with the EDE-Q for comprehensive assessment. The inclusion of the dietary characteristic items offers a novel distinguishing feature which can be used to assist healthcare professionals to understand how the patient’s dietary attitudes may integrate with their eating disorder symptomology. Developed from themes generated during in-depth interviews with eating disorder clinicians, these items can be used as “conversation starters” to decipher a patient’s dietary adherence and attitudes. For example, if accompanied by higher V-EDS scores and subsequent diagnosis of an eating disorder, Item 4 (“You are willing to introduce meat to your diet if it is vital for your survival”) may provide clinicians with potential insight into their patient’s dietary flexibility which may be required to achieve recovery. Indeed, the importance of understanding dietary motivations and dietary flexibility within the context of a vegetarian and vegan diet emerged as important themes in this study and may provide insight into a patient’s eating disorder practices [48, 49]. For example, if a patient is motivated to adhere to a vegetarian or vegan diet for animal welfare or ecological concerns, do they incorporate other ethical lifestyle practices, such as eliminating products tested on animals or prioritising sustainability. It could also be useful to explore whether the client places additional dietary restrictions within the context of their vegetarian or vegan diet. Ultimately the V-EDS could potentially fill a critical gap as a psychometrically-sound screening tool to detect and explore eating disorder risk among individuals who follow a vegetarian or vegan diet.
A screening instrument for the detection of eating disorder risk in vegetarians and vegans potentially offers a number of valuable opportunities. While dietary status may not necessarily be a risk factor for the development of an eating disorder, adherence to a vegetarian and vegan diet may provide an advantageous avenue to permit disordered eating behaviours in already vulnerable people [11]. The V-EDS can provide healthcare professionals with a potential starting point to begin to decipher their patient’s dietary adherence from their eating disorder symptomology. We encourage clinicians to explore their patient’s dietary adherence in a way that is sensitive, non-judgemental, and non-assumptive to allow for their beliefs to be respected but also challenged in a therapeutic manner. Next, the V-EDS can be used to encourage discussions related to vegetarian and vegan nutrition care to ensure the patient is meeting minimum dietary requirements. Last, the V-EDS may be used as a tool for specialised vegetarian and vegan eating disorder training. For example, the V-EDS could be included as part of professional development workshops for clinicians learning about the assessment and treatment of eating disorders in these growing populations.
Strengths
This study developed, to our knowledge, the first eating disorder screening tool to specifically examine eating disorder risk in individuals who follow a vegetarian or vegan diet. We employed a rigorous methodological design that relied on critical input and review from a diverse participant group, including vegetarians, vegans, individuals with lived eating disorder experience, dieticians, and psychologists. Furthermore, each phase of this study recruited large sample sizes in accordance with minimum sample recommendations [50, 51]. Finally, the V-EDS may potentially overcome limitations of other commonly employed eating disorder tools to incorporate effective, quick, and inexpensive administration and scoring which provides reliable and valid results. While further research and validation are very much needed, the V-EDS may be a potential candidate for implementation in both healthcare and research settings [52].
Limitations and future research
A limitation of this study is that we relied on the recruitment of convenience sampling through established participant recruitment databases, personal and professional networks, and social media groups. As a result, the generalisability of the findings, and therefore validation of the V-EDS, is limited to broader populations of vegetarians and vegans, including those who adhere to their diet for religious and/or cultural reasons. Next, a large portion of the sample in Phase 3 and 4 self-reported as having either a current or previous eating disorder diagnosis. This is likely a reflection of the targeted nature of our recruitment advertising via social media and therefore is subject to sampling bias. In addition, we categorised vegetarian and vegan participants according to Asher, Green [53] multistep classification. Ultimately, this process allowed for the collection of “clean” vegetarian and vegan samples [6], however does place value on dietary patterns over self-identity which may have influenced the interpretation of participant responses. Furthermore, this study is preliminary in nature, and therefore we were unable to conduct a full suite of psychometric properties of the V-EDS across all participant groups and demographics. We encourage future research to expand on the present study and examine the psychometric properties of the V-EDS in more diverse samples in terms of age, gender, ethnicity, geographic region, dietary motivations, and clinical background. Finally, we were unable to conduct test–retest reliability analysis due to insufficient sample size as a result of potential response bias. Future research should focus on assessing the consistency of the V-EDS across time points, but also administration methods (e.g., digital vs pen and paper) to determine whether the V-EDS can be used to track progress through eating disorder recovery.
Conclusion
This study aimed to develop and preliminary validate a novel eating disorder screening tool for use in individuals following a vegetarian or vegan diet. We developed an 18-item tool, comprising six dietary characteristic items and 12 eating disorder scored items which demonstrated excellent initial psychometric properties. The V-EDS constitutes a promising instrument that could potentially be integrated as a standalone measure for initial screening in clinical and research settings, but also for more comprehensive assessment when combined with other gold-standard eating disorder tools, such as the EDE-Q and clinical interview. Ultimately, to our knowledge, the development of the V-EDS as the first eating disorder tool to capture unique vegetarian and vegan eating disorder symptomology offers an important step forward in understanding the complex relationship between vegetarianism, veganism, and eating disorders. Future research could build on our preliminary work and further validate the V-EDS across a wider range of diverse samples, including clinical backgrounds.
Availability of data and materials
The datasets generated and/or analysed from this study cannot be made available in line with ethics compliance.
References
Roy Morgan. Rise in vegetarianism not halting the march of obesity. [Place Unknown]; 2019.
Vegan Australia. Frequently aksed questions about veganism Sydney (AU): Vegan Australia; n.d. [Available from: https://www.veganaustralia.org.au/faq].
YouGov. Dietary choices of Brits United Kingdom: YouGov; 2021 [Available from: https://yougov.co.uk/topics/society/trackers/dietery-choices-of-brits-eg-vegeterian-flexitarian-meat-eater-etc.].
Motrøen M. The Orkla sustainable life barometer. Orkla: Orkla; 2019.
Craig WJ. Health effects of vegan diets. Am J Clin Nutr. 2009;89(5):1627–33.
McLean CP, Lavale A, Kulkarni J, Sharp G. Psychometric properties and factor structure of the Eating Disorder Examination-Questionnaire in omnivores, vegetarians, and vegans. Body Image. 2022;43:374–84.
Kadambari R, Cowers S, Crisp A. Some correlates of vegetarianism in anorexia nervosa. Int J Eat Disord. 1986;5(3):539–44.
O’Connor MA, Touyz SW, Dunn SM, Beumont PJ. Vegetarianism in anorexia nervosa? A review of 116 consecutive cases. Med J Aust. 1987;147(11–12):540–2.
Liskov TP, Gay LJ, Fairchild MM. Vegetarianism as a potential indicator of eating disorders among dietetic internship graduates. J Am Dietetic Assoc. 1996;96(9).
McLean CP, Kulkarni J, Sharp G. Eating disorders and meat avoidance: a call to understand the “why” instead of the “what.” Aust N Z J Psychiatry. 2022;56(6):731–2.
McLean CP, Kulkarni J, Sharp G. Disordered eating and the meat-avoidance spectrum: a systematic review and clinical implications. Eat Weight Disord. 2022;27:2347–75.
Timko CA, Hormes JM, Chubski J. Will the real vegetarian please stand up? An investigation of dietary restraint and eating disorder symptoms in vegetarians versus non-vegetarians. Appetite. 2012;58(3):982–90.
Zuromski KL, Witte TK, Smith AR, Goodwin N, Bodell LP, Bartlett M, et al. Increased prevalence of vegetarianism among women with eating pathology. Eat Behav. 2015;19:24–7.
Trautmann J, Rau SI, Wilson MA, Walters C. Vegetarian students in their first year of college: are they at risk for restrictive or disordered eating behaviors? Coll Stud J. 2008;42(2):340.
Bardone-Cone AM, Fitzsimmons-Craft EE, Harney MB, Maldonado CR, Lawson MA, Smith R, et al. The inter-relationships between vegetarianism and eating disorders among females. J Acad Nutr Diet. 2012;112(8):1247–52.
Klopp SA, Heiss CJ, Smith HS. Self-reported vegetarianism may be a marker for college women at risk for disordered eating. J Am Diet Assoc. 2003;103(6):745–7.
Cooper Z, Fairburn C. The Eating Disorder Examination: a semi-structured interview for the assessment of the specific psychopathology of eating disorders. Int J Eat Disord. 1987;6(1):1–8.
McLean CP, Kulkarni J, Sharp G. The 26-item eating attitudes test (EAT-26): psychometric properties and factor structure in vegetarians and vegans. Nutrients. 2023;15(2):297.
Heiss S, Boswell JF, Hormes JM. Confirmatory factor analysis of the Eating Disorder Examination-Questionnaire: a comparison of five factor solutions across vegan and omnivore participants. Int J Eat Disord. 2018;51(5):418–28.
Fairburn CG, Beglin SJ. Assessment of eating disorders: Interview or self-report questionnaire? Int J Eat Disord. 1994;16(4):363–70.
Zickgraf HF, Hazzard VM, O’Connor SM, Simone M, Williams-Kerver GA, Anderson LM, et al. Examining vegetarianism, weight motivations, and eating disorder psychopathology among college students. Int J Eat Disord. 2020;53(9):1506–14.
Heiss S, Timko CA, Hormes JM. Confirmatory factor analysis of the EDE-Q in vegans and omnivores: support for the brief three factor model. Eat Behav. 2020;39:101477.
Costello A, Osborne J. Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Pract Assess Res Eval. 2005;10.
Markowitz JT, Butler DA, Volkening LK, Antisdel JE, Anderson BJ, Laffel LMB. Brief screening tool for disordered eating in diabetes: internal consistency and external validity in a contemporary sample of pediatric patients with type 1 diabetes. Diabetes Care. 2010;33(3):495–500.
Hazzard VM, Schaefer LM, Mankowski A, Carson TL, Lipson SM, Fendrick C, et al. Development and validation of the eating disorders screen for athletes (EDSA): a brief screening tool for male and female athletes. Psychol Sport Exerc. 2020;50:101745.
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
Liang S, Fu Y. Otter.ai [Computer software]. Otter.ai; 2016.
Morgan JF, Reid F, Lacey JH. The SCOFF questionnaire: assessment of a new screening tool for eating disorders. BMJ. 2000;319(7223):1467–8.
Forbush KT, Wildes JE, Pollack LO, Dunbar D, Luo J, Patterson K, et al. Development and validation of the eating pathology symptoms inventory (EPSI). Psychol Assess. 2013;25(3):859–78.
Garner DM, Olmstead MP, Polivy J. Development and validation of a multidimensional eating disorder inventory for anorexia nervosa and bulimia. Int J Eat Disord. 1983;2(2):15–34.
Rusticus SA, Lovato CY. Impact of sample size and variability on the power and type I error rates of equivalence tests: a simulation study. Pract Assess Res Eval. 2014;19:11.
Douglas BD, Ewell PJ, Brauer M. Data quality in online human-subjects research: comparisons between MTurk, prolific, CloudResearch, Qualtrics, and SONA. PLoS ONE. 2023;18(3):e0279720.
IBM Corp. IBM SPSS Statistics for Macintosh, Version 27.0. IBM Corp: IBM Corp; 2020.
StataCorp. Stata statistical software: release 17. College Station, TX: StataCorp LLC.; 2021.
Lovibond PF, Lovibond SH. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the beck depression and anxiety inventories. Behav Res Ther. 1995;33(3):335–43.
Grilo CM, Reas DL, Hopwood CJ, Crosby RD. Factor structure and construct validity of the eating disorder examination-questionnaire in college students: further support for a modified brief version. Int J Eat Disord. 2015;48(3):284–9.
Zhang Z. Missing data imputation: focusing on single imputation. Ann Transl Med. 2016;4(1):9.
Li C-H. Confirmatory factor analysis with ordinal data: comparing robust maximum likelihood and diagonally weighted least squares. Behav Res Methods. 2015;48(3):936–49.
Hu L-T, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6(1):1–55.
Diamantopoulos A, Siguaw JA. Introducing LISREL: a guide for the uninitiated. London: London: SAGE Publications, Limited; 2000. xii–xii p.
Hair JF, Anderson RE, Tatham RL, Black WC. Multivariate data analysis. Prentice-Hall; 1995.
Kline P. A handbook of test construction: Introduction to psychometric design. London: Routledge; 1986.
Tucker LR, Lewis C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika. 1973;38(1):1–10.
Giraudeau B, Mary JY. Planning a reproducibility study: How many subjects and how many replicates per subject for an expected width of the 95 per cent confidence interval of the intraclass correlation coefficient. Stat Med. 2001;20(21):3205–14.
Sharp G, McLean CP. An Australian perspective on “clean” dietary labels: Commentary on Negowetti et al. (2021). Int J Eating Disorders. 2022;55(1):52–4.
Fukutomi A, Austin A, McClelland J, Brown A, Glennon D, Mountford V, et al. First episode rapid early intervention for eating disorders: a two-year follow-up. Early Interv Psychiatry. 2020;14(1):137–41.
Allen KL, Mountford VA, Elwyn R, Flynn M, Fursland A, Obeid N, et al. A framework for conceptualising early intervention for eating disorders. Eur Eat Disorder Rev. 2023;31(2):320–34.
Fuller SJ, Brown A, Rowley J, Elliott-Archer J. Veganism and eating disorders: assessment and management considerations. BJPsych Bull. 2022;46(2):116–20.
Heiss S, Coffino JA, Hormes JM. Eating and health behaviors in vegans compared to omnivores: dispelling common myths. Appetite. 2017;118:129–35.
MacCallum RC, Widaman KF, Zhang S, Hong S. Sample size in factor analysis. Psychol Methods. 1999;4(1):84–99.
Anthoine E, Moret L, Regnault A, Sébille V, Hardouin J. Sample size used to validate a scale: a review of publications on newly-developed patient reported outcomes measures. Health Qual Life Outcomes. 2014;12:176.
McCabe C, Claxton K, Culyer AJ. The NICE cost-effectiveness threshold: what it is and what that means. Pharmacoeconomics. 2008;26(9):733–44.
Asher K, Green C, Gutbrod H, Jewell M, Hale G, Bastian B. Study of current and former vegetarians and vegans: companion to the initial findings. [Place Unknown]: Faunalytics; 2014.
Acknowledgements
The authors would like to acknowledge the support of the participants who took part in this study.
Funding
This research was supported by an Australian Government Research Training Program (RTP) Scholarship.
Author information
Authors and Affiliations
Contributions
CM & GS conceptualised the project, CM, RS and JE assisted with data curation, CM, ZC, RS and JE assisted with formal analysis, CM and GS wrote the original draft. All authors assisted with reviewing and editing of the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Methods for this study were approved by Monash University Human Research Ethics Committee (Project ID: 30651) and participants provided informed consent prior to participating.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. V-EDS conceptual framework themes.
Additional file 2
. Vegetarian Vegan Eating Disorder Screener (V-EDS).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
McLean, C.P., Chen, Z., Song, R. et al. Development and preliminary validation of a novel eating disorder screening tool for vegetarians and vegans: the V-EDS. J Eat Disord 12, 4 (2024). https://doi.org/10.1186/s40337-024-00964-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40337-024-00964-7