
Abstract
Background
There is increasing interest in associations between cognitive impairments and clinical symptoms in Anorexia Nervosa (AN), however, the relationship with everyday function is unclear. The current review synthesizes existing data regarding associations between scores on tests of set-shifting and central coherence and functional outcome measures for individuals with AN.
Method
A systematic electronic database search yielded 13 studies which included participants with current or lifetime AN where scores on a neuropsychological test of set-shifting or central coherence were directly or indirectly compared to a functional outcome measure.
Results
Associations between set-shifting and central coherence performance measures and functional outcomes were limited in number and noted only in adult or mixed-age cohorts. Associations were noted at subscale level, suggesting they are specific in nature. In younger cohorts, assessments of executive functioning in everyday life appear sensitive to cognitive-behavioral flexibility issues.
Conclusions
Associations between cognitive performance and functional outcome have not been as systematically assessed in AN as in other psychiatric disorders. Key factors to address in future research include: (a) the use of function measures which are sensitive to both the level of impairment, and specific rather than general impairments (b) the ecological validity of measures, (c) the task impurity problem, especially in regard to cognitive flexibility assessment, and (d) the need to measure both cognitive deficits and strengths, because tests of specific cognitive processes may underestimate the ability to function in daily life due to compensatory strategies.
Similar content being viewed by others

Plain English summary
The current review gathers existing evidence regarding whether poor performance on tests of cognitive flexibility and detail-oriented processing are associated with difficulties in everyday function for people with Anorexia Nervosa. A literature search identified 13 articles which included data which address this question. The associations between poor performance on cognitive tests and day-to-day function were not strong, and were noted only in adult and mixed-aged groups. In younger samples, self-report measures of everyday cognitive skills appear to be more sensitive to function issues. Overall this review suggests that more research is needed to better understand how group differences on cognitive flexibility and detail-oriented processing tests relate to daily functioning for individuals with Anorexia Nervosa. It is recommended that future research should also measure cognitive strengths which may be used to compensate for cognitive weaknesses in everyday life.
Background
Anorexia Nervosa (AN) is an eating disorder (ED) characterized by extreme dietary restriction and other weight-loss behaviors, and a persistent fear of weight-gain despite significantly low weight [1]. The complex and serious physical and psychological health issues associated with AN result in significant health-related disability. Individuals with AN experience severe impairment in their social and occupational function [83], and longitudinal research highlights poor psychosocial functioning as a significant predictor of mortality [30].
In the past 10 years there has been increasing interest in neurocognitive functioning in ED research, with a recent ‘review of reviews’ finding 28 systematic and meta-analytic publications since 2010 [73]. A consistent finding in the literature is that adults with AN perform more poorly on neuropsychological tests of set-shifting and central coherence than healthy control groups [45, 100]. Set-shifting is the ability to shift focus between mental sets in response to changing demands, and is a measure of cognitive flexibility [21]. Central coherence refers to the normal tendency to process information in a global or holistic manner, rather than with excessive attention to detail. In contrast, a focus on detail at the expense of overall conceptual and contextual understanding, is an attentional bias known as weak central coherence [37]. Poor performance in these two areas forms a cognitive profile of inflexible, detail-focused processing which is consistent with clinical observations of cognitive-behavioral rigidity in individuals with AN. The Cognitive-Interpersonal Maintenance Model for AN [72] proposes poor set-shifting and weak central coherence underlie obsessive-compulsive traits, and together with socio-emotional avoidance, are key risk factors in both the aetiology and maintenance of the disorder. This inflexible cognitive style is further suggested to contribute to poor treatment engagement and response [84].
Taking a broader perspective, deficits in set-shifting and/or central coherence are present in other psychiatric disorders, prompting suggestions that the impairments may be a trans-diagnostic marker, or general risk-factor for a range of disorders. Within this wider psychiatric literature, cognitive deficits across the domains of attention, memory and executive function have been shown to predict both clinical and functional outcomes. Meta-analytic results suggest a substantial effect of general cognitive deficits on overall functional outcome in Schizophrenia [34], Bipolar Disorder [20], and a more limited general effect in Major Depressive Disorder [26]. In AN there has been no synthesis of the existing evidence of the effect of cognitive impairments on functional outcomes. However, a substantial body of research has focused on the measurement of cognitive impairments and possible associations with clinical characteristics of the disorder.
Set-shifting and central coherence impairments in AN
Set-shifting
A comprehensive meta-analysis which included 1394 participants with AN [100], found set-shifting deficits across a range of tasks of small to medium effect (Hedges' g = − 0.44). The effect was not consistent across included studies; 29 of 49 studies did not find significant differences between AN participants and healthy control cohorts. Effect sizes also varied greatly by measure; performance was most impaired in the Haptic Illusion task [87] (g = − 1.02), but not significantly different to controls in the Intra-Extra Dimensional Set Shift test [71] (g = − 0.17). There are suggestions that shifting is not impaired in all domains; participants with AN have demonstrated superior category switching compared to controls on tests of verbal fluency [77, 78].
Set-shifting is most commonly assessed using the Wisconsin Card Sort Task (WCST; [32]) on which individuals with AN often perform poorly. A meta-analysis of 22 studies which assessed set-shifting using the WCST found significant effect for adults (Cohen's d = .48) but not children (d = .25) [95]. This is consistent with meta-analysis across a range of executive function tasks which found effects were not significant for children with AN [40], however other meta-analytic results have not yielded significant differences between adolescent and adult participants [100] suggesting further clarification is needed.
Differences in shifting ability between AN Restricting subtype (AN-R) and Binge-Purge subtype (AN-BP) are inconsistent [73], however studies are often limited in their power to detect effects by sub-type. Splitting by sub-type, meta-analytic results of 11 studies including participants with AN-R suggest set-shifting deficits of medium effect (g = − 0.51) but across 6 studies the effect size for AN-BP was not significant (g = − 0.18) [100]. Overall, the literature suggests the presence of set-shifting impairments, but effects are not consistent, and vary greatly by measure.
Weak central coherence
Meta-analytic results of 7 studies using the Rey Osterreith Complex Figure Test (ROCFT; [61]) in AN indicate difficulties with global processing of medium to large effect (d = 0.63) [45, 47]. A synthesis of 5 studies using the Group Embedded Figures Test (GEFT; [98, 99]) shows a bias towards local processing, also of medium to large effect (d = 0.63) [45, 47]. Taken together, these results indicate weak central coherence in participants with AN. Significant differences in central coherence by AN subtype have been suggested, with AN-R participants noted to perform more poorly than AN-BP on the Wechsler Block Design and Object Assembly tasks [88], however the validity of the Block Design task as a central coherence measure has been questioned [45, 47, 50]. A meta-synthesis of studies using the ROCFT found participants with AN, and a group of unaffected relatives of AN patients both scored significantly lower on the central coherence index than healthy controls, but participants recovered from AN performed similarly to controls [46]. These findings are difficult to interpret, since poor performance by unaffected relatives suggest deficits may be trait-based, while similar performance to controls by the recovered group suggests issues may be state-dependent.
Associations between cognitive impairments and clinical characteristics of AN
Associations between cognitive impairments and clinical characteristics of the disorder provide support for the Cognitive-Interpersonal Maintenance Model for AN [72]. Poor set-shifting has been associated with a longer duration of illness, more severe ED rituals [69] and illness severity [84]. Weak central coherence has been associated with severity of illness, BMI and ED-related compulsions [70]. However, evidence regarding the relationship between cognitive impairments and clinical characteristics is quite inconsistent, which has prompted suggestions that deficits may be “clinically silent” [67]. The direction of causality is also difficult to interpret since cognitive flexibility is impacted by even short-term starvation in healthy participants [8, 63].
Cognitive Remediation Therapy (CRT) for AN is a treatment augmentation which aims to improve set-shifting and central coherence [81]. Since difficulties in these areas are thought to be both a risk factor in the maintenance of the disorder and also a barrier to engagement with treatment, remediation may improve clinical outcomes. Early reviews showed encouraging results and good patient acceptance in both adult and adolescent cohorts [82, 85]. However, a recent meta-analysis of randomized controlled trials of CRT versus control treatments showed no improvement in central coherence, ED symptoms or BMI, and mixed results for set-shifting which were unable to be synthesized due to the wide variety of measures used [35]. These results require cautious interpretation; since CRT is a relatively new intervention they include participants across a wide age group and both AN subtypes. Part of the CRT program involves applying new thinking styles to everyday life, and two studies which have included quality of life (QoL) outcomes [22, 90] have shown CRT is associated with improvement in ED-related QoL [35].
Functional outcome in AN
Functional impairment, or limitation in ability in areas of everyday living such as social, academic and occupational function, does not form part of the diagnostic criteria of AN. However, improvement in function is widely acknowledged as a key marker of recovery, and a self-report measure of function or QoL is often included as a secondary outcome in empirical research.
The Clinical Impairment Assessment (CIA; [10]), is a widely-used ED-specific self-report measure designed to assess functional impairments secondary to eating disorder symptoms. Weight and shape concerns and binge eating frequency have been shown to significantly predict CIA scores [66], and impairment on the CIA has also been demonstrated to increase as a function of illness severity according to BMI [18]. A recent network analysis of data from participants with AN found moderate correlations between ED symptoms at baseline and post-treatment CIA scores [24].
Results from assessments of QoL in AN are somewhat mixed, and may be complicated by the ego-syntonic nature of the disorder, wherein aspects of the disorder are perceived as congruent with the ideal self. Participants with AN-R have been noted to score similarly to healthy controls on a subjective QoL scale, possibly because items may be interpreted differently by AN patients whose concerns are not associated with low weight, and where weight increases towards a healthy range may be associated with a reduction in QoL ratings [58]. Mixed results appear to be more associated with shorter term follow-up measures, and shorter duration of illness [55], but in participants with severe and enduring AN, a close association between QoL, BMI and ED symptom severity has been demonstrated [5].
Functional impairment in AN is most commonly assessed as a secondary outcome, however longitudinal research has demonstrated that health-related QoL has a bi-directional relationship with ED symptoms - lower QoL scores predicted increases in ED symptoms over periods up to 4 years - suggesting QoL is a valid treatment target [55]. QoL, mood and social adjustment were the primary outcome measures in a randomized controlled trial of two alternative treatments for severe and enduring AN which demonstrated an unusually high retention rate, suggesting the approach may also increase patient engagement [86]. As mentioned earlier, CRT has been associated with preliminary, yet encouraging improvements in self-reported QoL in two studies [35]. These results suggest QoL could be more broadly explored as a treatment target in future CRT interventions.
The current review
Understanding the possible impact of cognitive factors on everyday function is important because functional improvements are milestones of recovery. Cognitive Remediation Therapy (CRT) is being implemented in AN, and it has been suggested that further evaluation of CRT should include whether it supports improvement in everyday functioning [11, 49]. To support the inclusion of broader functional outcomes in the evaluation of current therapies, a clearer understanding of the impact of cognitive inefficiencies on day-to-day function in AN is needed. To address this need, we conducted a systematic review of the literature to answer the question: Are poor set-shifting and central coherence associated with everyday function in Anorexia Nervosa?
Method
Inclusion and exclusion criteria
Inclusion criteria for studies were:
-
(a)
Participants met the criteria for current or lifetime Anorexia Nervosa.
-
(b)
Comparison between scores on a neuropsychological test of set-shifting or central coherence and scores on a measure of everyday function, or concurrent measurement of these variables compared to a healthy control group was reported.
A broad definition of everyday function which included social function, quality of life scales and measures of cognitive flexibility or detail-oriented processing in everyday life was used to maximize the breadth of studies included. We did not apply any age limit on participants because studies in AN often include a wide age range to maximize power.
Literature search
A search was conducted in November 2019 and updated in February 2021. Embase, Medline, PsychInfo and Scopus databases were searched using the following general and Medical Subject Headings (MeSH) search terms:
“anorexia nervosa” AND.
“daily function” OR “quality of life” OR “activities of daily living” OR “functional outcome” OR “employment” OR “independent living” OR “work and social adjustment scale” OR “Clinical impairment assessment” OR “eating disorders quality of life” OR “inventory of interpersonal problems” OR “Health related quality of life in eating disorders” OR “SF-36” OR “social function” OR “psychosocial function” OR “socio-emotional function” OR “social cognition” OR “ecological validity” OR “ecologically valid” OR “Behavioural assessment of dysexecutive syndrome” OR “Behaviour rating inventory of executive function” OR “detail and flexibility questionnaire” OR “D-Flex” AND.
Neurocogniti* OR neuropsych* OR “cognitive assessment” OR “neuropsychological assessment” OR “cognitive style” OR “cognitive deficit” OR “cognitive flexibility” OR “executive function” OR “ set shifting” OR “task switching” OR “central coherence” OR “Rey-Osterreith” OR “Wisconsin card sort” OR “Group embedded figures” OR “trail making” OR “Fragmented pictures” OR “Hayling” OR “Brixton” OR “Ravello Profile” OR “Delis Kaplan” OR “NEPSY*”.
Initial results were limited to English language, human subjects and peer-reviewed articles where possible. The database search was supplemented by a ProQuest Dissertations and Theses search using the above terms to search the full bibliographic record excluding the full text (NOFT), and a manual reference list search to identify any further articles relevant to the review. The review was performed according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) standards. Two reviewers (K.D. & S.T.) independently reviewed a subset of the articles at both abstract and full-text stage to determine eligibility.
Results
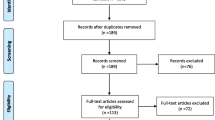
Thirteen articles met the inclusion criteria. The systematic search process is illustrated in Fig. 1. Included studies used a variety of measures of set-shifting, central coherence and functional outcome, and different methods of analysis, therefore a descriptive review was conducted. The included studies are summarized in Table 1. The table is organized according to the type of functional outcome measure used. The first section includes studies which used general function, social function and quality of life measures. The second section includes studies which employed measures of executive functioning in daily life.

PRISMA flow diagram for study selection
Quality assessment
Methodological quality of the included studies was assessed using a modified version of the Downs & Black Quality Index [23]. Items excluded from the original index were items relating to randomized controlled trials, as revised by Ferro and Speechley [28], and one item relating to description of response rate which were not useful assessment criteria for the current review. The amended 14-item index is presented in Table 2. Items were scored 1 for Yes (✓), and 0 for No (x) or Unable to determine (?). Maximum score was 14. The overall methodological quality of the studies included in the review was high. Two items were not well fulfilled; only two studies included a power calculation and less than half included information regarding the proportion of participants vs. those who were invited to participate.
Sample characteristics and measures
Participants in the studies included in the review were demographically heterogeneous. Most studies included only female participants, one study included two males [79] and two did not specify [39, 60]. Five studies included only adult participants and six studies describe their cohorts as children, adolescents or young people. One study included participants 16–42 years [75], and one included participants 12–47 years [94]. Eight studies included a healthy control comparison group.
Participants were also clinically heterogeneous. Most studies included only participants with AN; one study also included participants with Bulimia Nervosa, however clear subgroup analysis was provided [38]. Eight studies identified their participants by diagnostic subtype or included only one subtype. Studies included participants across a spectrum of stage and severity of AN, and included inpatient and outpatients cohorts. Studies varied in their exclusion criteria, however all excluded participants with other serious conditions, e.g. neurological or developmental disorders. Most studies did not exclude participants using psychopharmacological medication.
Power is an issue for AN research. Five studies had a sample size of under 25 participants; four of these were studies which included only children and/or adolescents, one was an adult cohort [36]. Some studies where analysis was undertaken by subtype or stage of illness also had low numbers of participants per group.
Studies included a variety of measures of set-shifting and central coherence, summarized in Table 3. Neurocognitive predictor measures were all performance-based, except the Detail and Flexibility Questionnaire (DFlex). The Wisconsin Card Sort Task (WCST) was the most common set-shifting measure, used in nine studies (however, note [67] use as a measure of general executive function). The Rey Osterreith Complex Figure Test (ROCFT) Central Coherence Index (CCI) was the most common measure of central coherence, also used in nine studies.
Studies included a variety of functional outcome measures, summarized in Table 4. Six studies included measures of social function, three of which were social cognition measures. Six studies used measures designed to assess executive function in daily life. Two studies assessed ED-specific functional impairment and two studies measured quality of life. Functional outcome measures in five studies were self-report only. Two studies included a parent-reported measure and two included a clinician-reported measure. Four studies included a performance-based function measure; three of these were the tests of social cognition and one was a measure of executive function in daily life.
Are poor set-shifting and central coherence associated with everyday function in anorexia nervosa?
Overall there were more associations between set-shifting and functional outcome measures than between central coherence and functional outcome measures. Seven studies reported a direct or indirect association between a set-shifting and a function measure, and three studies reported an association between a central coherence measure and a function measure. Interpretations based on grouping these associations by neurocognitive measures are very limited due to the wide range of functional outcome measures used, therefore results are grouped according to functional outcome.
Social function measures
Three studies used social cognition tasks to measure social functioning. In an adult sample with current AN, Harrison et al. [38] report higher WCST perseverative errors were associated with lower emotion recognition on the Reading the Mind in the Eyes test, however the association was not significant after Bonferroni correction.
Renwick et al. [67] tested adult participants with current AN on cognitive (WCST, Brixton Spatial Anticipation Test, ROCFT) and social cognitive (Reading the Mind in Films; RMIF) tests and used discriminant function analysis to identify three clusters representing a social-cognitive profile of high, mixed and poor performance. The cluster with poor overall performance is noted to have increased perseverative errors on the WCST, poor ROCFT copy trial scores and poor RMIF emotional theory of mind, which is interpreted as an indirect association between poor set-shifting, weak central coherence, and poor social-cognitive function.
Calderoni et al. [14] tested children/adolescents with AN-R using the full NEPSY-II battery which includes two shifting tests in the domain of attention and executive function, and three social perception tests. Direct associations between the set-shifting and social cognition tests were not included, however there were no differences between the AN-R patients and a healthy control group on the social perception tests (verbal theory of mind, contextual theory of mind and affect recognition). There were also no group differences on the overall domain of attention and executive function or the test of inhibition shifting, however performance on the response set-shifting test was marginally worse in the AN-R group.
Two studies used the Autism Diagnostic Observation Schedule (ADOS) as a measure of social functioning. Bentz et al. [9] tested an adolescent/young adult cohort comprised of individuals with first episode AN and those recovered from adolescent AN. A composite set-shifting score included the shift conditions from three Delis-Kaplan Executive Function System (D-KEFS) subtests: verbal fluency, design fluency and trail making. Composite set-shifting scores did not predict social function according to the ADOS total scores.
Westwood et al. [94] used ADOS Social Affect and Restricted and Repetitive Behavior scores to allocate a mixed age (12–47) cohort of participants with current AN into high vs. sub-clinical vs. no Autism Spectrum Disorder (ASD) symptoms groups. Participants were also tested on the WCST and the ROCFT. An increase in the percentage of perseverative errors on the WCST was associated with increased ASD symptoms, but the ROCFT was not associated with increased ASD symptoms.
One study used the Inventory of Interpersonal Problems (IIP-32). Talbot et al. [79] tested an adult cohort across stages of AN, including currently ill, weight-restored and fully recovered participants. A number of associations between WCST perseverative error (PE) scores and the IIP-32 are reported, however they are in the opposite direction to what may be expected. WCST PE scaled scores (where higher scores indicate better performance) were associated with higher scores on IIP-32 scores (which indicate greater interpersonal problems), in the subscales ‘Too dependent’, ‘Too aggressive’, ‘Hard to be involved’ and ‘Hard to be supportive’. Talbot et al. [79] also report two further associations in the opposite direction expected, between higher WCST Categories Completed (CC) and higher IIP-32 ‘Too dependent’ and ‘Too aggressive’. However, WCST CC is a measure of runs of 10 correct trials (when rule changes after 10 trials) and may be more indicative of general abstract reasoning, or the ability to learn how to ‘play the game’ [48]. Participants also completed the ROCFT, which demonstrated some relation to the IIP-32 in the predicted direction. Lower ROCFT Central Coherence Index and Order of Construction Index (OCI) were associated with greater endorsement of IIP-32 ‘Hard to be supportive’, and lower OCI was associated with higher IIP-32 ‘Hard to be involved’.
Measures of executive function in daily life
Six studies used assessments of executive functioning in daily life. Four studies utilized the self–report version of the Behavior Rating Inventory of Executive Function (BRIEF-SR) in younger cohorts, and two of those also included the parent form (BRIEF-PR).
Herbrich et al. [39] found no group differences between children/ adolescents with AN and healthy controls for the WCST, ROCFT or the Group Embedded Figures Test (GEFT). Participants with AN-R were faster on the Trail Making Test (TMT) than controls. BRIEF-SR scores for both AN subtypes and controls were all within normal range, however scores on the “Shift” subscale were graded, with AN-R participants indicating more issues with shifting than the controls, and AN-BP participants indicating more problems than AN-R.
van Noort, Kraus, Pfeiffer, Lehmkuhl, and Kappel [89] tested adolescents with AN and healthy control participants on the TMT, ROCFT and BRIEF-SR before and after Cognitive Remediation Therapy. There were no group differences for TMT or ROCFT at baseline. Irrespective of time point, participants with AN reported less flexibility than controls with medium-high effect on the BRIEF-SR subscales “Cognitive shift” and “Behavioral shift”.
Stedal and Dahlgren [76] tested adolescents with AN with the ‘Ravello Profile’ battery which includes the Brixton, ROCFT, and the shift trials from the Delis-Kaplan Executive Functioning System (D-KEFS) TMT, colour-word interference and verbal fluency tests. Participants also completed the BRIEF-SR, and their parents completed BRIEF-PF. Scores for all performance-based test scores and the BRIEF-SR and BRIEF-PF were within normal range.
McAnarney et al. [54] tested adolescents and young adults with AN-R (14–20 years) on the WCST, CANTAB Intra-Extra Dimensional Set Shift Test (IED), BRIEF-SR and BRIEF-PF. Participants with AN-R scored more poorly than a control group on WCST total errors, but perseverative error scores were not significantly worse. There were no significant group differences on the IED. Self and parent-reported difficulties with shifting were greater for AN-R participants than controls. At the subscale level, differences between AN-R participants and controls were greater for the BRIEF-SR Behavioral Shift than BRIEF-SR Cognitive Shift.
One study tested a mixed age cohort of participants with AN using the BADS and the WCST, TMT and ROCFT. Spitoni, Aragonaa, Bevacqua, Cotugno, and Antonucci [75] found perseverative errors on the WCST were higher for participants with AN than a control group, though the effect size was small. Performance on the TMT-B was slower than controls with small to medium effect. Participants with AN had a lower ROCFT Central Coherence Index (CCI) than controls with small to medium effects at 30 s and 20 min recall, however, the direct copy trial is the preferred CCI measure [46], and there was no group difference on direct copy trial performance. On the BADS battery, participants with AN performed similarly to controls in accuracy, however AN participants were slower than controls across most tasks with medium to very large effect sizes.
One study used the Detail and Flexibility Questionnaire (DFlex), a self-report measure of cognitive rigidity and attention to detail in daily life. Westwood et al. [94] found no significant difference in DFlex scores across high vs. sub-clinical vs. no ASD symptom groups, however on the cognitive rigidity subscale scores were significantly higher (more rigidity) in the high than the no ASD symptoms group.
Clinical impairment assessment
Two studies used the Clinical Impairment Assessment (CIA) to assess functional impairment secondary to ED symptoms. Renwick et al. [67] administered the CIA to an adult cohort with AN alongside the WCST, Brixton, and ROCFT (and social cognition measures, as described above), however a discriminant function analysis found no effect of cluster on CIA scores. Also in an adult cohort, Oldershaw et al. [60] found cognitive tests (WCST, Brixton, TMT, GEFT) did not predict CIA scores.
Quality of life measures
Two studies used QoL measures. In a cohort of adults with AN, Hamatani et al. [36] found greater Difficulty Maintaining Set (DMS) on the WCST Keio version was associated with lower scores on SF-36 Physical Component Summary (PCS). However, PCS scores for AN participants were not significantly different from a healthy control group, and DMS is not a standard set-shifting measure. DMS is the number of times an incorrect response occurs after 2–5 consecutive correct responses and may be more indicative of distractibility, as failing to maintain set has been inversely associated with performance on a vigilance task [29]. In the same group of participants, ROCFT central coherence index 30-min delayed recall was positively associated with SF-36 Mental Component Summary, however, as mentioned previously, the direct copy trial is considered to be best measure [46].
Talbot et al. [79] report an association between higher WCST Categories Completed (CC) and better financial QoL. However, as mentioned above, WCST CC is not a standard set-shifting measure and may be more indicative of general abstract reasoning or the ability to learn the task-rule.
Discussion
The current review synthesizes the existing evidence of associations between tests of set-shifting and central coherence and function measures in AN. Overall, the review highlights that this question has received little empirical focus, and of the studies which have assessed the question directly or indirectly, only a limited number of associations have been identified. Differences in the methodologies, measures and samples in the included studies complicate interpretation of the results, however it is possible to make a few general conclusions.
Firstly, the impact of set-shifting and central coherence deficits on functional outcomes in AN appears to be limited, and specific in nature. Levels of functional impairment have been compared to schizophrenia [4], however in schizophrenia neurocognitive deficits appear to exert a substantial general effect on overall functional outcome. The pattern of effect in AN represented by the current review is very different; associations between the cognitive tasks and functional outcomes were inconsistent, with many studies finding no association, and those noted were mostly at the subscale level, indicating a specific impact.
A second general conclusion is that the associations between set-shifting and central coherence deficits and functional outcome identified by the current review were in the adult samples, not the child/adolescent samples. There was generally little evidence of set-shifting and central coherence deficits on performance measures in the younger samples, which is largely consistent with meta-analytic results [40, 47]. However, significant differences between adolescents with AN and control participants were identified by the Behavior Rating Inventory of Executive Function (BRIEF).
Which is the third general conclusion; results of the current review suggest assessments of executive functioning in everyday life may be more sensitive to the cognitive-behavioral flexibility issues experienced by individuals with AN. This is particularly clear for the studies with child/adolescent participants where there were no group differences on the cognitive performance measures, but those that utilized the BRIEF identified that young people with AN report more difficulties with shifting in their daily lives than controls. These differences were noted using both the self-report and parent-report versions of the BRIEF. Results also suggest that behavioral shifting may be more problematic than cognitive shifting. This is consistent with neuroimaging research that suggests rigidity in AN may be secondary to impairments in behavioral response shifting rather than cognitive set-shifting [101].
Additionally, the one adult study which used a measure of executive functioning in everyday life, the Behavioral Assessment of Dysexecutive Syndrome (BADS), was the only study to find a general effect across measures. The BADS is comprised of tasks which are more complex and less structured than standard cognitive tests, involving not only the execution of a task, but planning, organizing, initiation and decision-making that is more similar to real-life task completion. Spitoni et al. [75] found adults with AN were just as accurate, but generally slower across most tasks, and concluded this may be due to perfectionism related to a detail-oriented processing style. The results are also consistent with a large synthesis of studies which questioned the nature of this general ‘slow-down’ effect seen in ED cohorts, which showed speed of information processing in simple reaction-time tasks was not impaired, but choice reaction time was slower [27].
Both the BRIEF and the BADS are test batteries designed to improve the ecological validity of executive function testing, an issue that has been extensively debated in the clinical and general population literature (see [16] for a review). Researchers in the eating disorder field have called for the use of more ecologically-valid measures to assess cognitive functioning in everyday tasks [15, 62, 76]. Objective performance tests with a specific focus on ecological validity have not been widely utilized in ED research, however measures of self-reported executive function are increasingly used, including ED-specific measures such as the Detail and Flexibility Questionnaire (D-flex; see Table 2), and a measure which encompasses both general and ED-specific flexibility, the Eating Disorder Flexibility Index (EDFLIX; [17]).
Although the current review suggests the nature of the impact of set-shifting and central coherence issues on functional outcome is specific, it is unable to identify which area of function is most affected. The review identified more associations with social function than other areas, however, it is not possible to conclude that social function is most impacted because many of the included studies were more focused on social difficulties than work or everyday activities. A focus on interpersonal problems is valid; patients with AN often experience reduced motivation for, and pleasure from, social interaction, and social-emotional avoidance is a key maintenance factor in the Cognitive-Interpersonal Maintenance Model for AN [72]. However, in terms of the question of possible associations with everyday function, investigations in other disorders suggest a focus on social impact may be an issue. Although results in schizophrenia suggest a general effect of neurocognitive performance on functional outcomes, there is a greater impact on occupational than social function [34]. And in obsessive-compulsive disorder, a more specific relationship has been identified; a retrospective in-patient study found poor set-shifting, measured by the Trail Making Test part B predicted poorer vocational outcome, but not social outcome or independent living status [64]. This raises the question: Could the use of outcome measures that are heavily weighted towards social items mean that the potential impact of cognitive difficulties is being missed by the outcome measure? Answering this question will require further systematic assessment of everyday function across social, workplace and everyday activities.
Although the quality of the studies included in the current review was generally high, the quality of the evidence regarding associations between the cognitive tests and functional outcome measures may be limited by several measurement and sample issues. For the majority of the included studies, associations with functional outcomes was not the primary outcome measure, therefore these issues are discussed not as criticisms of the studies, but rather to highlight methodological issues which may be addressed in future research.
Measurement issues
Studies included in the review primarily used the Wisconsin Card Sort Task (WCST) as the set-shifting measure. Nine studies used the WCST, and in three cases [36, 79, 94] the WCST was the only set-shifting measure. Seven studies reported an association between a set-shifting and a function measure, and in five cases the measure was the WCST. This may be an issue, because the WCST has a limited ability to isolate set-shifting ability from other areas of executive function, known as the task impurity problem. The problem arises because performance on even a simple behavioral task will involve cognitive processes outside the variable of interest [56]. Executive function broadly encompasses three areas: shifting flexibly between mental sets, updating working memory, and inhibition of a prepotent response [57]. The WCST dependent variable for set-shifting ability is number of perseverative errors, or errors in sorting where enough information to derive the correct sorting rule has been given. However, perseverative errors could occur due to difficulties with monitoring or updating working memory or inhibiting a response. In particular, the ability to inhibit a previously rewarded response, or reversal learning ability, has been raised as a problematic confound for ED research which uses the WCST [96]. Overall, these issues mean the WCST is best taken as a general measure of executive function, as it was used in one included study [67]. Concurrent measurement of working memory and inhibition, or a composite set-shifting measure to reduce task-related variability may improve the measurement of shifting-specific variance. One study included in the review [9] used a composite measure comprised of the shift conditions of verbal fluency, design fluency and trail making tests from the D-KEFS.
Included studies primarily used the Rey Osterreith Complex Figure Test (ROCFT) as the central coherence measure. Nine of the twelve studies which assessed central coherence used the ROCFT, and in six studies the ROCFT was the only central coherence measure [36, 67, 75, 76, 89, 94]. To provide a more comprehensive assessment of central coherence, utilizing both a global processing measure and a detail-oriented processing measure to demonstrate a bias away from global and towards local processing is useful. Three studies reported an association between a central coherence measure and a function measure, in all cases the measure was the ROCFT, however only one of these studies calculated central coherence index using the direct copy trial, which is the preferred measure [46].
A wide variety of functional outcome measures were used in the included studies and differences in their sensitivity to detect the impact of cognitive inefficiencies may account for the inconsistent findings. A meta-analysis of the associations between cognitive tests and everyday function in Bipolar Disorder notes the strength of correlations varied more due to functional measurement than cognitive domain [20]. General measures may be designed for populations where deficits are of greater magnitude or are more global in nature, and may therefore lack sensitivity to the level or pattern of impairment experienced by individuals with AN. Disorder-specific function measures such as the CIA may be more sensitive to functional impairments than general measures, however significant associations were not found using the CIA in this review. Null results may be partly explained by the general finding that associations between performance-based and self-report measures are low [52, 76], and most included studies used performance measures of set-shifting and central coherence, and many used self-report measures of functional outcome.
Four studies included a performance-based function measure, however, three of these were tests of social cognition only. The Reading the Mind in the Eyes test is a common test of social cognition, however it may be more strongly related to vocabulary than to emotion recognition or theory of mind ability [59].
Sample issues
Null effects may also be due to small sample sizes, or to the heterogeneity of the sample. Sample sizes in AN research are often low, and therefore it is usually only possible to avoid one of these issues. Significant differences in set-shifting and central coherence have been suggested between adults and children, by AN subtype, and between currently ill and recovered individuals, therefore investigating these groups separately is important. However, the power to detect effects was limited in the studies included in this review which sampled only children and/or adolescents, or split their analyses by diagnostic subtype. One study included a particularly wide age range of 12–47 years [94] which may be an issue because although maximum development in executive function occurs between 7 and 12 years old [65], executive function continues to develop until the early 20s, and age has been associated with performance on set-shifting and detail processing tasks [43]. However, age was included as a covariate in the analysis, and the WCST was the primary measure of set-shifting, on which performance is estimated to reach an adult level by around 12 years [65].
Finally, it is important to measure depression, anxiety and IQ (or an estimate of premorbid IQ) alongside cognitive measures. Evidence of the extent to which these factors affect performance on cognitive tasks is somewhat inconsistent in the general psychiatric literature, but results of a review in AN suggest set-shifting performance is negatively impacted by depression [2]. Most studies measured depression and anxiety, however three did not [75, 76, 79]. One study measured depression, but not anxiety [54]. An estimate of premorbid IQ was reported in all but one study [60].
There are also strengths and limitations to the current review. The database search included published conference abstracts and was supplemented by a dissertations and theses search. However, unpublished data and data not available in English was not included, and the review was not pre-registered. Although this may have biased the results, many of the studies included in the review report non-significant findings. To maximize the breadth of studies included and provide a rich analysis of the existing evidence in this area, the review included a broad range of functional outcome measures. However, differences in the methodologies employed in the included studies limit the conclusions which can be drawn from the review.
Extending beyond the scope of the current review, there may be issues related to the limited focus on set-shifting and central coherence deficits when investigating the possible impact of cognitive predictors on functional outcomes. A focus on these two deficits is not without reason - these are the areas where performance difficulties are consistently noted for participants with AN. However, the result is a very narrow measurement of potentially determining factors which does not consider the effects of areas of cognitive strength, or the possibility of compensatory strategy use. For example, individuals with AN show superior performance to control groups in verbal fluency and verbal category switching [77, 80], and verbal memory has been shown to be a strong predictor of everyday function in schizophrenia [34]. Data from one of the studies included in the current review showed performance on set-shifting and central coherence tasks did not predict ADOS social function – but higher verbal memory scores did [9]. Tests of specific cognitive processes may underestimate the ability to function in daily life if strong compensatory strategies like these are used [53]. Recent research found adolescent participants with weight-restored AN showed superior performance to a control group on a verbal and visual-motor set-shifting task, but when inhibition was controlled for in the analyses, their performance was worse, demonstrating strong inhibitory control was used as a compensatory mechanism [93]. Results such as this highlight that to understand the impact of neuropsychological tests on everyday life, a cognitive profile of not only deficits, but also the strengths which could compensate for them is needed. Research in this area could provide support for future cognitive strengths-based approaches to support functional recovery in AN, as has recently been suggested for first-episode psychosis [3].
Conclusion
Despite increasing interest in the assessment of possible links between cognitive impairments and clinical symptoms in AN, very little empirical work has been undertaken to explore whether there is relationship with everyday function. The current review synthesized research which has noted direct or indirect associations between set-shifting and central coherence tests and functional outcome measures in AN across a broad range of samples, measures and methodologies. The results of the review suggest that poor set-shifting and central coherence as measured by performance on standard cognitive tests has only a limited and specific effect on functional outcome, but that measures of executive functioning in daily life may be more sensitive to functional difficulties experienced by individuals with AN. Although the quality of the included studies was high, functional outcome was often a secondary measure, and associations between cognitive performance and functional outcome have not been as systematically assessed as is evident in other psychiatric disorders. However, as mentioned by Green [33], although cognitive research ‘looks inwards’, the studies included in this review also attempt to ‘look outwards’ to understand how cognitive inefficiencies impact functional outcomes for individuals with AN. This is important, because functional improvements are milestones of recovery which may increase patient engagement with therapy in AN. Future research in this area could improve current cognition-focused therapies by identifying broader therapeutic targets, and functional milestones by which the therapies can be evaluated.
Availability of data and materials
Not applicable.
Abbreviations
- ADOS:
-
Autism Diagnostic Schedule
- AN:
-
Anorexia Nervosa
- AN-BP:
-
Anorexia Nervosa Binge-Purge subtype
- AN-R:
-
Anorexia Nervosa Restricting subtype
- ASD:
-
Autism Spectrum Disorder
- BADS:
-
The Behavioral Assessment of Dysexecutive Syndrome
- BMI:
-
Body Mass Index
- BRIEF:
-
Behavior Rating Inventory of Executive Function
- CC:
-
Categories Completed
- CCI:
-
Central Coherence Index
- CIA:
-
Clinical Impairment Assessment
- CRT:
-
Cognitive Remediation Therapy
- DKEFS:
-
Delis-Kaplan Executive Function System
- DMS:
-
Difficulty Maintaining Set
- DFlex:
-
Detail and Flexibility Questionnaire
- ED:
-
Eating Disorder
- GEFT:
-
Group Embedded Figures Test
- IED:
-
Intra-Extra Dimensional set shift test
- IIP:
-
Inventory of Interpersonal Problems
- IQ:
-
Intelligence Quotient
- OCI:
-
Order of Construction Index
- PCS:
-
Physical Component Summary
- PE:
-
Perseverative Errors
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews
- QoL:
-
Quality of Life
- TMT:
-
Trail Making Test
- ROCFT:
-
Rey Osterreith Complex Figure Test
- WCST:
-
Wisconsin Card Sort Task
References
American Psychiatric Association. Diagnostic and statistical manual of mental disorders, fifth edition (DSM-5) (5th ed). Arlington: American Psychiatric Publishing; 2013.
Abbate-Daga G, Buzzichelli S, Marzola E, Aloi M, Amianto F, Fassino S. Does depression matter in neuropsychological performances in anorexia nervosa? A descriptive review. Int J Eat Disord. 2015;48(6):736–45. https://doi.org/10.1002/eat.22399.
Allott K, Steele P, Boyer F, de Winter A, Bryce S, Alvarez-Jimenez M, Phillips L. Cognitive strengths-based assessment and intervention in first-episode psychosis: a complementary approach to addressing functional recovery? Clin Psychol Rev. 2020;79:101871. https://doi.org/10.1016/j.cpr.2020.101871.
Arkell J, Robinson P. A pilot case series using qualitative and quantitative methods: biological, psychological and social outcome in severe and enduring eating disorder (anorexia nervosa). Int J Eat Disord. 2008;41(7):650–6. https://doi.org/10.1002/eat.20546.
Bamford B, Barras C, Sly R, Stiles-Shields C, Touyz S, Le Grange D, et al. Eating disorder symptoms and quality of life: where should clinicians place their focus in severe and enduring anorexia nervosa? Int J Eat Disord. 2015;48(1):133–8. https://doi.org/10.1002/eat.22327.
Barkham M, Hardy GE, Startup M. The IIP-32: a short version of the inventory of interpersonal problems. Br J Clin Psychol. 1996;35(1):21–35. https://doi.org/10.1111/j.2044-8260.1996.tb01159.x.
Baron-Cohen S, Wheelwright S, Hill J, Raste Y, Plumb I. The “Reading the mind in the eyes” test revised version: a study with Normal adults, and adults with Asperger syndrome or high-functioning autism. J Child Psychol Psychiatry. 2001;42(2):241–51. https://doi.org/10.1111/1469-7610.00715.
Benau EM, Orloff NC, Janke EA, Serpell L, Timko CA. A systematic review of the effects of experimental fasting on cognition☆. Appetite. 2014;77:52–61. https://doi.org/10.1016/j.appet.2014.02.014.
Bentz M, Jepsen JRM, Kjaersdam Telléus G, Moslet U, Pedersen T, Bulik CM, Plessen KJ. Neurocognitive functions and social functioning in young females with recent-onset anorexia nervosa and recovered individuals. J Eat Disord. 2017;5(1). https://doi.org/10.1186/s40337-017-0137-3.
Bohn K, Doll HA, Cooper Z, O'Connor M, Palmer RL, Fairburn CG. The measurement of impairment due to eating disorder psychopathology. Behav Res Ther. 2008;46(10):1105–10. https://doi.org/10.1016/j.brat.2008.06.012.
Brockmeyer T, Friederich H-C. Comprehending and fostering cognitive-behavioural flexibility in anorexia nervosa; 2015. p. 92–108.
Bucks RS. Trail-Making Test. In: Gellman MD, Turner JR, editors. Encyclopedia of behavioral medicine. New York: Springer New York; 2013. p. 1986–7.
Burgess PW, Shallice T. The hayling and brixton tests. London: Pearson; 1997.
Calderoni S, Muratori F, Leggero C, Narzisi A, Apicella F, Balottin U, et al. Neuropsychological functioning in children and adolescents with restrictive-type anorexia nervosa: an in-depth investigation with NEPSY-II. J Clin Exp Neuropsychol. 2013;35(2):167–79. https://doi.org/10.1080/13803395.2012.760536.
Carral-Fernández L, González-Blanch C, Goddard E, González-Gómez J, Benito-González P, Bustamante-Cruz E, Gómez Del Barrio A. Planning abilities in patients with anorexia nervosa compared with healthy controls. Clin Neuropsychol. 2016;30(2):228–42. https://doi.org/10.1080/13854046.2016.1147603.
Chaytor N, Schmitter-Edgecombe M. The ecological validity of neuropsychological tests: a review of the literature on everyday cognitive skills. Neuropsychol Rev. 2003;13(4):181–97. https://doi.org/10.1023/B:NERV.0000009483.91468.fb.
Dahlgren CL, Hage TW, Wonderlich JA, Stedal K. General and eating disorder specific flexibility: development and validation of the eating disorder flexibility index (EDFLIX) questionnaire. Front Psychol. 2019;10(663). https://doi.org/10.3389/fpsyg.2019.00663.
Dakanalis A, Alix Timko C, Colmegna F, Riva G, Clerici M. Evaluation of the DSM-5 severity ratings for anorexia nervosa in a clinical sample. Psychiatry Res. 2018;262:124–8. https://doi.org/10.1016/j.psychres.2018.02.009.
Delis DC, Kaplan E, Kramer JH. Delis-Kaplan executive function system; 2001.
Depp CA, Mausbach BT, Harmell AL, Savla GN, Bowie CR, Harvey PD, Patterson TL. Meta-analysis of the association between cognitive abilities and everyday functioning in bipolar disorder. Bipolar Disord. 2012;14(3):217–26. https://doi.org/10.1111/j.1399-5618.2012.01011.x.
Diamond A. Executive Functions. Annu Rev Psychol. 2013;64(1):135–68. https://doi.org/10.1146/annurev-psych-113011-143750.
Dingemans AE, Danner UN, Donker JM, Aardoom JJ, van Meer F, Tobias K, et al. The effectiveness of cognitive remediation therapy in patients with a severe or enduring eating disorder: a randomized controlled trial. Psychother Psychosom. 2014;83(1):29–36. https://doi.org/10.1159/000355240.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–84. https://doi.org/10.1136/jech.52.6.377.
Elliott H, Jones PJ, Schmidt U. Central symptoms predict Posttreatment outcomes and clinical impairment in anorexia nervosa: a network analysis. Clin Psychol Sci. 2019;8(1):139–54. https://doi.org/10.1177/2167702619865958.
Engel SG, Wittrock DA, Crosby RD, Wonderlich SA, Mitchell JE, Kolotkin RL. Development and psychometric validation of an eating disorder-specific health-related quality of life instrument. Int J Eat Disord. 2006;39(1):62–71. https://doi.org/10.1002/eat.20200.
Evans V, Iverson G, Yatham L, Lam R. The relationship between neurocognitive and psychosocial functioning in major depressive disorder. J Clin Psychiatry. 2014;75(12):1359–70. https://doi.org/10.4088/JCP.13r08939.
Ferraro FR, Kramer R, Weigel S. Speed of processing time slowing in eating disorders. J Gen Psychol. 2018;145(1):79–92.
Ferro MA, Speechley KN. Depressive symptoms among mothers of children with epilepsy: a review of prevalence, associated factors, and impact on children. Epilepsia. 2009;50(11):2344–54. https://doi.org/10.1111/j.1528-1167.2009.02276.x.
Figueroa, I., & Youmans, R. (2013). Failure to maintain set. Proceedings of the Human Factors and Ergonomics Society Annual Meeting, 57, 828-832. doi:https://doi.org/10.1177/1541931213571180.
Franko, D., Keshaviah, A., Eddy, K., Krishna, M., Davis, M., Keel, P., & Herzog, D. (2013). A Longitudinal Investigation of Mortality in Anorexia Nervosa and Bulimia Nervosa 170(8), 917–925. doi:https://doi.org/10.1176/appi.ajp.2013.12070868.
Gioia GA, Isquith PK, Roth RM. Behavior rating inventory for executive function. In: Kreutzer JS, DeLuca J, Caplan B, editors. Encyclopedia of clinical neuropsychology. Cham: Springer International Publishing; 2018. p. 532–8.
Grant DA, Berg E. A behavioral analysis of degree of reinforcement and ease of shifting to new responses in a Weigl-type card-sorting problem. J Exp Psychol. 1948;38(4):404–11. https://doi.org/10.1037/h0059831.
Green MF. What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatr. 1996;153(3):321–30.
Green MF, Llerena K, Kern RS. The “right stuff” revisited: what have we learned about the determinants of daily functioning in schizophrenia? Schizophrenia Bull. 2015;41(4):781–5. https://doi.org/10.1093/schbul/sbv018.
Hagan KE, Christensen KA, Forbush KT. A preliminary systematic review and meta-analysis of randomized-controlled trials of cognitive remediation therapy for anorexia nervosa. Eat Behav. 2020:37:101391.
Hamatani S, Tomotake M, Takeda T, Kameoka N, Kawabata M, Kubo H, et al. Influence of cognitive function on quality of life in anorexia nervosa patients. Psychiatry Clin Neurosci. 2017;71(5):328–35. https://doi.org/10.1111/pcn.12491.
Happé F. Autism: cognitive deficit or cognitive style? Trends Cogn Sci. 1999;3(6):216–22. https://doi.org/10.1016/S1364-6613(99)01318-2.
Harrison A, Tchanturia K, Naumann U, Treasure J. Social emotional functioning and cognitive styles in eating disorders. Br J Clin Psychol. 2012;51(3):261–79. https://doi.org/10.1111/j.2044-8260.2011.02026.x.
Herbrich L, Kappel V, van Noort BM, Winter S. Differences in set-shifting and central coherence across anorexia nervosa subtypes in children and adolescents. Eur Eat Disord Rev. 2018. https://doi.org/10.1002/erv.2605.
Hirst RB, Beard CL, Colby KA, Quittner Z, Mills BM, Lavender JM. Anorexia nervosa and bulimia nervosa: a meta-analysis of executive functioning. Neurosci Biobehav Rev. 2017;83:678–90. https://doi.org/10.1016/j.neubiorev.2017.08.011.
Kagan J. Reflection-impulsivity: the generality and dynamics of conceptual tempo. J Abnorm Psychol. 1966;71(1):17.
Kagan J, Rosman BL, Day D, Albert J, Phillips W. Information processing in the child: significance of analytic and reflective attitudes. Psychol Monogr Gen Appl. 1964;78(1):1.
Kalkut EL, Han SD, Lansing AE, Holdnack JA, Delis DC. Development of set-shifting ability from late childhood through early adulthood. Arch Clin Neuropsychol. 2009;24(6):565–74. https://doi.org/10.1093/arclin/acp048.
Kemp SL. NEPSY-ii. In: Kreutzer JS, DeLuca J, Caplan B, editors. Encyclopedia of clinical neuropsychology. New York: Springer New York; 2011. p. 1732–6.
Lang K, Lopez C, Stahl D, Tchanturia K, Treasure J. Central coherence in eating disorders: an updated systematic review and meta-analysis. World J Biol Psychiatry. 2014a;15(8):586–98. https://doi.org/10.3109/15622975.2014.909606.
Lang K, Roberts M, Harrison A, Lopez C, Goddard E, Khondoker M, et al. Central coherence in eating disorders: a synthesis of studies using the Rey Osterrieth complex figure test. Plos One. 2016;11(11).
Lang K, Stahl D, Espie J, Treasure J, Tchanturia K. Set shifting in children and adolescents with anorexia nervosa: an exploratory systematic review and meta-analysis. Int J Eat Disord. 2014b;47(4):394–9. https://doi.org/10.1002/eat.22235.
Lange F, Kip A, Klein T, Müller D, Seer C, Kopp B. Effects of rule uncertainty on cognitive flexibility in a card-sorting paradigm. Acta Psychol. 2018;190:53–64. https://doi.org/10.1016/j.actpsy.2018.07.002.
Leppanen J, Adamson J, Tchanturia K. Impact of Cognitive Remediation Therapy on Neurocognitive Processing in Anorexia Nervosa. 2018;9(96). https://doi.org/10.3389/fpsyt.2018.00096.
Lopez C, Tchanturia K, Stahl D, Treasure J. Central coherence in eating disorders: a systematic review. Psychol Med. 2008;38(10):1393–404. https://doi.org/10.1017/S0033291708003486.
Lord C, Risi S, Lambrecht L, Cook EH, Leventhal BL, DiLavore PC, et al. The autism diagnostic observation schedule—generic: a standard measure of social and communication deficits associated with the Spectrum of autism. J Autism Dev Disord. 2000;30(3):205–23. https://doi.org/10.1023/A:1005592401947.
Lounes N, Khan G, Tchanturia K. Assessment of cognitive flexibility in anorexia nervosa-self-report or experimental measure? A brief report. J Int Neuropsychol Soc, 2011;17(5):925-928. https://doi.org/10.1017/S1355617711000671.
Marcotte TD, Scott JC, Kamat R, Heaton RK. Neuropsychology and the prediction of everyday functioning Neuropsychology of everyday functioning. New York: The Guilford Press; 2010. p. 5–38.
McAnarney ER, Zarcone J, Singh P, Michels J, Welsh S, Litteer T, et al. Restrictive anorexia nervosa and set-shifting in adolescents: a biobehavioral Interface. J Adolesc Health. 2011;49(1):99–101. https://doi.org/10.1016/j.jadohealth.2010.11.259.
Mitchison D, Morin A, Mond J, Slewa-Younan S, Hay P. The bidirectional relationship between quality of life and eating disorder symptoms: a 9-year community-based study of Australian women. PLoS One. 2015;10(3):e0120591. https://doi.org/10.1371/journal.pone.0120591.
Miyake A, Friedman NP. The nature and organization of individual differences in executive functions: four general conclusions. 2012;21(1):8–14. https://doi.org/10.1177/0963721411429458.
Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The Unity and Diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cogn Psychol. 2000;41(1):49–100. https://doi.org/10.1006/cogp.1999.0734.
Mond JM, Owen C, Hay PJ, Rodgers B, Beumont PJV. Assessing quality of life in eating disorder patients. Qual Life Res. 2005;14(1):171–8. https://doi.org/10.1007/s11136-004-2657-y.
Olderbak S, Wilhelm O, Olaru G, Geiger M, Brenneman MW, Roberts RD. A psychometric analysis of the reading the mind in the eyes test: toward a brief form for research and applied settings. Front Psychol. 2015;6:1503. https://doi.org/10.3389/fpsyg.2015.01503.
Oldershaw A, Lavender T, Schmidt U. Are socio-emotional and neurocognitive functioning predictors of therapeutic outcomes for adults with anorexia nervosa? Eur Eat Disord Rev. 2018;26(4):346–59. https://doi.org/10.1002/erv.2602.
Osterrieth P. The test of copying a complex figure: a contribution to the study of perception and memory. Arch Psychol. 1944;30:206–356.
Øverås M, Kapstad H, Brunborg C, Landrø NI, Lask B. Are poor set-shifting abilities associated with a higher frequency of body checking in anorexia nervosa? J Eat Disord. 2015;3(1). https://doi.org/10.1186/s40337-015-0053-3.
Pender S, Gilbert S, Serpell L. The neuropsychology of starvation: set-shifting and central coherence in a fasted nonclinical sample. PLoS ONE, 9(10), e110743-undefined. 2014. https://doi.org/10.1371/journal.pone.0110743.
Perna G, Cavedini P, Harvey PD, Di Chiaro NV, Daccò S, Caldirola D. Does neuropsychological performance impact on real-life functional achievements in obsessive-compulsive disorder? A preliminary study. Int J Psychiatry Clin Pract. 2016;20(4):224–31. https://doi.org/10.1080/13651501.2016.1223856.
Peters S, Crone E. Cognitive flexibility in childhood and adolescence. In Grange J, Houghton G, editors. Task Switching and Cognitive Control. New York: Oxford University Press; 2014.
Reas DL, Ro O. Less symptomatic, but equally impaired: clinical impairment in restricting versus binge-eating/purging subtype of anorexia nervosa. Eat Behav. 2018;28:32–7. https://doi.org/10.1016/j.eatbeh.2017.12.004.
Renwick B, Musiat P, Lose A, DeJong H, Broadbent H, Kenyon M, et al. Neuro- and social-cognitive clustering highlights distinct profiles in adults with anorexia nervosa. Int J Eat Disord. 2015;48(1):26–34. https://doi.org/10.1002/eat.22366.
Roberts ME, Barthel FM, Lopez C, Tchanturia K, Treasure JL. Development and validation of the detail and flexibility questionnaire (DFlex) in eating disorders. Eat Behav. 2011;12(3):168–74. https://doi.org/10.1016/j.eatbeh.2011.04.001.
Roberts ME, Tchanturia K, Treasure JL. Exploring the neurocognitive signature of poor set-shifting in anorexia and bulimia nervosa. J Psychiatric Res. 2010;44(14):964–70. https://doi.org/10.1016/j.jpsychires.2010.03.001.
Roberts ME, Tchanturia K, Treasure JL. Is attention to detail a similarly strong candidate endophenotype for anorexia nervosa and bulimia nervosa? World J Biol Psychiatry. 2013;14(6):452–63. https://doi.org/10.3109/15622975.2011.639804.
Sahakian BJ, Owen AM. Computerized assessment in neuropsychiatry using CANTAB: discussion paper. J R Soc Med. 1992;85(7):399–402.
Schmidt U, Treasure J. Anorexia nervosa: valued and visible. A cognitive-interpersonal maintenance model and its implications for research and practice. 2006;45(3):343–66. https://doi.org/10.1348/014466505x53902.
Smith KE, Mason TB, Johnson JS, Lavender JM, Wonderlich SA. A systematic review of reviews of neurocognitive functioning in eating disorders: the state-of-the-literature and future directions Int J Eat Disord, no pagination specified. 2018. https://doi.org/10.1002/eat.22929.
Snodgrass JG, Vanderwart M. A standardized set of 260 pictures: norms for name agreement, image agreement, familiarity, and visual complexity. J Exp Psychol Hum Learn Mem. 1980;6(2):174.
Spitoni GF, Aragonaa M, Bevacqua S, Cotugno A, Antonucci G. An ecological approach to the behavioral assessment of executive functions in anorexia nervosa. Psychiatry Res. 2018;259:283–8. https://doi.org/10.1016/j.psychres.2017.10.029.
Stedal K, Dahlgren CL. Neuropsychological assessment in adolescents with anorexia nervosa – exploring the relationship between self-report and performance-based testing. J Eat Disord. 2015;3(1):27. https://doi.org/10.1186/s40337-015-0062-2.
Stedal K, Landro NI, Lask B. Verbal fluency in anorexia nervosa. Eat Weight Disord. 2013;18(2):151–6. https://doi.org/10.1007/s40519-013-0024-0.
Stedal K, Rose M, Frampton I, Landro NI, Lask B. The neuropsychological profile of children, adolescents, and young adults with anorexia nervosa. Arch Clin Neuropsychol. 2012;27(3):329–37. https://doi.org/10.1093/arclin/acs032.
Talbot A, Hay P, Touyz S. Exploring the relationship between cognitive style and daily functioning in patients with anorexia nervosa. Adv Eat Disord. 2015;3(3):300–10. https://doi.org/10.1080/21662630.2015.1057858.
Tamiya H, Ouchi A, Chen R, Miyazawa S, Akimoto Y, Kaneda Y, Sora I. Neurocognitive impairments are more severe in the binge-eating/purging anorexia nervosa subtype than in the restricting subtype. Front Psychiatry. 2018;9(APR). https://doi.org/10.3389/fpsyt.2018.00138.
Tchanturia K, Davies H, Reeder C, Wykes T. Cognitive remediation programme for anorexia nervosa: a manual for practitioners. London: Institute of Psychiatry; 2010.
Tchanturia K, Giombini L, Leppanen J, Kinnaird E. Evidence for cognitive remediation therapy in young people with anorexia nervosa: systematic review and meta-analysis of the literature. Eur Eat Disord Rev. 2017;25(4):227–36. https://doi.org/10.1002/erv.2522.
Tchanturia K, Hambrook D, Curtis H, Jones T, Lounes N, Fenn K, et al. Work and social adjustment in patients with anorexia nervosa. Compr Psychiatry. 2013;54(1):41–5. https://doi.org/10.1016/j.comppsych.2012.03.014.
Tchanturia K, Harrison A, Davies H, Roberts M, Oldershaw A, Nakazato M, et al. Cognitive flexibility and clinical severity in eating disorders. Plos One. 2011;6(6). https://doi.org/10.1371/journal.pone.0020462.
Tchanturia K, Lounes N, Holttum S. Cognitive remediation in anorexia nervosa and related conditions: a systematic review. Eur Eat Disord Rev. 2014;22(6):454–62. https://doi.org/10.1002/erv.2326.
Touyz S, Le Grange D, Lacey H, Hay P, Smith R, Maguire S, et al. Treating severe and enduring anorexia nervosa: a randomized controlled trial. Psychol Med. 2013;43(12):2501–11. https://doi.org/10.1017/S0033291713000949.
Uznadze DN. The psychology of set; 1966.
Van Autreve S, Vervaet M. Are there differences in central coherence and set shifting across the subtypes of anorexia nervosa?: a systematic review. J Nervous Ment Dis. 2015;203(10):774–80. https://doi.org/10.1097/NMD.0000000000000366.
van Noort BM, Kraus MKA, Pfeiffer E, Lehmkuhl U, Kappel V. Neuropsychological and Behavioural short-term effects of cognitive remediation therapy in adolescent anorexia nervosa: a pilot study. Eur Eat Disord Rev. 2016;24(1):69–74. https://doi.org/10.1002/erv.2383.
van Passel B, Danner UN, Dingemans AE, Aarts E, Sternheim LC, Becker ES, et al. Cognitive remediation therapy does not enhance treatment effect in obsessive-compulsive disorder and anorexia nervosa: a randomized controlled trial. Psychother Psychosom. 2020:1–14. https://doi.org/10.1159/000505733.
Ware, J. E. (2000). SF-36 Health Surv Update 25(24), 3130–3139.
Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): I. conceptual framework and item selection. Med Care. 1992;30(6):473–83.
Weinbach N, Bohon C, Lock J. Set-shifting in adolescents with weight-restored anorexia nervosa and their unaffected family members. J Psychiatr Res. 2019;112:71–6. https://doi.org/10.1016/j.jpsychires.2019.02.022.
Westwood H, Mandy W, Tchanturia K. The association between symptoms of autism and neuropsychological performance in females with anorexia nervosa. Psychiatry Res. 2017, 258:531–7. https://doi.org/10.1016/j.psychres.2017.09.005.
Westwood H, Stahl D, Mandy W, Tchanturia K. The set-shifting profiles of anorexia nervosa and autism spectrum disorder using the Wisconsin card sorting test: a systematic review and meta-analysis. Psychol Med. 2016;46(9):1809–27. https://doi.org/10.1017/S0033291716000581.
Wildes JE, Forbes EE, Marcus MD. Advancing research on cognitive flexibility in eating disorders: the importance of distinguishing attentional set-shifting and reversal learning. Int J Eat Disord. 2014;47(3):227–30. https://doi.org/10.1002/eat.22243.
Wilson BA, Evans JJ, Emslie H, Alderman N, Burgess P. The development of an ecologically valid test for assessing patients with a Dysexecutive syndrome. Neuropsychol Rehabil. 1998;8(3):213–28. https://doi.org/10.1080/713755570.
Witkin H, Oltman P, Raskin E, Karp S. Group embedded figures test manual. Redwood City: Mind Garden, Inc.; 2002.
Witkin HA. A manual for the embedded figures tests. Palo Alto: Consulting Psychologists Press; 1971.
Wu M, Brockmeyer T, Hartmann M, Skunde M, Herzog W, Friederich HC. Set-shifting ability across the spectrum of eating disorders and in overweight and obesity: a systematic review and meta-analysis. Psychol Med. 2014;44(16):3365–85. https://doi.org/10.1017/S0033291714000294.
Zastrow A, Kaiser S, Stippich C, Walther S, Herzog W, Tchanturia K, et al. Neural correlates of impaired cognitive-behavioral flexibility in anorexia nervosa. Am J Psychiatry. 2009;166(5):608–16. https://doi.org/10.1176/appi.ajp.2008.08050775.
Acknowledgements
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
KD, PH and ST conceptualized the review. KD conducted the literature search and wrote the manuscript. KD and ST screened studies for inclusion. All authors reviewed drafts of the manuscript. All authors contributed to, and have approved, the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
PH has prepared a report under contract for (July 2017) and received honoraria for education of psychiatrists from Takeda (formerly Shire) Pharmaceuticals.
ST has received travel grants, research grants and honoraria from Takeda for commissioned reports, public speaking and consultant work. He chairs their Australian Clinical Binge Eating Advisory Board.
KD has no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Dann, K.M., Hay, P. & Touyz, S. Are poor set-shifting and central coherence associated with everyday function in anorexia nervosa? A systematic review. J Eat Disord 9, 40 (2021). https://doi.org/10.1186/s40337-021-00392-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40337-021-00392-x