
Abstract
Background
Understanding the global spatiotemporal pattern of seasonal influenza is essential for influenza control and prevention. Available data on the updated global spatiotemporal pattern of seasonal influenza are scarce. This study aimed to assess the spatiotemporal pattern of seasonal influenza after the 2009 influenza pandemic.
Methods
Weekly influenza surveillance data in 86 countries from 2010 to 2017 were obtained from FluNet. First, the proportion of influenza A in total influenza viruses (PA) was calculated. Second, weekly numbers of influenza positive virus (A and B) were divided by the total number of samples processed to get weekly positive rates of influenza A (RWA) and influenza B (RWB). Third, the average positive rates of influenza A (RA) and influenza B (RB) for each country were calculated by averaging RWA, and RWB of 52 weeks. A Kruskal-Wallis test was conducted to examine if the year-to-year change in PA in all countries were significant, and a universal kriging method with linear semivariogram model was used to extrapolate RA and RB in all countries.
Results
PA ranged from 0.43 in Zambia to 0.98 in Belarus, and PA in countries with higher income was greater than those countries with lower income. The spatial patterns of high RB were the highest in sub-Saharan Africa, Asia-Pacific region and South America. RWA peaked in early weeks in temperate countries, and the peak of RWB occurred a bit later. There were some temperate countries with non-distinct influenza seasonality (e.g., Mauritius and Maldives) and some tropical/subtropical countries with distinct influenza seasonality (e.g., Chile and South Africa).
Conclusions
Influenza seasonality is not predictable in some temperate countries, and it is distinct in Chile, Argentina and South Africa, implying that the optimal timing for influenza vaccination needs to be chosen with caution in these unpredictable countries.
Similar content being viewed by others

Background
Seasonal influenza caused substantial morbidity and mortality worldwide, especially in elderly population and children aged under five years. It is estimated that, from 1999 to 2015, there were 291 243 to 645 832 seasonal influenza-associated respiratory deaths every year globally [1], causing a considerable health burden. For example, Australia witnessed its largest influenza season in 2017 since the 2009 pandemic, posing a substantial burden to primary care and hospitals [2]. Unveiling the global spatial pattern of seasonal influenza is essential for national and international decision making on influenza prevention and control.
Vaccination has been widely recognized as the most effective means of seasonal influenza prevention and can largely ease the burden caused by influenza. Identification of the optimal timing for vaccination is of great importance because vaccine-induced immunity wanes quickly after vaccination [3], and unfolding influenza seasonality is a crucial step for determining optimal vaccination timing. The widespread consensus in the literature is that influenza seasonality pattern is more ascertained in temperate regions/countries, but remains largely unclear and controversial in tropical and subtropical regions/countries [4,5,6]. It has been suggested that although influenza seasonality in tropics and subtropics is complicated, it might still be possible to group countries into similar zones for tailored and timely vaccination [7].
Prior studies have reported that the epidemiology (e.g., seasonality) of influenza A and influenza B may differ from each other [8,9,10], and the relative importance of influenza A and influenza B in driving seasonal influenza peak may vary across different countries [11]. For the development of strategic seasonal influenza control programs (e.g., using trivalent vaccines or quadrivalent vaccines), it is essential to assess the proportions of influenza A virus and influenza B virus in seasonal influenza virus.
Global, contemporaneous and comparative analysis of influenza data would help focus resources more effectively on areas/populations that need it most [12, 13]. Previous studies have reported the global spatial and temporal patterns of seasonal influenza up to 2015 [8, 14, 15], but very up-to-date information is not available in existing literature. Our study attempted to characterize the global spatial pattern of seasonal influenza A and B after 2009 influenza pandemic (i.e., from 2010 to 2017), to assess the proportions of influenza A virus and influenza B virus in total influenza virus, and to elucidate the seasonality of seasonal influenza A and B in temperate countries and tropical/subtropical countries. The specific objectives were three-fold: I). what was the proportion of influenza A virus in total influenza positive virus (PA) in each country; and whether there were any year-to-year changes in this proportion? II). what were the high risk regions of influenza A and influenza B? and III). what were the global seasonal patterns of influenza A and influenza B?
Methods
Data collection
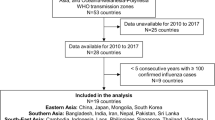
Weekly influenza surveillance data from 2010 to 2017 were collected from FluNet, an online database of WHO Global Influenza Surveillance Network for laboratory-confirmed influenza samples [6, 8]. Detailed information on FluNet can be found in WHO website (http://www.who.int/influenza/gisrs_laboratory/flunet/en/). FluNet data are real-life data. The diagnostic methods may vary widely between countries because of manpower and training issues, but FluNet data are the most widely available data that can be used by WHO surveillance to design the seasonal influenza vaccines. It is not easy practically (if not impossible) to unify the world’s approach to testing for these influenza viruses due to the resource variability and limitations. Thus, FluNet data are still quite valuable despite its limitations. Specifically, the data extracted in this study included the following variables: total number of influenza positive virus, total number of influenza A virus, total number of influenza B virus, and total number of samples processed. Countries with complete data of at least one year from 2010 to 2017 were selected, and in total there were 86 countries included in this study. The detailed influenza information on the countries selected, including time period(s), total number of samples processed, total number of influenza positive virus, total number of influenza A virus, and total number of influenza B virus, is depicted in Additional file 1: Table S1. World Bank categorized all countries into four income groups, including low income, lower middle income, upper middle income, and high income. We collected this information for each included country to assess if PA varied across different income groups (http://blogs.worldbank.org/opendata/new-country-classifications-income-level-2017-2018).
Data analysis
There were three analytical approaches corresponding to three objectives. First, for each country, total number of influenza A virus was divided by total number of influenza positive virus to get the proportion of influenza A virus in total influenza positive virus (PA). Data on 21 countries with complete data from 2010 to 2017 were used to present the year-to-year change in PA. The yearly PA data for each country were ratio and were not normally distributed (after normality test), so we conducted a Kruskal-Wallis test to check if the year-to-year changes in PA in all countries were statistically significant. Second, weekly numbers of influenza positive virus for influenza A and influenza B, as well as total number of samples processed, across all years were merged into 52 weeks in each country. Weekly numbers of influenza positive virus (influenza A and influenza B) were divided by the total number of samples processed to get weekly positive rates of influenza A (RWA), and influenza B (RWB). The average positive rates of influenza A (RA), and influenza B (RB) for each country were calculated by averaging RWA, and RWB of 52 weeks, and a kriging approach was used to extrapolate the average influenza positive rate in all countries globally. Specifically, we used the “universal” kriging method and the “linear” semivariogram model. Universal kriging is a powerful method which simultaneously estimates a trend and used the resulting errors for kriging. The equations for calculating PA, RWA, RWB, RA and RB, are presented in Table 1. Third, heat maps were plotted using RWA and RWB to present the seasonal patterns of influenza A and influenza B in temperate countries and tropical/subtropical countries. A cosinor function combined with Poisson regression was used to quantify the peak time and trough time of influenza A and influenza B [16].
Spatial mapping and kriging were conducted in ArcGIS 10.5 (ESRI Inc., Redlands, CA, USA), and all other analyses were done in R package 3.4.4 (https://www.r-project.org/).
Results
The global spatial pattern of PA and its temporal change
The proportion of influenza A virus in total influenza positive virus (PA) were illustrated in Fig. 1. The highest PA was in Belarus (upper-middle-income), Ethiopia (low-income), Iraq (upper-middle-income), and Venezuela (upper-middle-income). Specifically, PA was greater than 0.5 in all countries except for Zambia and Lebanon. Fig. 2 shows that PA was higher in high-income and upper-middle-income countries than low-income and lower-middle-income countries (P = 0.0015 in the Kruskal-Wallis test), although one of the four countries with the highest PA was a low-income country (i.e., Ethiopia). Fig. 3 shows that there were year-to-year changes in the relative proportions of influenza A virus. The Kruskal-Wallis test indicates that the year-to-year changes globally were not statistically significant (P = 0.5271).

Global pattern of influenza A proportion

Influenza A proportion in countries from different income groups

Temporal change in influenza A proportion in 21 countries
The global spatial patterns of RA and RB
The global spatial patterns of RA and RB was shown in Fig. 4. The highest RA distributed in Venezuela, Bolivia, Nepal, Ethiopia and China, and the highest RB distributed in sub-Saharan Africa, Asia-Pacific region and South America.

Global pattern of influenza positive rate
The seasonal patterns of influenza a and influenza B
The seasonal patterns of RWA and RWB in temperate countries and tropical/subtropical countries by latitude were presented in Fig. 5. RWA and RWB peaked in early weeks of each year in most temperate countries except for Australia, New Caledonia, Mauritius, Maldives and Malaysia, and the peak weeks of RWA occurred earlier than influenza RWB. For most tropical/subtropical countries, influenza seasonality pattern was diverse (i.e., either having several peaks or occurring all year around). However, influenza seasonality was distinct in Chile, Argentina, and South Africa. The peak time and trough time of influenza in all selected countries quantified by cosinor function are presented in Table 2. The peak time and trough time varied considerably across different countries.

Seasonality of influenza A and B in temperate and tropical/subtropical countries
The seasonal patterns of RWA and RWB in 21 countries with complete data from 2010 to 2017 were shown in Additional file 2: Figure S1. Influenza seasonality in the two tropical/subtropical countries, i.e., Chile and Argentina, was steadily distinct across different years.
Discussion
This study used data up to 2017 and kriging approach to unravel the updated global spatial pattern of seasonal influenza. It quantified the proportion of influenza A virus in total influenza virus and modeled the peak times of influenza A and influenza B in each country from 2010 to 2017. Three findings are note-worthy. First, the highest PA was observed in Belarus, Ethiopia, Iraq, and Venezuela, and PA changed from year to year. Second, for influenza B, high risk regions distributed in sub-Saharan Africa, Asia-Pacific region and South America. Third, influenza seasonality was distinct in most temperate countries but there were some exceptions (e.g., Mauritius and Maldives), and influenza seasonality was surprisingly distinct in some tropical/subtropical countries, including Chile, Argentina and South Africa.
Unsurprisingly, we observed that influenza A was the dominant subtype in almost all countries (except for Zambia and Lebanon). Notwithstanding, we found that the proportion of influenza B was greater than the proportion of influenza A in certain years in Malaysia, Nicaragua, Panama, Egypt, and Norway. Iuliano et al. estimated the global burden of influenza-associated respiratory deaths and reported that the highest mortality rate was found in sub-Saharan Africa and southeast Asia, and among those who are aged 75 years or older [1]. The high positive rate of influenza B that we observed in sub-Saharan Africa suggested that not only mortality but also morbidity in this region were high, calling for more influenza prevention resources to be allocated to this socioeconomically-disadvantaged region. Previous studies have also highlighted the necessity of building comprehensive influenza surveillance system in sub-Saharan Africa [17,18,19]. Regarding the influenza situation in Asia-Pacific region, some countries such as Australia and China had a high influenza positive rate (finding of the present study) but low/moderate mortality rate [1], implying a relatively good healthcare system in these countries but also suggesting a strong need to identify the national, regional, and local optimal vaccination timing for cost-effective influenza prevention (especially for China as it has wide latitude spans) [10], and to build up influenza early warning system which gives warning in a timely manner (e.g., internet-based early warning tools incorporating information collected through traditional surveillance system) [20]. Our prior works have suggested that early warning of infectious diseases using data from search engine (e.g., Google and Baidu) may shed some new light on infectious disease control [21, 22]. The constrains and barriers for influenza control and prevention in Asia-Pacific region are multifaceted (e.g., logistic and resourcing issues) [23], and preventing people in this region from influenza attacks requires concerted efforts from policy makers, public health officials, healthcare workers, and scientists.
The noticeable change of influenza seasonality in the included countries that we observed in this study, to some extent, indicates that there is no one-size-suits-all vaccination timing for tropical/subtropical countries and some temperate countries. Grouping tropical/subtropical countries into several zones for influenza vaccination might need much more detailed works (e.g., identifying the fundamental determinants behind the year-to-year change in seasonality etc.). A prior study investigating the global environmental drivers found that absolute humidity and temperature drive the outbreaks of seasonal influenza [24], and the season of influenza in Vietnam has been found coinciding with the rainy seasons [4], implying that future endeavors aiming to look at the relationships between climatic factors and influenza season in a regional or local scale in tropical and subtropical countries are warranted.
This study has two strengths. First, it unfolded the global spatial pattern of influenza positive rate, which may aid policy making in influenza control and prevention. Second, it identified some temperate countries with non-distinct influenza seasonality and some tropical/subtropical countries with distinct influenza seasonality. Five limitations of this study need to be acknowledged. First, there was sampling bias due to overall bias of case data being reported between different countries. Second, the time periods for all selected countries were not consistent, although they were all within the range of 2010 to 2017. It would benefit the influenza surveillance a lot if some countries with data covering a short period of time (e.g., Mauritius) had more resources injection. Third, the country-level data restricted us to explore the socioecological drivers of influenza seasonality. Fourth, different subtypes of influenza A have different and complex transmission routes, and the results of this study only present a global figure on all influenza A subtypes. Fifth, there were large amount of missing data on the subtypes of influenza A in the FluNet data, which restricted us to distinguish and study the patterns of different influenza viruses.
Conclusions
Influenza control and prevention attention can predominantly be paid to influenza A in countries such as Venezuela. Sub-Saharan Africa needs more influenza control resources, and efficient influenza prevention programs in Asia-Pacific region call for state-of-the-art internet-based influenza early warning system incorporating traditional surveillance data. Future attempts using spatiotemporal approaches to explore the drivers (e.g., socio-ecological factors) behind the influenza seasonality of tropical and subtropical countries are warranted.
Availability of data and materials
The data used in this study are publicly available data, and can be accessed from WHO FluNet (https://www.who.int/influenza/gisrs_laboratory/flunet/en/).
Abbreviations
- PA :
-
The proportion of influenza A virus in total influenza positive virus;
- RA :
-
The average positive rate of influenza A
- RB :
-
The average positive rate of influenza B
- RWA :
-
Weekly positive rate of influenza A
- RWB :
-
Weekly positive rate of influenza B
References
Iuliano AD, Roguski KM, Chang HH, Muscatello DJ, Palekar R, Tempia S, et al. Estimates of global seasonal influenza-associated respiratory mortality: a modelling study. Lancet. 2017;391(10127):1285–300.
Australian Government Department of Health: 2017 influenza season in Australia: A summary from the National Influenza Surveillance Committee. 2017.
Castilla J, Martínez-Baz I, Martínez-Artola V, Reina G, Pozo F, García Cenoz M, et al. Decline in influenza vaccine effectiveness with time after vaccination, Navarre, Spain, season 2011/12. Eurosurveillance. 2013;18(5):20388.
Caini S, Andrade W, Badur S, Balmaseda A, Barakat A, Bella A, et al. Temporal patterns of influenza a and B in tropical and temperate countries: what are the lessons for influenza vaccination? PLoS One. 2016;11(3):e0152310.
Tamerius J, Nelson MI, Zhou SZ, Viboud C, Miller MA, Alonso WJ. Global influenza seasonality: reconciling patterns across temperate and tropical regions. Environ Health Perspect. 2011;119(4):439–45.
Newman LP, Bhat N, Fleming JA, Neuzil KM. Global influenza seasonality to inform country-level vaccine programs: an analysis of WHO FluNet influenza surveillance data between 2011 and 2016. PLoS One. 2018;13(2):e0193263.
Hirve S, Newman LP, Paget J, Azziz-Baumgartner E, Fitzner J, Bhat N, et al. Influenza seasonality in the tropics and subtropics – when to vaccinate? PLoS One. 2016;11(4):e0153003.
He D, Lui R, Wang L, Tse CK, Yang L, Stone L. Global spatio-temporal patterns of influenza in the post-pandemic era. Sci Rep. 2015;5:11013.
Iha Y, Kinjo T, Parrott G, Higa F, Mori H, Fujita J. Comparative epidemiology of influenza A and B viral infection in a subtropical region: a 7-year surveillance in Okinawa, Japan. BMC Infect Dis. 2016;16:650.
Yu H, Alonso WJ, Feng L, Tan Y, Shu Y, Yang W, et al. Characterization of regional influenza seasonality patterns in China and implications for vaccination strategies: spatio-temporal modeling of surveillance data. PLoS Med. 2013;10(11):e1001552.
Saha S, Chadha M, Mamun AA, Rahman M, Sturm-Ramirez K, Chittaganpitch M, et al. Influenza seasonality and vaccination timing in tropical and subtropical areas of southern and South-Eastern Asia. Bull World Health Organ. 2014;92(5):318–30.
Lam TT, Tang JW, Lai FY, Zaraket H, Dbaibo G, Bialasiewicz S, et al. Comparative global epidemiology of influenza, respiratory syncytial and parainfluenza viruses, 2010–2015. J Inf Secur. 2019;79(4):373–82.
Tang JW, Lam TT, Zaraket H, Lipkin WI, Drews SJ, Hatchette TF, et al. Global epidemiology of non-influenza RNA respiratory viruses: data gaps and a growing need for surveillance. Lancet Infect Dis. 2017;17(10):e320–6.
Alonso WJ, Yu C, Viboud C, Richard SA, Schuck-Paim C, Simonsen L, et al. A global map of hemispheric influenza vaccine recommendations based on local patterns of viral circulation. Sci Rep. 2015;5:17214.
He D, Chiu APY, Lin Q, Yu D. Spatio-temporal patterns of proportions of influenza B cases. Sci Rep. 2017;7:40085.
Xu Z, Hu W, Zhang Y, Wang X, Tong S, Zhou M. Spatiotemporal pattern of bacillary dysentery in China from 1990 to 2009: what is the driver behind? PLoS One. 2014;9(8):e104329.
McAnerney JM, Cohen C, Moyes J, Besselaar TG, Buys A, Schoub BD, et al. Twenty-five years of outpatient influenza surveillance in South Africa, 1984–2008. J Infect Dis. 2012;206(suppl_1):S153–8.
Nyatanyi T, Nkunda R, Rukelibuga J, Palekar R, Muhimpundu MA, Kabeja A, et al. Influenza sentinel surveillance in Rwanda, 2008–2010. J Infect Dis. 2012;206(suppl_1):S74–9.
Theo A, Liwewe M, Ndumba I, Mupila Z, Tambatamba B, Mutemba C, et al. Influenza surveillance in Zambia, 2008–2009. J Infect Dis. 2012;206(suppl_1):S173–7.
Milinovich GJ, Williams GM, Clements ACA, Hu W. Internet-based surveillance systems for monitoring emerging infectious diseases. Lancet Infect Dis. 2014;14(2):160–8.
Liu K, Wang T, Yang Z, Huang X, Milinovich GJ, Lu Y, et al. Using Baidu search index to predict dengue outbreak in China. Sci Rep. 2016;6:38040.
Zhang Y, Milinovich G, Xu Z, Bambrick H, Mengersen K, Tong S, et al. Monitoring pertussis infections using internet search queries. Sci Rep. 2017;7(1):10437.
Cowling BJ, Caini S, Chotpitayasunondh T, Djauzi S, Gatchalian SR, Huang QS, et al. Influenza in the Asia-Pacific region: findings and recommendations from the global influenza initiative. Vaccine. 2017;35(6):856–64.
Deyle ER, Maher MC, Hernandez RD, Basu S, Sugihara G. Global environmental drivers of influenza. Proc Natl Acad Sci U S A. 2016;113(46):13081–6.
Acknowledgements
We’d like to thank World Health Organization for making the FluNet data publicly available. Dr. Wenbiao Hu was supported by an Australian Research Council Future Fellowship (award number FT140101216).
Funding
No funding.
Author information
Authors and Affiliations
Contributions
WH conceived the study. ZX and WH analyzed the data. ZX drafted the manuscript. WH, ZX and ZL interpreted the results and revised the manuscript. All authors read the approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Supplementary information
Additional file 1: Table S1.
Detailed information on influenza in the selected countries (listed by latitude).
Additional file 2: Figure S1.
Seasonality patterns of influenza A and influenza B in countries of temperate climate and of tropical or subtropical climate, from 2010 to 2017.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Xu, ZW., Li, ZJ. & Hu, WB. Global dynamic spatiotemporal pattern of seasonal influenza since 2009 influenza pandemic. Infect Dis Poverty 9, 2 (2020). https://doi.org/10.1186/s40249-019-0618-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40249-019-0618-5