
Abstract
Background
An increase in serum undercarboxylated osteocalcin concentrations suggests vitamin K deficiency. Clinical intervention studies suggested that the vitamin K supplementation might contribute to preventing bone loss in postmenopausal women. Evidence on the relationship between serum undercarboxylated osteocalcin (ucOC) levels and bone parameters of quantitative ultrasound (QUS) is limited. We examined the correlation between serum ucOC concentrations and bone status as measured by QUS among middle-aged and older Japanese men and women.
Methods
The subjects were community-dwelling men (n = 358) and women (n = 503) aged ≥ 40 years in Japan. Heel QUS parameters, including the stiffness index, speed of sound, and broadband ultrasound attenuation, were measured. Serum ucOC concentrations were measured by electrochemiluminescence immunoassay. Grip strength was measured in the dominant hand. Information on alcohol drinking, current smoking, exercise, and menopause in women was collected.
Results
Serum ucOC concentrations were significantly associated with age in both sexes. Serum ucOC concentrations in men were higher at ≥ 80 years than those in the age groups of 40–49, 50–59, and 60–69 years. Serum ucOC concentrations in women were higher in the age groups of 50–59 and 60–69 years than those at 40–49 years. Partial correlation analysis adjusting for covariates (age, body mass index, grip strength, alcohol drinking, current smoking, and exercise in men; age, body mass index, grip strength, alcohol drinking, current smoking, exercise, and menopause in women) showed that serum ucOC concentrations were negatively significantly correlated with all QUS parameters in women. Serum ucOC concentrations were not correlated with them in men.
Conclusions
Vitamin K deficiency, evaluated with higher serum ucOC, was correlated with poor bone status in women.
Similar content being viewed by others

Background
Osteoporosis and associated fragility bone fracture is a major health problem in the elderly. Osteoporosis was defined as a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase in bone fragility and susceptibility to fracture. Low bone mass is one of the reliable objective evaluations for osteoporosis and is reported to be associated with various factors, such as gender, age, several foods, and behavior in daily life. Among these factors vitamins were safe and thought to be effective targets for the prevention against osteoporosis.
Vitamin K is a liposoluble vitamin discovered in 1929, and its name derived from the German word koagulation. Clinical intervention studies suggested that the vitamin K supplementation might contribute to preventing bone loss in postmenopausal women [1, 2]. Vitamin K can be measured in plasma, but the values alone may not be sufficient to assess the biological vitamin K status because of its many isoforms and different bioavailability. Phylloquinone is an isoform found in human diet and is synthesized by plants and green vegetables. Menaquinones with several subtypes are another isoform of vitamin K in meat and are endogenously synthesized by intestinal bacteria. Food frequency questionnaires can assess the intake of vitamin K, but assessing the activity rather than intake seems clinically more appropriate. Objective measurement by quantifying undercarboxylation of osteocalcin seems to be sensitive for the activity of vitamin K.
Osteocalcin (OC) is a non-collagenous protein that is secreted by osteoblasts, and has three glutamic acid residues [3]. These residues in OC are γ-carboxylated in the presence of vitamin K, and OC becomes carboxylated osteocalcin (Gla-OC), which binds to calcium ions in hydroxyapatite (hydroxylated calcium phosphate). While Gla-OC deposits to bone, at an insufficient vitamin K dietary intake, OC does not undergo complete γ-carboxylation, and undercarboxylated osteocalcin (ucOC) is released [4]. Because ucOC is not taken in by the bone matrix and is released in the blood, an increase in blood ucOC concentrations indicates a lack of vitamin K and a decrease in Gla-OC [4].
Low vitamin K intake is associated with an increased risk of hip fractures [5, 6]. Vergnaud et al. [7] showed that serum ucOC concentrations predict the risk of hip fracture independent of femoral neck bone mineral density (BMD) in older women. Bullo et al. [8] showed that vitamin K intake is associated with a higher BMD in men and women, but Booth et al. [9] showed an association only in women, not in men. Some studies have shown that elevated serum ucOC concentrations are associated with a low BMD in women [10, 11], but other studies did not show this association [12, 13].
Quantitative ultrasound (QUS) provides information that is more useful than just density for estimating bone strength [14]. QUS is even a promising alternative to dual energy X-ray absorptiometry for estimating BMD [15, 16]. Liu et al. [12] showed that serum ucOC concentrations were negatively correlated with QUS parameters in older women. Recently, Suzuki et al. [17] showed a correlation between serum ucOC concentrations and QUS parameters, such as the speed of sound (SOS), in female college students. Therefore, evidence on the relationship between serum ucOC concentrations and QUS parameters is limited in women. Furthermore, to the best of our knowledge, there have been no reports on correlations between serum ucOC concentrations and QUS parameters in men. We examined the correlations between serum ucOC concentrations, as an objective indicator for the vitamin K status, and bone status as measured by QUS in middle-aged and older Japanese men and women.
Methods
The subjects were community-dwelling men and women aged 40 years and older in Unzen City, Nagasaki Prefecture, Japan. The population aged 40 years and older in this City was approximately 13,000. Subjects were recruited from men and women who participated in periodic health examinations in 2011–2013. A total of 441 men (mean [SD] age 66.1 [9.9], range 40–92 years) and 637 women (mean [SD] age 66.0 [9.2], range 40–89 years) participated in this study. All subjects provided written, informed consent before examinations. This study was approved by the Ethics Committee of Nagasaki University Graduate School of Biomedical Sciences.
Heel QUS parameters, including the stiffness index, SOS, and broadband ultrasound attenuation (BUA), were measured using a Lunar Achilles device (GE Lunar Corp., Madison, WI). Spot blood samples were collected. Serum ucOC concentrations were measured by electrochemiluminescence immunoassay. Height (cm) and weight (kg) were measured with light clothing and without shoes, and the body mass index (BMI) was calculated as weight/height squared (kg/m2). Grip strength was measured using a hydraulic hand dynamometer (Jamar hydraulic hand dynamometer 5030 J1; Jafayette Instrument Company, Inc., Jafayette, IN). The average performance from two trials using the participants’ dominant hand was used as the result for analysis. Since lifestyle is important to physical and health status [18,19,20], information on alcohol drinking (≥ 40 g/day in men, ≥ 20 g/day in women), current smoking (yes/no), exercise (at least 30 min twice per week), and menopause (yes/no only in women) was collected by interview.
Subjects with missing values for any variables were excluded from the analysis, with a total of 358 men and 503 women for the final data analysis. The Student t test or the chi-square test was used to examine the differences in variables between sexes. One-way ANOVA was used to compare serum ucOC concentrations among 10-year age groups. As ucOC and QUS parameters were out of normal distribution, Pearson’s product-moment correlations and partial correlations adjusting for age, BMI, grip strength, alcohol drinking, current smoking, exercise, and menopause (for women) were calculated to assess correlations between serum ucOC concentrations and QUS parameters [20,21,22,23]. A p value of less than 0.05 was considered significant. The data were analyzed using the Statistical Analysis System software package version 9.4 (SAS Institute, Cary, NC).
Results
Table 1 shows the characteristics of the subjects. QUS parameters (stiffness index, SOS, and BUA) were higher in men than those in women (p < 0.001 for these). Serum ucOC concentrations in women were higher than those in men (p < 0.001).
Table 2 shows the mean (SD) of QUS parameters by age groups. QUS parameters significantly decreased with age in both sexes (p < 0.001).
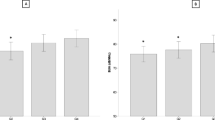
Table 3 shows the mean (SD) of serum ucOC concentrations by age groups. Serum ucOC concentrations significantly increased with age in men and women (p = 0.018 and p = 0.016, respectively). Serum ucOC concentrations in men were higher in the age group of 80 years and older compared with those in the age groups of 40–49, 50–59, and 60–69 years. Serum ucOC concentrations in women were higher in the age groups of 50–59 and 60–69 years than those in the age group of 40–49 years.
Table 4 shows simple and partial correlation coefficients between serum ucOC concentrations and the stiffness index, SOS, and BUA. Simple correlation analysis showed that serum ucOC concentrations were negatively correlated with all QUS parameters in women (p = 0.013, 0.044, and 0.015, respectively) and with the stiffness index and SOS in men (p = 0.031 and 0.030). Partial correlation analysis adjusted for covariates (age, BMI, grip strength, alcohol drinking, current smoking, and exercise in men; age, BMI, grip strength, alcohol drinking, current smoking, exercise, and menopause in women) showed that serum ucOC concentrations were negatively significantly correlated with all QUS parameters in women (p = 0.019, 0.034, and 0.045, respectively). Serum ucOC concentrations were not correlated with the stiffness index, SOS, or BUA in men (p = 0.229, 0.149, and 0.421, respectively).
Discussion
We showed that after adjusting for covariates, serum ucOC concentrations were negatively significantly correlated with the stiffness index, SOS, and BUA only in women. To the best of our knowledge, this is the first study to examine the correlation between serum ucOC concentrations and QUS parameters in men, in whom no correlations were found.
In the present study, serum ucOC concentrations significantly were associated with age in both sexes. Serum ucOC concentrations were higher after 50 years old in women. Previous studies showed that serum ucOC concentrations decreased with age in men [24, 25] and increased postmenopausally in women [10, 24,25,26]. These findings are consistent with our findings in women, but not in men. Because vitamin K is the main factor determining the state of carboxylation of OC, an increase in serum ucOC concentrations suggests vitamin K deficiency. There may be variations in vitamin K intake among individuals, which could in part contribute to the inconsistent results in men.
There were significant differences in bone mass between men and women. Also there was gender difference in the concentration of ucOC in community-dwelling subjects living in the same city. Some factors may be associated with the gender difference in activity of vitamin K about bone health, such as the differences in the amount of bone mass, amount of sex hormones, prevalence of drinking and smoking, and postmenopausal hormonal change. Further study is necessary to assess the mechanism of gender difference in the function of vitamin K.
QUS measurements reflect qualitative properties [27], considering that BUA is mainly affected by structural characteristics of trabecular bone, such as porosity [8, 28], and that SOS is an indicator of the elastic properties of bone [29]. Our results suggest that elevated serum ucOC concentrations (vitamin K deficiency) contribute to increased porosity and decreased elasticity.
The intake of environmental resource as a food, including several kinds of vitamins, is one of the physiological adaptations because human cannot synthesize any vitamins in their own cells. It is well established that the deficiency of vitamin K leads to health problems of blood clotting. Not only in the pathological status, but also in physiological status of community-dwelling subjects, vitamin K may play a role for bone health. Further study may discover the different physiological adaptation in absorbance, bioavailability or response to vitamins, which may contribute to adapt to the poor environmental resource.
Vitamin K deficiency is associated with hip or vertebral fractures [5,6,7, 30]. Liu et al. [12] showed that serum ucOC concentrations were more strongly correlated with calcaneal QUS parameters (e.g., ultrasonic transmitted velocity) than femoral neck BMD. This finding suggests that ucOC content of bone may adversely affect bone strength, with more effect on bone quality than on BMD. Vitamin K deficiency may adversely affect bone quality more than bone mass.
This study has several limitations. First, because the study was cross-sectional in nature, proving causal relationships between ucOC concentrations and QUS parameters was difficult. A longitudinal study is required to determine this causality. Second, because BMD measurements were not available in this study, we could not assess the degree of bone quality (QUS) and mass (BMD). Third, because we could not assess nutritional status, dietary vitamin K levels were unknown. Forth, because we showed an association between ucOC and QUS parameter adjustment for gender, age, body mass index, grip strength, alcohol drinking, current smoking, exercise, and menopause, we could not assess other possible factors influencing bone health, including nutrition and occupations. Fifth, because our subjects were all Japanese who voluntarily participated in periodic health examinations, our results have to be interpreted with caution as the selection bias.
Conclusion
Vitamin K deficiency, evaluated with higher serum ucOC, was correlated with poor bone status in women, but not in men.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- BMD:
-
Bone mineral density
- BUA:
-
Broadband ultrasound attenuation
- OC:
-
Osteocalcin
- QUS:
-
Quantitative ultrasound
- SOS:
-
Speed of sound
- ucOC:
-
Undercarboxylated osteocalcin
References
Knapen MH, Schurgers LJ, Vermeer C. Vitamin K2 supplementation improves hip bone geometry and bone strength indices in postmenopausal women. Osteoporos Int. 2007;18:963–72 PMID: 17287908.
Braam LA, Knapen MH, Geusens P, Brouns F, Hamulyák K, Gerichhausen MJ, Vermeer C. Vitamin K1 supplementation retards bone loss in postmenopausal women between 50 and 60 years of age. Calcif Tissue Int. 2003;73:21–6 PMID: 14506950.
Price PA, Williamson MK, Lothringer JW. Origin of the vitamin K-dependent bone protein found in plasma and its clearance by kidney and bone. J Biol Chem. 1981;256:12760–6.
Sokoll LJ, Sadowski JA. Comparison of biochemical indexes for assessing vitamin K nutritional status in a healthy adult population. Am J Clin Nutr. 1996;63:566–73.
Booth SL, Tucker KL, Chen H, Hannan MT, Gagnon DR, Cupples LA, Wilson PW, Ordovas J, Schaefer EJ, Dawson-Hughes B, Kiel DP. Dietary vitamin K intakes are associated with hip fracture but not with bone mineral density in elderly men and women. Am J Clin Nutr. 2000;71:1201–8.
Feskanich D, Weber P, Willett WC, Rockett H, Booth SL, Colditz GA. Vitamin K intake and hip fractures in women: a prospective study. Am J Clin Nutr. 1999;69:74–9.
Vergnaud P, Garnero P, Meunier PJ, Breart G, Kamihagi K, Delmas PD. Undercarboxylated osteocalcin measured with a specific immunoassay predicts hip fracture in elderly women: the EPIDOS Study. J Clin Endocrinol Metab. 1997;82:719–24.
Bullo M, Estruch R, Salas-Salvado J. Dietary vitamin K intake is associated with bone quantitative ultrasound measurements but not with bone peripheral biochemical markers in elderly men and women. Bone. 2011;48:1313–8.
Booth SL, Broe KE, Gagnon DR, Tucker KL, Hannan MT, McLean RR, Dawson-Hughes B, Wilson PW, Cupples LA, Kiel DP. Vitamin K intake and bone mineral density in women and men. Am J Clin Nutr. 2003;77:512–6.
Kim SM, Kim KM, Kim BT, Joo NS, Kim KN, Lee DJ. Correlation of undercarboxylated osteocalcin (ucOC) concentration and bone density with age in healthy Korean women. J Korean Med Sci. 2010;25:1171–5.
Szulc P, Arlot M, Chapuy MC, Duboeuf F, Meunier PJ, Delmas PD. Serum undercarboxylated osteocalcin correlates with hip bone mineral density in elderly women. J Bone Miner Res. 1994;9:1591–5.
Liu G, Peacock M. Age-related changes in serum undercarboxylated osteocalcin and its relationships with bone density, bone quality, and hip fracture. Calcif Tissue Int. 1998;62:286–9.
Yamauchi M, Yamaguchi T, Nawata K, Takaoka S, Sugimoto T. Relationships between undercarboxylated osteocalcin and vitamin K intakes, bone turnover, and bone mineral density in healthy women. Clin Nutr. 2010;29:761–5.
Krieg MA, Barkmann R, Gonnelli S, Stewart A, Bauer DC, Del Rio Barquero L, Kaufman JJ, Lorenc R, Miller PD, Olszynski WP, Poiana C, Schott AM, Lewiecki EM, Hans D. Quantitative ultrasound in the management of osteoporosis: the 2007 ISCD Official Positions. J Clin Densitom 2008, 11:163-187.
Laugier P. Quantitative ultrasound of bone: looking ahead. Joint Bone Spine. 2006;73:125–8.
Moris M, Peretz A, Tjeka R, Negaban N, Wouters M, Bergmann P. Quantitative ultrasound bone measurements: normal values and comparison with bone mineral density by dual X-ray absorptiometry. Calcif Tissue Int. 1995;57:6–10.
Suzuki Y, Maruyama-Nagao A, Sakuraba K, Kawai S. Level of serum undercarboxylated osteocalcin correlates with bone quality assessed by calcaneal quantitative ultrasound sonometry in young Japanese females. Exp Ther Med. 2017;13:1937–43.
Tuggle AC, Cohen JH, Crews DE. Stress, migration, and allostatic load: a model based on Mexican migrants in Columbus. Ohio. J Physiol Anthropol. 2018;37:28.
Logan AC, Prescott SL, Haahtela T, Katz DL. The importance of the exposome and allostatic load in the planetary health paradigm. J Physiol Anthropol. 2018;37:15.
Neglia C, Argentiero A, Chitano G, Agnello N, Ciccarese R, Vigilanza A, Pantile V, Argentiero D, Quarta R, Rivezzi M, Di Tanna GL, Di Somma C, Migliore A, Iolascon G, Gimigliano F, Distante A, Piscitelli P. Diabetes and obesity as independent risk factors for osteoporosis: updated results from the ROIS/EMEROS registry in a population of five thousand post-menopausal women living in a region characterized by heavy environmental pressure. Int J Environ Res Public Health. 2016;13:1067.
Abe Y, Nishimura T, Arima K, Kanagae M, Mizukami S, Tomita Y, Okabe T, Goto H, Horiguchi I, Aoyagi K. Effect of self-reported walking difficulty on bone mass and bone resorption marker in Japanese people aged 40 years and over. J Physiol Anthropol. 2016;35:25.
Hasegawa J, Suzuki H, Yamauchi T. Impact of season on the association between muscle strength/volume and physical activity among community-dwelling elderly people living in snowy-cold regions. J Physiol Anthropol. 2018;37:25.
McCloskey EV, Kanis JA, Oden A, Harvey NC, Bauer D, Gonzalez-Macias J, Hans D, Kaptoge S, Krieg MA, Kwok T, Marin F, Moayyeri A, Orwoll E, Glusmall io RC, Johansson H. Predictive ability of heel quantitative ultrasound for incident fractures: an individual-level meta-analysis. Osteoporos Int 2015, 26:1979-1987.
Furusyo N, Ihara T, Hayashi T, Ikezaki H, Toyoda K, Ogawa E, Okada K, Kainuma M, Murata M, Hayashi J. The serum undercarboxylated osteocalcin level and the diet of a Japanese population: results from the Kyushu and Okinawa Population Study (KOPS). Endocrine. 2013;43:635–42.
Nimptsch K, Hailer S, Rohrmann S, Gedrich K, Wolfram G, Linseisen J. Determinants and correlates of serum undercarboxylated osteocalcin. Ann Nutr Metab. 2007;51:563–70.
Tsugawa N, Shiraki M, Suhara Y, Kamao M, Tanaka K, Okano T. Vitamin K status of healthy Japanese women: age-related vitamin K requirement for gamma-carboxylation of osteocalcin. Am J Clin Nutr. 2006;83:380–6.
Njeh CF, Fuerst T, Diessel E, Genant HK. Is quantitative ultrasound dependent on bone structure? A reflection. Osteoporos Int. 2001;12:1–15.
Gluer CC, Wu CY, Jergas M, Goldstein SA, Genant HK. Three quantitative ultrasound parameters reflect bone structure. Calcif Tissue Int. 1994;55:46–52.
De Terlizzi F, Battista S, Cavani F, Cane V, Cadossi R. Influence of bone tissue density and elasticity on ultrasound propagation: an in vitro study. J Bone Miner Res. 2000;15:2458–66.
Tsugawa N, Shiraki M, Suhara Y, Kamao M, Ozaki R, Tanaka K, Okano T. Low plasma phylloquinone concentration is associated with high incidence of vertebral fracture in Japanese women. J Bone Miner Metab. 2008;26:79–85.
Funding
This work was supported by JSPS KAKENHI Grant Number JP23370105.
Author information
Authors and Affiliations
Contributions
KA designed the study and prepared the first draft of the paper. NT, KA, TN, YT, SM, TO, YA, SK, RT, and KA contributed to the acquisition, analysis, and interpretation of the data. NT, KA, TN, MU, YH, MK, MO, and KA were responsible for statistical analysis of the data and participated in the discussion and preparation of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Nagasaki University Graduate School of Biomedical Sciences. All participants provided written informed consent before examinations. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent for publication
Informed consent was obtained from all individual participants included in the study.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tanaka, N., Arima, K., Nishimura, T. et al. Vitamin K deficiency, evaluated with higher serum ucOC, was correlated with poor bone status in women. J Physiol Anthropol 39, 9 (2020). https://doi.org/10.1186/s40101-020-00221-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40101-020-00221-1