
Abstract
Objective
To develop a new score system for patients with prostate specific antigen (PSA) ranging from 4 to 20 ng/mL to improve the accuracy of prostate cancer (PCa) detection, and to evaluate it with receiver operating characteristic curve.
Methods
A total of 797 patients (208 with prostate cancer) with total PSA 4–20 ng/mL who had undergone transrectal ultrasound (TRUS)-guided 12 + 1-core prostate biopsy during Sept. 2009–Jan. 2013 were retrospectively evaluated in the study. Age, PSA, fPSA, PV, f/T, PSAD, DRE findings and ultrasound findings were considered as predictive factors and tested by logistic regression. Predictors with P < 0.05 were selected to develop a new score system.
Results
Age, PSA, PV, f/T, DRE findings, and hypoechoic in ultrasound were selected in our new score system. The risk of PCa increased with the score. From 0 to 6, the risk was 2.0, 8.4, 13.9, 33.5, 63.8, 75.0 and 100.0 % respectively. Area under curve (AUC) of our new score system was 0.804, which was significantly higher than The Prostate Cancer Risk Calculator by Stichting Wetenschappelijk Onderzoek Prostaatkanker (SWOP) (0.720, P = 0.002).
Conclusions
We developed a new simple score system for patients with PSA ranging from 4 to 20 ng/mL to improve the accuracy of PCa detection.
Similar content being viewed by others


Background
Prostate specific antigen (PSA) is widely used for the screening of prostate cancer in recent years. However, an increasing level of PSA can also represent the occurrence of benign prostate hyperplasia (BPH) and prostatitis, which questioned the specificity of PSA in predicting prostate cancer (Catalona et al. 1995). Although the region of PSA levels from 4 to 10 ng/mL is defined as a “gray zone” according to the traditional concepts, the prostate cancer detection rate of the patients with PSA levels of 10–20 ng/mL is not superior to the patients whose PSA levels in the “gray zone” conspicuously. The incidence rate was 25 % or less in the region of PSA from 4 to 20 ng/mL (Tang et al. 2013; Chavan et al. 2009). The rate of the patients with the PSA level in range of 4–20 ng/mL in the initial examination in clinic has been increase since the examination of PSA level was a routine physical examination. Clearly, there is an urgent need to develop a new system for improving the detection rate and reducing unnecessary prostate biopsies in the region of PSA levels from 4 to 20 ng/mL.
Methods
Ethics statement
This study was approved by the institutional review board of the First Affiliated Hospital of Nanjing Medical University. Written informed consent was obtained from all patients with regard to the storage of their information for the purpose of research. All research procedures were conducted in accordance with the Declaration of Helsinki.
Characteristics and methods
Our study included 797 patients, who had an elevated PSA level ranging from 4 to 20 ng/mL and had undergone a transrectal ultrasound (TRUS)-guided prostate biopsy from September 2009 to January 2013 at the First Affiliated Hospital of Nanjing Medical University, China. All the patients envolved in our study are Chinese men. Detail patient information, including age, PSA, free PSA (fPSA), digital rectal examination (DRE) findings and other clinical information were recorded before prostate biopsy. The information of patients’ PSA levels were provided by laboratory of the First Affiliated Hospital of Nanjing Medical University, they used a single validated assay to assess PSA levels. An ellipsoid formula (PI/6 × lateral × anteroposterior × superoinferior diameters) was used to calculate the prostate volume (PV) of every patient in this study by means of ultrasonoscopy, and detailed observation were carried out regarding microcalcifications and hypoechoic lesions. PSA density (PSAD) was defined as the ratio of PSA to PV. The free/total PSA ratio (f/T) was calculated by dividing the level of fPSA present by the total level of PSA.
We used Philips Envisor C Ultrasound Machine to localized the position and used Bard Maxcore Disposable Biopsy Instrument MC1820 to collected the tissue of prostate. The TRUS-guided prostate biopsy from September 2009 to January 2013 were performed by experienced urologists in the First Affiliated Hospital of Nanjing Medical University. Routine examination including blood, liver and kidney function and coagulation was taken by the patients before the prostate biopsy.
Statistical analysis
Statistical analysis was performed using SPSS 18.0 software. Differences between data of the patients were analyzed using the t test for continuous variables and the Chi square test for categorical variables. We used multiple logistic regression analysis with a backward elimination selection procedure to select potential predictors. One score was given when the positive factors more than the median score. 100 patients from a total of 797 patients with total PSA 4–20 ng/mL who had undergone TRUS-guided 12 + 1-core prostate biopsy during Sept. 2009–Jan. 2013 the First Affiliated Hospital of Nanjing Medical University were randomly selected with random number table for assessment of effectiveness of the new score system and The Prostate Cancer Risk Calculator by Stichting Wetenschappelijk Onderzoek Prostaatkanker (SWOP), which is an initiative of the Department of Urology of the Erasmus MC, the University and Medical Centre of Rotterdam, in The Netherlands. Erasmus MC is one of eight European centers taking part in the world’s largest study of screening for prostate cancer, the European Randomized Study of Screening for Prostate Cancer (ERSPC). We used a receiver-operating characteristic (ROC) curve to assess the effectiveness of the new score system and The Prostate Cancer Risk Calculator by SWOP Finally, Z-test was used to compare the difference of the area under the curve. We considered statistical significant when P value <0.05.
Results
In this study, 208 (27 %) of 797 patients had positive biopsy results. The characteristic details of the patients in the study cohort are indicated in Table 1. The mean ages of patients in the PCa group and the non-PCa group were 70.6 ± 6.8 and 66.9 ± 8.7 years; P < 0.01. Moreover, other statistical differences including PSA (P < 0.001), fPSA (P < 0.001), PSAD (P < 0.001), f/TPSA (P < 0.001) DRE findings (P < 0.001) and hypoechoic under transrectal ultrasound findings (P < 0.001) were found between the PCa group and non-PCa group. However, there is no significant statistical difference in microcalcifications (P = 0.262). Univariate analysis indicated that age, PSA, fPSA, f/T, PV, PSAD, abnormal DRE and the rate of ultrasonic hypoechoic mass in patients with a positive initial prostate biopsy were different from patients with an initial negative biopsy. Age, PSA, fPSA, t/T, PV, PSAD, DRE findings and ultrasonic hypoechoic mass were included in logistic analysis on multivariate analysis. The categorical variables were valuated before analysis. We valuated abnormal and no significant abnormal DRE findings as 1 and 0 score; valuated hypo echoic mass and no significant hypoechoic mass in TURS as 1 and 0 score; valuated positive and negative prostate biopsy finding as 1 and 0 score. All the other independent variable were included in the logistic analysis as continuous variables. After a backward elimination selection procedure, six predictors indicated significant differences (Age, PSA, t/T, PV, DRE findings and ultrasonic hypoechoic mass in TURS) suggested that these parameters were potential predictors for initial prostate biopsy (Table 2). According to the result of the logistic analysis, the new system model was created including the significantly potential predictors such as age, PSA, f/T, PV, DRE findings and hypo echoic mass in TURS. The section point was defined as the overall median of the predictors. Positive factors such as age > 69, PSA > 9.3 was valuated as 1 score; while negative factors such as PV < 37.1, f/T < 0.14 was valuated 1 score. Additionally, abnormal DRE findings and hypo echoic mass in TURS was also valuated as 1 score. The positive rate of new score system is shown in Table 3.
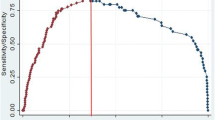
Receiver operating characteristic (ROC) was used to evaluated the accuracy of PCa detection in the new score system (Fig. 1). A notable rise of the area under the curve (AUC) of the ROC for the new score system (0.804) was observed by using the Z-test in this study when compared with The Prostate Cancer Risk Calculator by SWOP (0.72, P = 0.002).

ROC of our new score system and SWOP. The AUC of these predictors were 0.804 and 0.720
Discussion
PSA is a conventional clinical screening parameter. However, the increase of PSA can also been observed in various situation such as benign prostatic hypertrophy (BPH), inflammation and prostate cancer (Littrup et al. 1994). Screening of PSA was also questioned by some scholars because although it increase the detection rate, the mortality is still not reduce and also bring the problem of overdiagnosis and overtreatment (Peres 2013). The number of patients with PSA level ranging from 4 to 20 ng/mL in the initial clinic examination is increasing since the PSA level was been an event of the routine examination in some medical center, China. A large amount of unnecessary prostate biopsy will be performed if we still insist on PSA > 4 as the biopsy indication (Wolf et al. 2010). Considering of the low specificity of the screening of PSA, some other upgraded predictors such as PSAD, f/T and The Prostate Cancer Risk Calculator by SWOP were introduced. However, most of these parameters have involved from PSA, therefore making them provincial (Vickers et al. 2009).
Previous research has shown that predictive models which based on clinical laboratory and ultrasound parameters, DRE findings can improve the accuracy of prostate cancer detection to a various degrees (Carlson et al. 1998; Eastham et al. 1999; Potter et al. 2001). Unfortunately, score systems based other races usually unsuitable for Chinese men. Furthermore, it is hard to use the score model in clinic because it remains controversial (Park et al. 2011). Thus, it is obvious that particularly designed for the patients with PSA level ranging from 4 to 20 ng/mL can gain further insights. In this study we develop a new score system to improve the accuracy of prostate cancer in PSA from 4 to 20 ng/mL.
10–14 cores biopsy has gained widespread acceptance in the initial examination (Scattoni et al. 2007; Ukimura et al. 2013). We used 12 + 1 cores biopsy with ultrasound and got high accuracy of PCa detection, which guarantee the dependability of our new score system.
The positive rate of patients had positive biopsy results in this study was more than 50 % when score >3, which means patients with 0 and 1 score had a low positive rate of biopsy (<10 %). Encourage patients with 0 and 1 score to receive prostate biopsy may lead to overdiagnosis and overtreatment.
ROC curve is widely used to evaluate clinic diagnosis index. AUC shows a positive correlation with the value of diagnosis index. AUC of our new score system was 0.790, which was significantly higher than The Prostate Cancer Risk Calculator by SWOP (0.720, P = 0.002) (Fig. 1). The accuracy of PCa detection of the new score system is significantly higher than single parameter.
Prostate biopsy belongs to invasive examination and has some risks including bleeding and infection. PCa is a common malignant disease in elderly people, who are also suffering from the threaten of some chronic disease such as hypertension, diabetes and coronary artery disease. Previous studies have demonstrated that the accuracy of PCa detection of patients with PSA level ranging from 4 to 20 ng/mL is low. Thus, elderly patients should undergo biopsies depended on their physical conditions. A new score system was developed based on our study. According to the system, patients with 0–1 score should closely monitored for PSA; patients with 2 score should consider to biopsy according to physical examinations; patients with score ≥3 should undergo biopsy actively. The other advantage of the new score system is that predictors such as PSA, PV, age, DRE finding, hypoechoic mass and f/T are routine clinical examination events. It is convenient to use new score system on outpatients instead of complex formulas.
Conclusions
In conclusion, we developed a new score system to improve the accuracy of prostate cancer detection in PSA 4–20 ng/mL. A reasonable prostate biopsy strategy based on the new score system was demonstrated to reduce the unnecessary prostate biopsies and increase the detection rate of PCa.
References
Carlson GD, Calvanese CB, Partin AW (1998) An algorithm combining age, total prostate-specific antigen (PSA), and percent free PSA to predict prostate cancer: results on 4298 cases. Urology 52(3):455–461
Catalona WJ, Smith DS, Wolfert RL (1995) Evaluation of percentage of free serum prostate-specific antigen to improve specificity of prostate cancer screening. JAMA 274(15):1214–1220
Chavan PR, Chavan SV, Chavan NR (2009) Detection rate of prostate cancer using prostate specific antigen in patients presenting with lower urinary tract symptoms: a retrospective study. J Postgrad Med 55:17–21
Eastham JA, May R, Robertson JL (1999) Development of a nomogram that predicts the probability of a positive prostate biopsy in men with an abnormal digital rectal examination and a prostate-specific antigen between 0 and 4 ng/mL. Urology 54(4):709–713
Littrup PJ, Goodman AC, Mettlin CJ (1994) Cost analyses of prostate cancer screening: frameworks for discussion. Investigators of the American Cancer Society-National Prostate Cancer Detection project. J Urol 152(5 Pt 2):1873–1877
Park JY, Yoon S, Park MS (2011) Initial biopsy outcome prediction in Korean patients-comparison of a noble web-based Korean prostate cancer risk calculator versus prostate-specific antigen testing. J Korean Med Sci 26(1):85–91
Peres J (2013) Risks of PSA screening now better understood. J Natl Cancer Inst 105(21):1590–1592
Potter SR, Horniger W, Tinzl M (2001) Prostate-specific antigen, and digital rectal examination as determinants of the probability of having prostate cancer. Urology 57(6):1100–1104
Scattoni V, Zlotta A, Montironi R (2007) Extended and saturation prostatic biopsy in the diagnosis and characterisation of prostate cancer: a critical analysis of the literature. Eur Urol 52:1309–1322
Tang P, Du W, Xie K (2013) Transition zone PSA density improves the prostate cancer detection rate both in PSA 4.0–10.0 and 10.1–20.0 ng/ml in Chinese men. Urol Oncol 31(6):744–748
Ukimura O, Coleman JA, De La Taille A (2013) Contemporary role of systematic prostate biopsies: indications, techniques, and implications for patient care. Eur Urol 63:214–230
Vickers AJ, Savage C, O’brien MF (2009) Systematic review of pretreatment prostate-specific antigen velocity and doubling time as predictors for prostate cancer. J Clin Oncol 27(3):398–403
Wolf AM, Wender RC, Etzioni RB (2010) American Cancer Society Prostate Cancer Advisory Committee. American Cancer Society guideline for the early detection of prostate cancer: update 2010. CA Cancer J Clin 60(2):70–98
Authors’ contributions
ZY carried out data analysis, drafting and revision of the final manuscript, HY prepared the data collection and manuscript for submission, CG coordinated efforts of the critical revision of the manuscript, ZC and WJ provided assistance with statistical analysis and critical revision of the manuscript, QC provided assistance with statistical analysis and critical revision of the manuscript, HL participated in the data collection and performed final data check, WZ were involved with study conception, supervision and critical revision of the manuscript. All authors have read and approved the final manuscript.
Acknowledgements
We would like to acknowledge the help of the Department of Urology, the First Affiliated Hospital of Nanjing Medical University. There are no conflicts of interest or financial to declare.
Competing interests
The authors declare that they have no competing interests.
Animal rights
This article does not contain any studies with animals performed by any of the authors.
Ethical standard
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
This study was funded by the Priority Academic Program Development of Jiangsu Higher Education Institution (PAPD) (Grant Number JX10231801).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Zheng, Y., Huang, Y., Cheng, G. et al. Developing a new score system for patients with PSA ranging from 4 to 20 ng/mL to improve the accuracy of PCa detection. SpringerPlus 5, 1484 (2016). https://doi.org/10.1186/s40064-016-3176-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40064-016-3176-3