
Abstract
Background
COVID-19 is an infectious disease currently spreading worldwide. The COVID-19 virus requires angiotensin-converting enzyme 2, an enzyme that plays a vital role in regulating the apelinergic system for entry into target cells. The underlying diseases of hypertension, diabetes mellitus, and obesity are risk factors for the severity of COVID-19 infection. This study aimed to compare the serum levels of apelin and nitric oxide in hospitalized COVID-19 patients and non-COVID-19 subjects with and without the mentioned risk factors.
Methods
Serum samples were taken from 69 COVID-19 patients and 71-matched non-COVID-19 participants enrolled in the Kerman coronary artery disease risk factors cohort study. Study participants were divided into eight groups of control (healthy), hypertension, diabetes mellitus, obesity, COVID-19, COVID-19 + hypertension, COVID-19 + diabetes mellitus, and COVID-19 + obesity (n = 15–20 in each group). Serum apelin and nitrite were measured by the enzyme-linked immunosorbent assay and colorimetric methods, respectively.
Results
Hypertensive and obese patients had lower serum apelin compared to the control group. In addition, apelin content was lower in the COVID-19 and COVID-19 + diabetes mellitus groups compared to the non-COVID-19 counterpart groups. Serum apelin levels were positively associated with arterial O2sat. and negatively with the severity of lung involvement. Nitric oxide metabolites were significantly lower in the COVID-19, COVID-19 + diabetes mellitus, and COVID-19 + obesity groups.
Conclusions
The lower apelin and nitric oxide levels in patients with hypertension and obesity or their reduction due to infection with COVID-19 or concomitant COVID-19 + diabetes mellitus may make them vulnerable to experiencing severe diseases.
Similar content being viewed by others


Introduction
The COVID-19 infection caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was originally reported as an epidemic in Wuhan, China, in December 2019 [1]. This infection has spread worldwide and, according to the World Health Organization (WHO), is a health challenge sparking international alarm [2]. People with risk factors such as hypertension, diabetes mellitus, obesity, and other cardiovascular diseases (CVDs) risk factors, and those older than 55 years are at greater risk [3, 4]. As a result, taking care of the elderly and those with underlying CVDs is a higher priority, as more severely ill patients will impose higher expenses on the country’s healthcare system [5].
For entry into its target cells, the SARS-CoV-2 binds to the angiotensin-converting enzyme type 2 (ACE2) through glycoprotein spikes. ACE2, a member of the renin–angiotensin–aldosterone system (RAAS), is responsible for inactivating angiotensin I and II and producing angiotensin 1–7 [6].
Apelin originated from a 77-amino acid pre-propeptide with several functional isoforms, including apelin-36, apelin-17, apelin-13, and (Pyr1) apelin-13, which is a post-translationally modified isoform in the circulation [7]. Apelin and ACE2 have a bilateral relationship. ACE2 degrades the apelin peptides to inactive forms, while apelin increases ACE2 expression [8]. Apelin and its receptor (APLNR, also known as APJ) are expressed in many tissues, such as the heart, lung, and blood vessels, regulating the cardiovascular and respiratory systems [9,10,11]. Apelin reduces arterial blood pressure by increasing nitric oxide (NO) generation and enhancing heart contractility. This peptide also protects the heart against ischemic–reperfusion injuries [11] and has antithrombotic properties [9]. Apelin also improves pulmonary hypertension and is a protective factor against acute respiratory distress syndrome (ARDS) [10]. Its circulatory concentration changes in diabetes mellitus, hypertension, metabolic syndrome, and obesity [12,13,14,15,16], the diseases that aggravate the severity of COVID-19 [3, 4, 17].
Given the regulatory roles of apelin/APJ in the cardiovascular system and its relation with ACE2 and COVID-19 patients’ symptoms, which are characteristic of dysregulation of apelin/APJ signaling pathways, such as ARDS, vascular dysfunction, thrombosis, and inflammation [11, 18, 19], this study aimed to evaluate the serum levels of apelin in patients with COVID-19 with and without the underlying diseases of hypertension (HTN), diabetes mellitus (DM), and obesity (OB). Considering that some effects of apelin, such as the antithrombotic and antihypertensive effects, are exerted through the NO signaling pathway, the amount of NO metabolites in the serum of these patients was also evaluated.
Materials and methods
In this case–control study, 69 COVID-19 subjects were selected from patients who were referred to and hospitalized at Afzalipour Hospital in Kerman, Iran, the main referral center in the city, from February to November 2020. Seventy-one non-COV matched subjects were selected from individuals who were ordinary city residents who participated simultaneously in the Kerman coronary artery disease risk factors study (KERCADRS) phase III [20].
COVID-19 infection was confirmed by positive reverse transcription–polymerase chain reaction (RT–PCR). The clinical and lung computed tomographic scan (CT-scan) findings were recorded after admission and interpreted by the physicians. The current smoking history and opium use were recorded by interview. The severity of the COVID-19 disease was almost similar on the first day of admission in all patients when the blood samples were taken. The blood was centrifuged at 4000 g, and serum was stored at − 80 °C.
The hypertensive subjects were those with systolic blood pressures equal to or above 140 mm Hg and/or diastolic blood pressure equal to or above 90 mm Hg or those taking antihypertensive drugs [21]. Those with diabetes mellitus were selected from subjects whose fasting blood sugar was higher than 126 mg/dL or who were taking anti-diabetic drugs [22]. People with a BMI equal to or above 30 kg/m2 were considered obese [23]. The hypertensive and diabetic patients with COVID-19 were chosen based on their history of having these underlying diseases as COVID-19 increases the possibility of hyperglycemia and hypertension after infection [24].
The participants were divided into eight groups: 1—Control (CTL, n = 20), healthy individuals who did not have COVID-19 or any underlying disease, 2—HTN (n = 20), 3—DM (n = 17); 4—OB (n = 15), 5—COVID-19 (COV) (n = 20), patients with COVID-19 who did not have any underlying disease, 6—COV + HTN (n = 17), 7—COV + DM (n = 15), and 8—COV + OB (n = 17). The number of subjects in the groups was chosen according to similar previous studies [25]. The participants’ demographic and initial clinical characteristics are presented in Table 1. We did our best for the corresponding case and control groups to be matched based on sex, age, body mass index (BMI), and history of diabetes, hypertension, and hyperlipidemia.
Measurement of biochemical factors
The level of serum apelin-13 was determined by the enzyme-linked immunosorbent assay (ELISA) method according to the instructions of the kit (Bioassay Technology Laboratory, China). Serum NO content was evaluated by measuring its metabolite nitrate using the Rice calorimetric method. In this method, nitrate is converted to nitrite by vanadium (III) chloride (VaCl3), and the optical density (OD) is measured at 540 nm [26].
Statistical analysis
Data in the tables and figures are presented as median with interquartile range (IQR) for continuous and n (%) for categorical variables. The continuous variables were analyzed using the Mann–Whitney U test for two independent groups (e.g., for the COV with non-COV groups) and the Kruskal–Wallis test for comparison among different study groups (CTL, HTN, DM, OB, COV, COV + HTN, COV + DM, and COV + OB), accompanied by the Mann–Whitney U test. The categorical variables were analyzed using the chi-square test. Multivariable linear regression was used to assess the correlation between duration of hospitalization and arterial O2sat. with apelin levels. The models were adjusted for sex, age, BMI, hypertension, diabetes status, and other covariates. Pearson correlation test was used to assess the association between apelin levels and other variables, such as age, arterial O2 saturation, and NO levels. P values < 0.05 were considered significant.
Results
The demographic data of the studied groups are summarized in Table 1. The sex, age, and hyperlipidemia status of the subjects are matched among the groups. Only HTN groups have significantly higher ages than the CTL group (P < 0.05). The arterial systolic and diastolic blood pressure of the COV, HTN, COV + HTN, COV + DM, and COV + OB groups were higher than the CTL group (P < 0.05 to P < 0.001). However, in the non-HTN groups blood pressure was below the threshold level for hypertension. As expected, BMI in the OB and COV + OB groups was also higher than in the CTL group (P < 0.001). BMI was also higher in the COV + DM and COV + HTN groups than the CTL group (P < 0.01), although it was below the defined level for obesity.
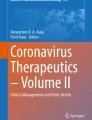
Overall, the apelin levels were significantly lower in COV patients compared to non-COV participants (P < 0.05) (Fig. 1A). They were also lower in patients with COVID-19 without any underlying disease than healthy individuals (P < 0.01). Apelin levels in patients with COV + DM were lower than in the CTL and DM groups (P < 0.05). As apelin levels were already low in the HTN and OB groups, infection with SARS-CoV-2 did not reduce them further (Fig. 1B).

Apelin level in studied groups. Panel A indicates overall apelin level in COV patients compared to non-COV individuals. Analyzed by Mann–Whitney U test. Panel B indicates apelin level based on underlying diseases subgroups, analyzed by Kruskal–Wallis test followed by Mann–Whitney U test. @ P < 0.05 vs. non-COV, *P < 0.05, **P < 0.01, *** P < 0.001 vs. CTL and, #P < 0.05 vs. DM group. CTL control (healthy subjects), HTN hypertension, DM diabetes mellitus, OB obese. n = 15–20 in each group
Overall, nitrite levels (NO metabolite) were significantly lower in COV compared to non-COV subjects (P < 0.05) (Fig. 2A). In addition, in people with non-underlying diseases they were significantly lower in the COV subgroups compared to the non-COV subgroups (P < 0.05). In the COV + OB group, nitrite levels were significantly lower compared to the CTL group (P < 0.05) (Fig. 2B). Furthermore, nitrite levels were lower in the COV + DM group than the DM group (P < 0.05).

Nitrite level in the studied groups. Panel A indicates overall nitrite level in COV patients compared to non-COV individuals analyzed by Mann–Whitney U test. Panel B indicates nitrite level based on underlying diseases subgroups analyzed by Kruskal–Wallis test followed by Mann–Whitney U test. @ P < 0.05 vs. non-COV, *P < 0.05, **P < 0.01, vs. CTL. #P < 0.05 vs. DM group, CTL control (healthy subjects), HTN hypertension, DM diabetes mellitus, OB obese. n = 15–20 in each group
Serum apelin levels in COVID-19 patients were not dependent on sex, smoking status, and opium use (Table 2). The findings also indicated that apelin levels were lower in patients who had more extensive lung involvement, according to their CT scans (P = 0.03) (Table 2).
The association of apelin levels with disease severity according to the length of hospital stay and arterial O2 saturation was analyzed using multivariable linear regression. There was no significant relationship between duration of hospitalization and arterial O2 saturation with age, sex, BMI, DM, and HTN status (Table 3). However, there was a negative linear relationship between serum apelin levels and the length of hospital stay (R2 = 0.078 P = 0.02) (Fig. 3A and Table 3). There was a positive correlation between apelin levels and O2 saturation (R2 = 0.064 P = 0.03) (Fig. 3B and Table 3). The results also showed a positive linear association between serum apelin and nitrite levels in the studied subjects (R2 = 0.089 P = 0.02) (Fig. 3C). A negative association between age and apelin serum levels was also observed (R2 = 0.035 P = 0.048) (Fig. 3D).

Pearson correlation test indicated correlations between serum apelin level with length of hospital stay A and arterial O2 saturation B in COV patients and the level of serum nitrite C and age D in studied groups. O2Sat: arterial O2 saturation
Discussion
The findings of this study showed that the apelin and nitric oxide content was lower than normal in patients with COVID-19 on admission. However, apelin levels were already decreased in patients with underlying risk factors, including hypertension and obesity, and remained low after infection with SARS-CoV-2. The reduction of serum apelin concentration associated with the reduction of O2 Sat. and the extent of lung involvement could partly predict the severity of diseases.
Apelin is a protective peptide in the cardiovascular and respiratory systems, and it exerts its beneficial effects through its receptor, APJ [10]. Apelin and its receptor are present in vascular endothelial cells, including lung blood vessels [10].
Apelin has also been identified as a substrate for ACE2. ACE2 degrades and inactivates some apelin isoforms in a process similar to its primary substrate, Ang-II [19]. Considering that SARS-CoV-2 reduces the amount and/or activity of ACE2 by binding to it, it is predictable that the level of apelin is reduced in COVID-19 patients. This study's findings showed that the serum apelin content was significantly lower in control and diabetic people with COVID-19, and the amount of its reduction levels were positively associated with the hospital duration. Therefore, it is suggested that lower apelin levels may worsen COVID-19 disease complications. Apelin can exert its effect directly by binding to APJ and acting on several signaling pathways in different tissues, including the respiratory and circulation system, and indirectly by enhancement of ACE2 expression [27, 28]. In experimental models of ARDS, apelin inhibits pro-inflammatory cytokine production, reduces inflammation, and improves oxygenation by activation of AKI–eNOS pathways [29]. The lower serum apelin levels found in COV patients in this study can be a result of its degradation by ACE2 as circulatory ACE2 has been shown to be increased in patients with COVID-19 [30]. In an animal model of ARDS, there was a significant decrease in the level of apelin in blood and lung tissue [29], and ACE2 and apelin expressions decreased in cardiomyocytes infected by SARS-CoV-2 [27].
The regulatory role of apelin in ACE2 gene expression has been proven [28]. Apelin enhances the transcription of the ACE2 gene in the rat heart [31] and in cardiomyocytes and adipose tissues of diabetic mice [28]. The enhancement of ACE2 expression could activate the signal pathways of ACE2/Angiotensin-II/Angiotensin-[1,2,3,4,5,6,7], which leads to the diminution of the detrimental effects of Ang-II. Therefore, the use of apelin or its analogs may be recommended for the treatment of COVID-19 patients. The concern is that apelin may increase the rate of SARS-CoV-2 entry into the cells by increasing the expression of ACE2 [8]. However, recent findings have shown that ACE inhibitors and the angiotensin type 1 receptor (AT1R) blockers do not increase the susceptibility to viral infection and the severity of COVID-19 [33]. Currently, these findings are contradictory, and this subject requires further investigation.
Our findings indicated that apelin levels are positively associated with O2 saturation. In contrast, tissue hypoxia and acute systemic hypoxia enhance apelin and APJ expression in the heart, kidney, and brain by inducing hypoxia-inducible factor-1 (HIF-1) and increasing circulating apelin levels in humans and animals [15, 34]. Treatment with apelin decreases the injuries induced by hypoxia in different organs. It seems that in normal conditions increase in apelin production is a compensatory mechanism to counter the harmful effects of hypoxia. However, in diseased conditions, such as COVID-19 infection, more ill people already have a lower level of apelin and lower O2sat.
The results of the present study also revealed that NO levels were lower in COVID-19 patients, as were apelin levels. Some of the effects of apelin, such as vasodilation and anticoagulant effects, are mediated by NO [11, 18]. Therefore, it was not unexpected that the concentration of NO decreased along with the reduction of apelin levels.
The finding that the amount of apelin decreases with increase in age may be consistent with the higher rate of complications and severity of COVID-19 in older patients (because of the reduction in protective effects of apelin). Apelin also has a role in regulating blood glucose by increasing insulin sensitivity [35]. Decreased apelin concentration in COVID-19 patients may be one of the reasons for the disturbances in blood glucose regulation in these patients, even in those who are without diabetes mellitus. The reduction of apelin in subjects with diabetes mellitus can worsen blood glucose regulation in these patients when they are infected with COVID-19. Moreover, our results indicated that in subjects with hypertension and obesity, apelin levels are also lower than normal. That is why obesity and hypertension are also among the comorbidities of COVID-19. These patients are also more likely to get COVID-19 and progress to ARDS when infected with the SARS-CoV-2 virus [3, 36].
We acknowledge that it would have been better if the sample size in each group had been larger. The small sample size was due to the limitations of finding subjects with only one of the underlying diseases while being matched for age, sex, and BMI to reduce the confounding factors that may affect serum apelin levels. In addition, we measured the levels of apelin and NO in subjects who were hospitalized. The levels of mentioned factors may vary in outpatient who had mild type of the disease.
Conclusions
We found lower apelin and nitric oxide levels in patients with hypertension and obesity and in their COVID-19-infected counterparts. Since arterial O2 saturation, hospitalization period, and degree of lung involvement were closely associated with serum apelin levels, this factor may predict the severity of the disease, especially in those with underlying cardiovascular risk factors, such as diabetes mellitus, obesity, and hypertension.
Availability of data and materials
Data will be available on request
Abbreviations
- ACE2:
-
Angiotensin-converting enzyme type
- APLNR:
-
Apelin receptor
- ARDS:
-
Acute respiratory distress syndrome
- AT1R:
-
Angiotensin type 1 receptor
- BMI:
-
Body mass index
- CTL:
-
Control
- CT-scan:
-
Computed tomographic scan
- CVDs:
-
Cardiovascular diseases
- DM:
-
Diabetes mellitus
- ELISA:
-
Enzyme-linked immunosorbent assay
- HIF-1:
-
Hypoxia-inducible factor-1
- HTN:
-
Hypertension
- IQR:
-
Interquartile range
- NO:
-
Nitric oxide
- O2sat:
-
Arterial O2 Saturation
- OB:
-
Obesity
- RAAS:
-
Renin–angiotensin–aldosterone system
- RT–PCR:
-
Reverse transcription–polymerase chain reaction
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- WHO:
-
World health organization
References
Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. Coronavirus investigating, and research team a novel coronavirus from patients with pneumonia in China 2019. N Engl J Med. 2020;382(8):727–33.
Organization WH. Coronavirus disease (COVID-19) pandemic–emergency use listing procedure (EUL) open for in vitro diagnostics. 2020-02-28) [2020-05-21]. https://www.who.int/diagnostics_laboratory/EUL/en. 2020
Batiha GES, Gari A, Elshony N, Shaheen HM, Abubakar MB, Adeyemi SB, et al. Hypertension and its management in COVID-19 patients The assorted view. Int J Cardiol Cardiovasc Risk Prev. 2021;11:200121. https://doi.org/10.1016/j.ijcrp.2021.200121.
Gammone MA, D’Orazio N. COVID-19 and obesity: overlapping of two pandemics. Obes Facts. 2021;14(6):579–85.
GhaffariDarab M, Keshavarz K, Sadeghi E, Shahmohamadi J, Kavosi Z. The economic burden of coronavirus disease 2019 (COVID-19): evidence from Iran. BMC Health Serv Res. 2021;21(1):1–7.
Kuba K, Yamaguchi T, Penninger JM. Angiotensin-converting enzyme 2 (ACE2) in the pathogenesis of ARDS in COVID-19. Front Immunol. 2021;12:1–7.
Lee DK, Cheng R, Nguyen T, Fan T, Kariyawasam AP, Liu Y, et al. Characterization of apelin, the ligand for the APJ receptor. J Neurochem. 2000;74(1):34–41.
Vickers C, Hales P, Kaushik V, Dick L, Gavin J, Tang J, et al. Hydrolysis of biological peptides by human angiotensin-converting enzyme-related carboxypeptidase. J Biol Chem. 2002;277(17):14838–43.
Li L, Xu J, Chen L, Jiang Z. Apelin/APJ system a novel promising therapy target for thrombotic diseases. Clin Chim Acta. 2016;48(April):589–91.
Yan J, Wang A, Cao J, Chen L. Apelin/APJ system: an emerging therapeutic target for respiratory diseases. Cell Mol Life Sci. 2020;77(12):2919.
Liu W, Yan J, Pan W, Tang M. Apelin/Elabela-APJ: a novel therapeutic target in the cardiovascular system. Ann Transl Med. 2020;8(5):243.
Habchi M, Duvillard L, Cottet V, Brindisi MC, Bouillet B, Beacco M, et al. Circulating Apelin is increased in patients with type 1 or type 2 diabetes and is associated with better glycaemic control. Clin Endocrinol (Oxf). 2014;81(5):696–701.
Bellissimo MP, Hsu E, Hao L, Easley K, Martin GS, Ziegler TR, et al. Relationships between plasma apelin and adiponectin with normal weight obesity, body composition, and cardiorespiratory fitness in working adults. J Clin Transl Endocrinol. 2021;24:100257.
Noyan T, Figen CC, Özdemir Ö. The investigation effect of weight loss on serum vaspin, apelin-13, and obestatin levels in obese individual. Turkish J Biochem. 2020;45(6):725–35.
Wysocka MB, Pietraszek-gremplewicz K, Nowak D. The role of apelin in cardiovascular diseases. Obesity and Cancer. 2018;9(May):1–15.
Xie H, Luo G, Zheng Y, Hu D, Peng F, Xie L. Lowered circulating apelin is significantly associated with an increased risk for hypertension a meta-analysis. Clin Exp Hypertens. 2017;00(00):1–6. https://doi.org/10.1080/10641963.2016.1267199.
Xie L, Zhang Z, Wang Q, Chen Y, Lu D, Wu W. COVID-19 and diabetes: a comprehensive review of angiotensin converting enzyme 2 mutual effects and pharmacotherapy. Front Endocrinol. 2021;12(November):1–25.
Khatib A, Lopez JJ, Vatier C, Turpin S, Muscat A, Soulet F, et al. Apelin an antithrombotic factor that inhibits platelet function. Journal Am Soc Hematol. 2016;127(7):908–20.
Kalea AZ, Batlle D. Apelin and ACE2 in cardiovascular disease. Curr Opin Investig Drugs. 2014;11(3):273.
Najafipour H, Mirzazadeh A, Haghdoost AA, Shadkam M, Afshari M, Moazenzadeh M, et al. Coronary artery disease risk factors in an urban and peri-urban setting, Kerman, Southeastern Iran (KERCADR study): methodology and preliminary report. Iran J Public Health. 2012;41(9):86.
Bonow RO, Mann DL, Zipes DP, Libby P. Braunwald’s heart disease-book: a textbook of cardiovascular medicine. Amsterdam: Elsevier Health Sciences; 2011.
Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J. Harrison’s principles of internal medicine. New York: Mcgraw-hill; 2012.
Organization WH. Global database on Body Mass Index: BMI Classification. 2006. World Heal Organ Geneva, Switz. 2015
He X, Liu C, Peng J, Li Z, Li F, Wang J, et al. COVID-19 induces new-onset insulin resistance and lipid metabolic dysregulation via regulation of secreted metabolic factors. Signal Transduct Target Ther. 2021;6(1):427.
Liakos CI, Sanidas EA, Perrea DN, Grassos CA, Chantziara V, Viniou N-A, et al. Apelin and visfatin plasma levels in healthy individuals with high normal blood pressure. Am J Hypertens. 2016;29(5):549–52.
Yucel AA, Gulen S, Dincer S, Yucel AE, Yetkin GI. Comparison of two different applications of the griess method for nitric oxide measurement. J Exp Integr Med. 2012;2:1.
Li X-T, Zhang M-W, Zhang Z-Z, Cao Y-D, Liu X-Y, Miao R, et al. Abnormal apelin-ACE2 and SGLT2 signaling contribute to adverse cardiorenal injury in patients with COVID-19. Int J Cardiol. 2021;336:123–9.
Sabry MM, Mahmoud MM, Shoukry HS, Rashed L, Kamar SS, Ahmed MM. Interactive effects of apelin, renin–angiotensin system and nitric oxide in treatment of obesity-induced type 2 diabetes mellitus in male albino rats. Arch Physiol Biochem. 2019;125(3):244–54.
Physiology C. Apelin-13 administration protects against LPS-induced acute lung injury by inhibiting NF-κB pathway and NLRP3 inflammasome activation. Cell Physiol Biochem. 2018;49:1918–32.
Reindl-Schwaighofer R, Hödlmoser S, Eskandary F, Poglitsch M, Bonderman D, Strassl R, et al. ACE2 elevation in severe COVID-19. Am J Respir Crit Care Med. 2021;203(9):1191–6.
Sato T, Sato C, Kadowaki A, Watanabe H, Ho L, Ishida J, et al. ELABELA-APJ axis protects from pressure overload heart failure and angiotensin II-induced cardiac damage. Cardiovasc Res. 2017;113(7):760–9.
Gheblawi M, Wang K, Viveiros A, Nguyen Q, Zhong J-C, Turner AJ, et al. Angiotensin-converting enzyme 2: SARS-CoV-2 receptor and regulator of the renin-angiotensin system: celebrating the 20th anniversary of the discovery of ACE2. Circ Res. 2020;126(10):1456–74.
Mehta N, Kalra A, Nowacki AS, Anjewierden S, Han Z, Bhat P, et al. Association of use of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers with testing positive for coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(9):1020–6.
Heinonen I, Vuolteenaho O, Koskenvuo J, Arjamaa O, Nikinmaa M. Systemic hypoxia increases circulating concentration of apelin in humans. High Alt Med Biol. 2017;18(3):292–5.
Alipour FG, Ashoori MR, Pilehvar-Soltanahmadi Y, Zarghami N. An overview on biological functions and emerging therapeutic roles of apelin in diabetes mellitus. Diabetes Metab Syndr Clin Res Rev. 2017;11:S919–23.
Demeulemeester F, de Punder K, van Heijningen M, van Doesburg F. Obesity as a risk factor for severe covid-19 and complications a review. Cells. 2021;10(4):933.
Funding
This work was supported by grants from the Iranian national science foundation-INSF (Grant NO. 99009916), and Vice-Chancellor for Research and Technology at Kerman University of Medical Sciences, Kerman, Iran (Grant No. IR.KMU.REC.1399000764).
Author information
Authors and Affiliations
Contributions
FR and HN designed the research. AAL selected the COVID-19 patients, collected their blood samples and sera. RY and SN recorded the clinical and CT-scan findings. FR analyzed the data and wrote the manuscript in collaboration with HN. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics committee of Kerman University of Medical Sciences approved the experimental protocol (Permission Code No: IR.KMU.REC.1399.586). All patients signed written informed consent to participate in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rostamzadeh, F., Najafipour, H., Yazdani, R. et al. Changes in serum levels of apelin and nitric oxide in hospitalized patients with COVID-19: association with hypertension, diabetes, obesity, and severity of disease. Eur J Med Res 27, 243 (2022). https://doi.org/10.1186/s40001-022-00852-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-022-00852-3