
Abstract
Background
Antimicrobial resistance has emerged as a major threat to global public health. Thus, the surveillance of changes in antimicrobial resistance in local and global settings is a paramount necessity. While many studies have tracked antimicrobial resistance, only a small percentage surveyed ocular isolates. The purpose of this study was to report the in vitro susceptibility of bacterial pathogens isolated from ocular samples in New York, NY from 2010 to 2015.
Methods
A retrospective review of ocular isolates was conducted. All organisms were collected by 25 separate inpatient wards and outpatient clinics, and were analyzed by the clinical microbiology laboratory at Mount Sinai Hospital. Clinical Laboratory and Standards Institute (CLSI) guidelines were followed for susceptibility testing and breakpoint interpretations.
Results
A total of 549 bacterial organisms were isolated from 1664 cultures (33%) during the 6-year study period. Of these, 358 isolates (65.2%) underwent susceptibility testing. 182 (50.8%) isolates were Gram-positive. The most common Gram-positive bacterium was Staphylococcus aureus (62.1%). Methicillin-resistance decreased in S. aureus isolates (31.3% in 2010, 14.1% in 2015) but was without significant change (p = 0.25). When analyzing all S. aureus isolates recovered during the study period, there were significantly more methicillin-resistant S. aureus (MRSA) isolates resistant to fluoroquinolones (p <0.0001), erythromycin (p <0.0001), and trimethoprim/sulfamethoxazole (TMP/SMZ; p <0.05). Overall, Streptococcus pneumoniae isolates showed reduced susceptibility to erythromycin, but were otherwise susceptible to the other antimicrobials tested. Haemophilus influenzae (26.1%) and Pseudomonas aeruginosa (23.9%) were the most common Gram-negative bacteria isolated. Resistance to ampicillin and TMP/SMZ was observed in several of the H. influenzae isolates. P. aeruginosa isolates did not show high resistance overall, however, it was noted that isolates resistant to meropenem were also resistant to other antimicrobials (p < 0.01).
Conclusion
Overall, antimicrobial resistance was infrequent for the Gram-negative and Gram-positive bacteria analyzed. While the MRSA isolates demonstrated increased resistance to multiple antimicrobial classes, this is expected for this pathogen. Due to the continued use of broad-spectrum oral and systemic antimicrobials to treat ocular infections, findings of this study and other surveillance studies specific to ocular isolates should be used as resources in effective decision making in the treatment of ocular disease.
Similar content being viewed by others


Background
Antimicrobial resistance is an issue that has been impacting medicine for many years. Whether in primary care or specialized care settings, antimicrobial resistance has been on the rise and has affected the way healthcare providers treat bacterial infections. Particularly in ophthalmic settings, physicians tend to treat ocular infections by prescribing empiric antibiotics because they often do not have data from culture analysis. As a result, there is a lack of awareness of fluctuating trends in antimicrobial resistance of many common pathogens [1,2,3,4]. This is an important concern, especially due to the fact that many ocular pathogens, if shown to possess multi-drug resistance (MDR), i.e. non-susceptibility to at least one agent in three or more antimicrobial classes [5], can be difficult to treat, which increases the chances of severe ocular damage and vision loss [3, 6, 7].
Generally, broad-spectrum antibiotics are used to treat many ocular infections, including microbial keratitis, conjunctivitis, and endophthalmitis; however, the pathogenic organisms that cause these conditions have shown increased resistance to antibiotics over the past decade. For example, Staphylococcus species and Pseudomonas aeruginosa have demonstrated resistance to fluoroquinolones, macrolides, and β-lactams [2, 3, 6, 8]. Haemophilus influenzae, a common Gram-negative bacterium, has also shown increased resistance to trimethoprim [9,10,11,12].
There have been a few nationwide surveillance studies, such as Ocular TRUST and ARMOR, which have tracked resistance patterns in many common ocular pathogens [9, 13]. However, given the growing importance of this issue, there is also a need for smaller, regional studies to obtain local data. Many such single-center studies have been surveying and tracking antimicrobial resistance in order to establish effective treatment methods against ocular infections on a local level [6,15,16,17,18,, 14–19]. The goal of this retrospective study was to determine resistance patterns in ocular pathogens isolated and analyzed by the Mount Sinai Hospital clinical microbiology laboratory in New York, NY and contribute our findings to the growing knowledge base regarding antimicrobial resistance of ocular pathogens. In turn, these findings can also help influence intelligent and effective antibiotic use in the New York City metropolitan area, with the potential to help develop informed treatment protocols against common ocular pathogens.
Methods
A retrospective, consecutive data review study was conducted. The study was approved by the institutional review board of Mount Sinai Hospital and the tenets of the Declaration of Helsinki were followed.
Collection of ocular isolates
A total of 1664 ocular cultures were performed from over 25 separate inpatient wards and outpatient clinics over a 6-year period (January 2010 to December 2015). The clinical microbiology laboratory at Mount Sinai Hospital performed all cultures and antimicrobial susceptibility testing for these facilities. For the purposes of this review, only specimens that tested positive for a bacterial organism were included in the study. Fungal isolates were not analyzed.
Eye culture workup and organism identification
Eye culture specimens (swabs of various ocular anatomic sites, corneal scrapings, and vitreous/aqueous fluids) were either directly plated to agar at the time of collection or sent to the clinical microbiology laboratory for plating. The routine culture media used for eye cultures included blood agar, chocolate agar, and CDC anaerobe 5% sheep blood agar. Providers collecting specimens at the bedside would also frequently add a thioglycollate broth during collection. All media was incubated aerobically in a 5% CO2 environment or under anaerobic conditions at 35–37 °C per laboratory standard operating protocols. Positive cultures were determined by the laboratory’s standard operating protocol. For specimens that were directly plated (isolated from corneal scrapings or vitreous fluids), the organism had to be localized to the area of the plate where the specimen was planted. For those specimens collected with a swab, the organism had to be localized in the first quadrant (first streak area) of the plate. If growth was observed in the 2nd, 3rd, or 4th area, consultation with the microbiology director typically resulted in the organism being labeled as a contaminant.
Significant ocular pathogens were primarily identified using routine biochemical testing and the VITEK-2 instrument (bioMérieux, Inc., Durham, NC). If the VITEK-2 result failed, alternate identification systems used by the laboratory included API strips (bioMérieux, Inc., Durham, NC) and the rapID identification system (Remel, Lenexa, KS).
Susceptibility testing
All susceptibility testing was performed in the Mount Sinai Hospital clinical microbiology laboratory. A total of 358 isolates underwent susceptibility testing from a total of 549 isolated bacterial isolates. Only significant ocular pathogens as defined by the laboratory standard operating protocol underwent susceptibility testing. Organisms identified that were believed to be contaminants or normal flora (i.e. Coagulase-negative Staphylococcus and Corynebacterium species) were excluded from analysis since susceptibility testing was not performed. This included 152 coagulase-negative Staphylococcus (CoNS) isolates that were collected during the 6-year period. Providers always had the opportunity to call the laboratory and request susceptibility testing on these isolates if they deemed them significant. The panel of antimicrobials tested was determined by the microbiology director and antimicrobial stewardship based on the institution’s antibiotic formulary. The primary susceptibility testing method used in the laboratory during the study was VITEK-2 (bioMérieux, Inc., Durham, NC), which was performed per manufacturer’s recommendations. Streptococcus species, infrequently isolated, and fastidious organisms were tested by E-test (bioMérieux Inc., Durham, NC) per manufacturer’s recommendations. Interpretations (susceptible, intermediate, susceptible dose-dependent, or resistant) were determined using Clinical Laboratories and Standards Institute (CLSI) guidelines (M100 [20] or M45 [21] documents) relevant to the year the organism was tested.
Data organization & inclusion procedures
All data was collected from the Laboratory Information System used by the Mount Sinai Hospital clinical microbiology laboratory. The data was imported into a Microsoft Excel spreadsheet file and all important patient identifiers were properly and securely discarded in accordance with IRB guidelines. The data imported included date of collection, age of patient, ward, collection site, organism isolated and MIC values against a variety of antibiotics. Only isolates that underwent susceptibility testing were included in this study. Susceptibility profiles are shown for microbial species that were tested at least 30 times during the study period with the exception of MRSA (n = 28), though not all antimicrobials were tested against each isolate. MIC50 and MIC90 values were also calculated.
Statistical analysis
Statistical analysis was conducted using the program Prism (software version 7.0a; GraphPad software). A Fisher’s exact test was used to study the prevalence of methicillin-resistance amongst all Staphylococcus aureus isolates during the study period as well as to compare differences in resistance between methicillin-resistant Staphylococcus aureus (MRSA) and methicillin-susceptible Staphylococcus aureus (MSSA) isolates. Comparisons amongst S. aureus and age of infection were conducted using a Chi-Squared test. Statistical significance was defined as p < 0.05.
Results
Of a total of 1664 cultures performed during the study period, 549 bacterial organisms were isolated. Of these, 358 ocular pathogens (65.2%) underwent susceptibility testing, which included 113 S. aureus, 30 S. pneumoniae, 42 P. aeruginosa, & 46 H. influenzae isolates (Table 1). Of the 358 isolates, 41 (11.5%), 30 (8.4%), 11 (3.1%), 17 (4.7%), and 3 (0.8%) samples were isolated from the conjunctiva, cornea, eyelid, contact lens, and vitreous fluid respectively. The remaining 256 (71.5%) samples were collected from unspecified ocular sites. Gram-positive bacteria accounted for 50.8% of the total isolates. S. aureus was the most common Gram-positive bacterium [113 of 182 (62.1%)] while H. influenzae was the most common Gram-negative bacterium [46 of 176 (26.1%)]. Comparison by patient age, in years, (Table 2) shows that the amount of Gram-positive organisms (S. aureus, coagulase-negative Staphylococcus (CoNS), and S. pneumoniae isolates) was higher in the elderly group (>65 years) than in any other group and increased in an age-dependent manner. MRSA infections were statistically more likely to occur in the two oldest age groups, i.e. >40 years, when compared to the younger age groups (p < 0.05). Gram-negative organisms, with the exception of H. influenzae, were more prevalent in the middle-aged groups, i.e. 18–64 years. Interestingly, H. influenzae isolates were more prevalent in the youngest and oldest age groups, presenting a bimodal distribution.
Staphylococcus aureus
MRSA
Over the 6-year period that was evaluated, the prevalence of methicillin-resistant S. aureus showed a decreasing yet statistically insignificant trend (Fig. 1), with 31.30% resistance in 2010 compared to 14.30% resistance in isolates collected in 2015 (p = .25).

Prevalence of MRSA from 2010–2015. An overall decreasing trend in MRSA prevalence is observed from 2010–2015. However, the trend is not statistically significant (p = 0.25).
A total of 28 cultures tested positive for methicillin-resistant S. aureus (Table 3a). MRSA isolates exhibited high resistance against erythromycin (89.29%), clindamycin (35.7%), levofloxacin (50%), and ciprofloxacin (80%) and high susceptibility to the remainder of the antimicrobials tested. No MRSA isolates showed resistance to vancomycin, daptomycin or linezolid.
MSSA
A total of 85 cultures tested positive for methicillin-susceptible S. aureus (Table 3a). MSSA isolates exhibited high susceptibility to the majority of antimicrobials tested with the exception of clindamycin (34.12%) and erythromycin (44.05%). No isolates were found to be resistant to vancomycin, daptomycin, gentamicin, or linezolid. Unlike MRSA, MSSA isolates were highly susceptible to levofloxacin and ciprofloxacin.
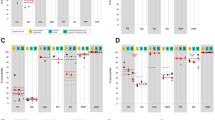
Resistance in MRSA and MSSA was also compared (Fig. 2). As expected, the resistance observed against ciprofloxacin (p <0.0001), erythromycin (p <0.0001), levofloxacin (p <0.0001), and TMP/SMZ (p <0.05) was significantly higher for the MRSA isolates compared to the MSSA isolates. This increased resistance is also seen in the MIC50/MIC90 values, in which MRSA had equal or higher MIC50/MIC90 values than MSSA in response to ciprofloxacin, erythromycin, levofloxacin, and TMP/SMZ.

Antimicrobial Resistance Observed in MRSA & MSSA Isolates. Significant differences in antimicrobial resistance between MRSA & MSSA isolates were observed for ciprofloxacin, erythromycin, levofloxacin, and TMP/SMZ. Note: Daptomycin, vancomycin, and linezolid are not included because no resistance was shown for either MRSA or MSSA isolates. Abbreviations: MSSA = methicillin-susceptible Staphylococcus aureus; MRSA = methicillin-resistant Staphylococcus aureus; TMP/SMZ = trimethoprim/sulfamethoxazole; **** = (p < .0001); * = (p < .05)
Streptococcus pneumoniae
A total of 30 cultures tested positive for S. pneumoniae (Table 3b). Overall, S. pneumoniae isolates exhibited relatively low resistance to all of the antimicrobials tested against them. This is further supported by the low MIC50 and MIC90 values for these antimicrobials. Only erythromycin showed moderate resistance, in which five of the isolates (16.67%) were resistant, as well as a large MIC range from .016 to 32 ug/ml. Vancomycin, clindamycin, and levofloxacin remained effective against S. pneumoniae, with each antimicrobial generating over 93% susceptibility.
Pseudomonas aeruginosa
A total of 42 cultures tested positive for P. aeruginosa (Table 4a). The majority of antimicrobials were greater than 90% effective against P. aeruginosa with the exception of both meropenem and piperacillin/tazobactam (11.91 and 12.20% resistance respectively). The five isolates that were resistant to meropenem were more likely to be resistant to other classes of antimicrobials (p = 0.008), including aminoglycosides and fluoroquinolones.
Haemophilus influenzae
A total of 46 cultures tested positive for H. influenzae (Table 4b). The vast majority of isolates were susceptible to most of the antimicrobials tested with the exception of TMP/SMZ and ampicillin, both of which showed high MIC90 values. All isolates were tested against TMP/SMZ, with 17 (37%) isolates showing resistance. Of the 33 isolates tested against ampicillin, 10 (30.30%) were resistant.
Discussion
In this retrospective review, 358 microorganisms were analyzed by a single-center institution over a 6-year study period. A wide variety of Gram-positive and Gram-negative organisms were collected including CoNS, S. marcescens, K. oxytoca, and E. coli, as well as more common bacterial pathogens such as S. aureus, S. pneumoniae, H. influenzae, and P. aeruginosa. In this study the number of Gram-negative organisms (49.2%) was nearly equal to the number of Gram-positive organisms (50.8%). While other single-center studies have found a much higher proportion of Gram-positive organisms in collected samples [1,23,, 7, 18, 22–24], this study exhibited a nearly equivalent Gram-positive to Gram-negative ratio. This difference is likely due to the clinical microbiology laboratory protocols that did not require susceptibility testing of CoNS until mid-2015 from eye sources due to the likelihood of these isolates being contaminants. Specifically, there were an additional 152 CoNS isolates, the majority isolated from conjunctival swabs, which did not undergo susceptibility testing. If these isolates had undergone susceptibility testing, the distribution between Gram-positive and Gram-negative bacteria would change considerably (65.5 and 34.5% respectively) and be more in line with previously published studies.
This study also showed an uneven distribution of ocular isolates among age groups. Gram-positive organisms were most common in the elderly, while Gram-negative organisms, except H. influenzae, were most common in the middle age ranges. H. influenzae isolates had a bimodal distribution, being more common in the youngest and oldest age groups. Additionally MRSA was statistically more likely (p < 0.05) to be found in the two oldest age groups (40–64 years and >65 years) when compared to the younger age groups suggesting a higher possibility of MRSA infection with increasing age. While the link between age and risk of infection remains unclear, it may be due to the underdeveloped immune system common in infants and children as well as the depressed immune function observed in the elderly, making the risk of microbial infection in these groups higher [25].
Several drugs are used to treat ocular infections, each with a different mechanism of action. Despite this, many of the pathogens observed in this study are adapting in ways that lead to increased resistance to several classes of antibiotics. Fluoroquinolones, which are a class of drugs often used as first-line treatment for ocular infections, have generally been successful, especially as newer generations have been introduced [1, 22]. However, just like other antimicrobial classes, the systemic use of these fluoroquinolones as first-line broad-spectrum antibiotics tends to lead to increases in resistance due to selective pressure [4, 15, 16, 19]. In this study, 50 and 80% of MRSA isolates showed resistance to levofloxacin and ciprofloxacin respectively, while 3.53 and 7.41% of MSSA isolates showed resistance to levofloxacin and ciprofloxacin, respectively.
Multi-drug resistance (MDR) was observed in many of the MRSA isolates collected in this study (n = 12; 42.9%). When compared to MSSA isolates, MRSA isolates have shown statistically significant increases in MDR when compared to MSSA isolates, making them resilient pathogens. However, even with this increased resistance, S. aureus isolates have shown limited to no resistance to vancomycin, daptomycin or linezolid, making these treatments reliably effective in bacterial populations that have already shown high resistance to fluoroquinolones, aminoglycosides, and macrolides.
Fluctuating trends in the prevalence of MRSA strains have been reported. Some studies have presented increasing trends in MRSA over extended periods of time [23, 24], while others, including those presented by the CDC, state a decline in MRSA prevalence [26,27,28]. This study shows a non-statistically significant, decreasing trend over the 6-year study period suggesting that MRSA prevalence has not fluctuated drastically over the last several years. While it is unclear why MRSA prevalence has remained relatively stable in our review, it may result from successful infection control strategies in both hospitals and surrounding communities, or perhaps the cyclical replacement of dominant, infective MRSA strains by MSSA strains over time [27].
In contrast to MRSA, resistance among S. pneumoniae and P. aeruginosa isolates was low against the antimicrobials tested while resistance among H. influenzae isolates was evident primarily against ampicillin and TMP/SMZ. Overall these three organisms did not show alarming resistance to the antimicrobials tested and are consistent with other antimicrobial surveillance studies that have been conducted recently [1, 7, 13, 19].
Several factors are important in the development of antimicrobial resistance in ocular isolates. Overuse of antibiotics is one of the main causes [16]. Other causes include use of an antibiotic when it is not warranted, as in the case of a viral infection, or improper use, such as stopping a course of antibiotics early or using them prophylactically [17]. Since most ocular infections are often resolved through topical application rather than through systemic use, the inherent pharmacokinetic differences between the two must be taken into account when evaluating antimicrobial resistance [29, 30]. Given the high risk of permanent vision loss with eye infection, such as corneal ulcers and endopthalmitis, topical antibiotics tend to be at higher concentrations and are often used as prophylaxis despite limited evidence on their efficacy. The role that topical antibiotics play in antimicrobial resistance is still ambiguous due to the lack of research in this specific area as well as the lack of standardized ocular tissue-specific breakpoints. With the lack of these breakpoints to qualify resistance, CLSI breakpoints have been agreed upon by many researchers as useful indicators of resistance in topical antibiotics and even with the differences mentioned, similar resistance trends are observed in both topical and systemic antibiotic use [31, 32]. Additionally, since systemic antibiotics are still used to treat chronic ocular infections, in such usage, CLSI breakpoints are appropriate. In fact, systemic use of antibiotics may be the key cause of resistance in all isolates, regardless of the source of infection [33, 34]. However, the uncertainty of the role of topical antibiotics is still apparent and therefore requires further attention in order to fully delineate their role.
Limitations of this study include the retrospective nature of this study, which predetermined our sample size, ultimately limiting our analysis of all possible antimicrobial resistance trends. Because there was no standardized protocol for collection of isolates, inevitably there was a large variation in the culturing procedure among physicians. This lack of uniformity may have affected organism recovery in culture. Additionally, the antimicrobial panel underwent small fluctuations from year to year leading to slightly inconsistent susceptibility testing and excluded testing on more recently introduced fluoroquinolones, such as gatifloxacin.
Conclusion
This 6-year retrospective study reported the numbers of common ocular bacterial isolates and their susceptibility profiles. The study demonstrated a relatively even ratio of Gram-negative to Gram-positive organisms and a variable distribution amongst age groups, depending on the organism. This study also found increased resistance to other drugs among MRSA strains when compared to MSSA strains, as well as moderately low resistance in Gram-negative organisms. Future studies should include a panel of commonly used antimicrobials for ocular infections, including more recently introduced fluoroquinolones. To prevent further progression of resistance, findings of this study and other surveillance data on ocular isolates should be used as resources in effective decision making in the treatment of ocular disease and infection.
Abbreviations
- ARMOR:
-
Antibiotic Resistant Monitoring in Ocular Microorganisms
- CDC:
-
Center for Disease Control
- CLSI:
-
Clinical Laboratory & Standards Institute
- CoNS:
-
Coagulase-Negative Staphylococcus
- MRSA:
-
Methicillin-resistant S. aureus
- MSSA:
-
Methicillin-Susceptible S. aureus
- TMP/SMZ:
-
Trimethoprim-Sulfamethoxazole
- TRUST:
-
Tracking Resistance in U.S. Today
References
Sand D, et al. Microbial keratitis in los angeles: the doheny eye institute and the los angeles county hospital experience. Ophthalmology. 2015;122(5):918–24.
Vazirani J, Wurity S, Ali MH. Multidrug-resistant pseudomonas aeruginosa keratitis: risk factors, clinical characteristics, and outcomes. Ophthalmology. 2015;122(10):2110–4.
Oldenburg CE, et al. Emerging moxifloxacin resistance in Pseudomonas aeruginosa keratitis isolates in South India. Ophthalmic Epidemiol. 2013;20(3):155–8.
Paul-Satyaseela M, et al. Characterization of antibiotic resistance profiles of ocular enterobacteriaceae isolates. Eur J Microbiol Immunol (Bp). 2016;6(1):40–8.
Magiorakos AP, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infection. 2012;18(3):268–81.
Fernandes M, et al. Extensively and pan-drug resistant Pseudomonas aeruginosa keratitis: clinical features, risk factors, and outcome. Graefes Arch Clin Exp Ophthalmol. 2016;254(2):315–22.
Muluye D, et al. Types and drug susceptibility patterns of bacterial isolates from eye discharge samples at Gondar university hospital, northwest Ethiopia. BMC Res Notes. 2014;7:292.
Haas W, et al. Monitoring antibiotic resistance in ocular microorganisms: results from the antibiotic resistance monitoring in ocular micRorganisms (ARMOR) 2009 surveillance study. Am J Ophthalmol. 2011;152(4):567–74. e3.
Asbell PA, et al. Ocular TRUST: nationwide antimicrobial susceptibility patterns in ocular isolates. Am J Ophthalmol. 2008;145(6):951–8.
Thornsberry C, et al. Regional trends in antimicrobial resistance among clinical isolates of streptococcus pneumoniae, haemophilus influenzae, and moraxella catarrhalis in the united states: results from the TRUST surveillance program, 1999–2000. Clin Infect Dis. 2002;34 Suppl 1:S4–S16.
Karlowsky JA, et al. Susceptibility to fluoroquinolones among commonly isolated gram-negative bacilli in 2000: TRUST and TSN data for the united states. Tracking resistance in the united states today. The surveillance network. Int J Antimicrob Agents. 2002;19(1):21–31.
Sahm DF, et al. Tracking resistance among bacterial respiratory tract pathogens: summary of findings of the TRUST surveillance initiative, 2001–2005. Postgrad Med. 2008;120(3 Suppl 1):8–15.
Asbell PA, et al. Antibiotic resistance among ocular pathogens in the united states: five-year results from the antibiotic resistance monitoring in ocular microorganisms (ARMOR) surveillance study. JAMA Ophthalmol. 2015;133(12):1445–54.
McDonald M, Blondeau JM. Emerging antibiotic resistance in ocular infections and the role of fluoroquinolones. J Cataract Refract Surg. 2010;36(9):1588–498.
Gentile RC, et al. Microbiological spectrum and antibiotic sensitivity in endophthalmitis: a 25-years review. Ophthalmology. 2014;121(8):1634–42.
Blanco AR, et al. Susceptibility of methicillin-resistant Staphylococci clinical isolates to netilmicin and other antibiotics commonly used in ophthalmic therapy. Curr Eye Res. 2013;38(8):811–6.
Willcox MD. Review of resistance of ocular isolates of Pseudomonas aeruginosa and staphylococci from keratitis to ciprofloxacin, gentamicin and cephalosporins. Clin Exp Optom. 2011;94(2):161–8.
Ong SJ, et al. Staphylococcus aureus keratitis: a review of hospital cases. PLoS One. 2013;8(11):e80119.
Al-Dhaheri HS, et al. Ocular pathogens and antibiotic sensitivity in bacterial keratitis isolates at king khaled Eye specialist hospital, 2011 to 2014. Cornea. 2016;35(6):789–94.
Clinical Laboratory and Standards Institute. Performance standards for antimicrobial susceptibility testing, in M100. 2010–2016.
Clinical Laboratory Standards Institute. Methods for antimicrobial dilution and disk susceptibility testing of infrequently isolated fastidious bacteria, M45 S2. 2nd ed. 2011.
Mantadakis E, et al. Antimicrobial susceptibility of Gram-positive cocci isolated from patients with conjunctivitis and keratitis in Crete, Greece. J Microbiol Immunol Infect. 2013;46(1):41–7.
Asbell PA, et al. Increasing prevalence of methicillin resistance in serious ocular infections caused by Staphylococcus aureus in the United States: 2000 to 2005. J Cataract Refract Surg. 2008;34(5):814–8.
Adebayo A, et al. Shifting trends in in vitro antibiotic susceptibilities for common bacterial conjunctival isolates in the last decade at the New York Eye and Ear Infirmary. Graefes Arch Clin Exp Ophthalmol. 2011;249(1):111–9.
Kale SS, Namita A, Sachin Y. The epidemiology of aging, Aging, infection, and immunity. Netherlands: Springer; 2012.
Chuang CC, et al. Staphylococcus aureus ocular infection: methicillin-resistance, clinical features, and antibiotic susceptibilities. PLoS One. 2012;8(8):e42437.
Rolain JM, et al. Worldwide decrease in methicillin-resistant Staphylococcus aureus: do we understand something? Clin Microbiol Infect. 2015;21(6):515–7.
Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. Atlanta: CDC; 2013.
Bertino Jr JS. Impact of antibiotic resistance in the management of ocular infections: the role of current and future antibiotics. Clin Ophthalmol. 2009;3:507–21.
Sharma S. Antibiotic resistance in ocular bacterial pathogens. Indian J Med Microbiol. 2011;29(3):218–22.
Parmar P, et al. Comparison of topical gatifloxacin 0.3% and ciprofloxacin 0.3% for the treatment of bacterial keratitis. Am J Ophthalmol. 2006;141(2):282–6.
Kaliamurthy J, et al. Comparison of in vitro susceptibilities of ocular bacterial isolates to gatifloxacin and other topical antibiotics. Ophthalmic Res. 2005;37(3):117–22.
Ray KJ, et al. Fluoroquinolone treatment and susceptibility of isolates from bacterial keratitis. JAMA Ophthalmol. 2013;131(3):310–3.
Rameshkumar G, et al. Prevalence and antibacterial resistance patterns of extended-spectrum beta-lactamase producing Gram-negative bacteria isolated from ocular infections. Indian J Ophthalmol. 2016;64(4):303–11.
Acknowledgements
The authors would like to acknowledge the kind and invaluable assistance of the Pathology Department of the Icahn School of Medicine at Mount Sinai, as well as Dhiraj Patel, a student at Stuyvesant High School, New York, NY.
Funding
No funding was obtained from any sources in order to conduct this study.
Availability of data and materials
The raw datasets analyzed during the current study period can be made available by the authors of this article upon reasonable request.
Authors’ contributions
MO, TD, CH, & PA were responsible for the study design. MO and TD collected and analyzed the data incorporated into this review. CG contributed to the drafting of the manuscript. All authors have read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for Publication
Not applicable.
Ethics approval and consent to participate
This study was approved by the Institutional Review Board at the Icahn School of Medicine at Mount Sinai. Collection of informed consent was waived due to the retrospective nature of the study. This research was in compliance with the Helsinki Declaration.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Oydanich, M., Dingle, T.C., Hamula, C.L. et al. Retrospective report of antimicrobial susceptibility observed in bacterial pathogens isolated from ocular samples at Mount Sinai Hospital, 2010 to 2015. Antimicrob Resist Infect Control 6, 29 (2017). https://doi.org/10.1186/s13756-017-0185-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13756-017-0185-0